What investigation should be done to ascertain the cause of secondary hypertension
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
I now have all the information needed for a thorough, well-structured response. Here is the comprehensive answer:
Investigations for Secondary Hypertension
Secondary hypertension is defined as elevated blood pressure resulting from an identifiable, often correctable, underlying cause. It should be considered in every newly diagnosed hypertensive patient and especially when there is: treatment-resistant hypertension, abrupt worsening of previously controlled BP, unprovoked hypokalemia, disproportionate target organ damage, new onset <30 years of age (without family history), or a BP rise after age 55.
(Frameworks for Internal Medicine; Harrison's Principles of Internal Medicine 22E; Brenner and Rector's The Kidney)
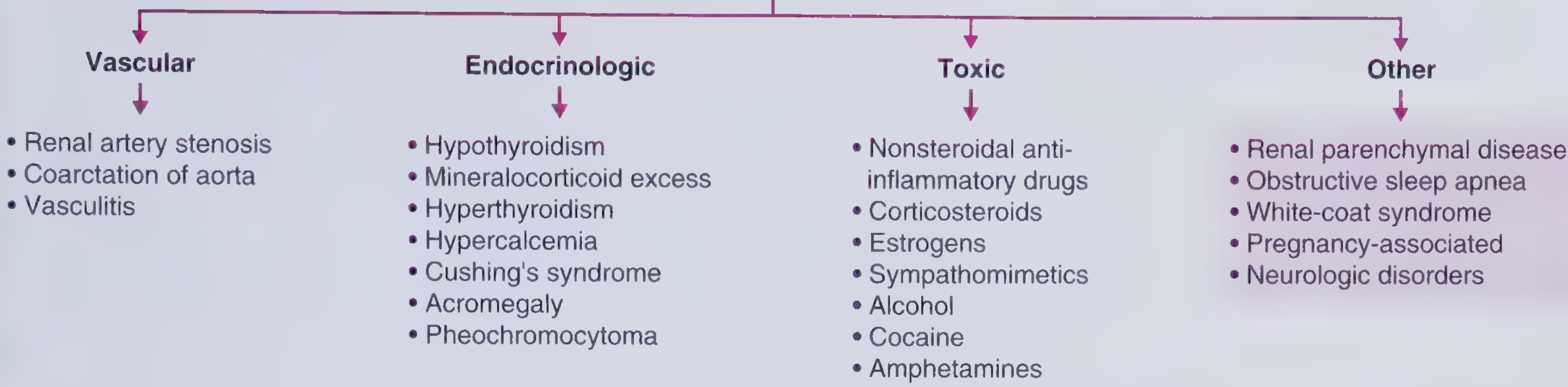
Causes of Secondary Hypertension (Categorized)
Step 1: Basic Screening Investigations (All Newly Diagnosed Patients)
These tests are recommended for every hypertensive patient to identify common secondary causes and assess end-organ damage:
| Test | Purpose |
|---|---|
| Serum urea and creatinine | Identify CKD/renal parenchymal disease |
| Urinalysis (dipstick + microscopy) | Proteinuria, hematuria - suggests renal disease |
| Serum electrolytes (Na+, K+) | Hypokalemia - raises suspicion for primary hyperaldosteronism |
| Fasting blood glucose / HbA1c | Diabetic nephropathy workup |
| Serum TSH (thyroid stimulating hormone) | Hypothyroidism or hyperthyroidism as a cause |
| Fasting lipid profile | Cardiovascular risk assessment |
| Full blood count | Baseline |
| ECG | Left ventricular hypertrophy (target organ damage) |
| Renal ultrasound | Renal size, asymmetry, obstruction, parenchymal disease |
Step 2: Targeted Investigations by Suspected Cause
1. Primary Hyperaldosteronism (Conn's Syndrome) - Most Common Cause
Present in up to 10% of hypertensive patients. Classic features: hypokalemia, mild hypernatremia, metabolic alkalosis (though not always present).
- Screening: Plasma aldosterone-to-plasma renin activity (ARR) ratio
- ARR >30 (aldosterone in ng/dL, renin activity in ng/mL/hr) is strongly suggestive
- Confirmatory: Salt loading test, fludrocortisone suppression test, saline infusion test
- Localisation: CT adrenal glands; adrenal vein sampling (AVS) to distinguish unilateral adenoma from bilateral hyperplasia
(Frameworks for Internal Medicine, p. 521; Brenner and Rector's The Kidney)
2. Renovascular Hypertension (Renal Artery Stenosis)
Consider in: young women (fibromuscular dysplasia), elderly smokers (atherosclerosis), patients with abdominal bruit, acute creatinine rise ≥30% after starting ACE inhibitor/ARB, recurrent flash pulmonary edema.
- Screening:
- Renal duplex ultrasonography (non-invasive, first-line)
- CT renal angiography (CTA)
- MR renal angiography (MRA) - preferred in renal impairment
- Gold standard confirmatory: Conventional renal angiography (catheter-based)
- Functional tests: Captopril renography (less commonly used today)
(Frameworks for Internal Medicine - "string of beads" appearance on angiography is characteristic of fibromuscular dysplasia)
3. Pheochromocytoma / Paraganglioma
Classic triad: episodic headache, sweating, palpitations. Present in 0.1-0.6% of hypertensives. Paroxysmal hypertension in ~25-30% of cases.
- Biochemical (first-line):
- Plasma fractionated metanephrines (normetanephrine + metanephrine) - most sensitive test (>90% sensitivity)
- 24-hour urine fractionated metanephrines and catecholamines - also >90% sensitive
- Elevations >3x upper limit of normal are rarely false-positives
- Localisation (after biochemical confirmation):
- CT abdomen/pelvis (adrenal)
- MRI adrenal (better soft tissue detail)
- MIBG scintigraphy (metaiodobenzylguanidine scan) - for extra-adrenal or metastatic disease
- PET scan with DOTATATE for paragangliomas
(Comprehensive Clinical Nephrology 7e; Goldman-Cecil Medicine; Campbell Walsh Wein Urology)
4. Cushing's Syndrome (Cortisol Excess)
Hypertension present in up to 95% with ectopic ACTH; ~20% in iatrogenic Cushing's.
- Screening (any one of three):
- 24-hour urinary free cortisol (UFC) - most reliable confirmatory test
- Low-dose dexamethasone suppression test (LDDST - 1 mg overnight or 2-day)
- Late-night salivary cortisol (x2)
- Localisation:
- Plasma ACTH level (ACTH-dependent vs. ACTH-independent)
- MRI pituitary (Cushing's disease - pituitary adenoma)
- CT chest/abdomen (ectopic ACTH - small cell lung carcinoma, carcinoid)
- CT adrenal (adrenal adenoma/carcinoma)
- CRH stimulation test / inferior petrosal sinus sampling (IPSS) to distinguish pituitary from ectopic
(Frameworks for Internal Medicine, p. 521)
5. Renal Parenchymal Disease (CKD / Glomerulonephritis)
- Serum creatinine, eGFR, BUN
- Urine protein:creatinine ratio or 24-hour urine protein
- Urine microscopy (red cell casts - glomerulonephritis)
- Renal ultrasound (bilateral small kidneys = CKD; asymmetry suggests renovascular)
- Renal biopsy (if indicated by clinical findings)
- Complement levels (C3, C4), ANA, ANCA, anti-GBM (if glomerulonephritis suspected)
6. Obstructive Sleep Apnea (OSA) - Most Common Overall Cause
Present in >30% of hypertensives. Strongly associated with resistant hypertension.
- Polysomnography (full overnight sleep study) - gold standard
- Home sleep apnea test (HSAT) - portable device for uncomplicated cases
- Epworth Sleepiness Scale (screening questionnaire)
- 24-hour ambulatory blood pressure monitoring (ABPM) - to detect non-dipping pattern
7. Thyroid Disorders
- Serum TSH + free T4
- Note: Hypothyroidism causes diastolic hypertension; Hyperthyroidism causes systolic hypertension with wide pulse pressure
8. Coarctation of the Aorta
Clinical clue: hypertension in upper extremities only, radio-femoral delay, rib notching on chest X-ray.
- Chest X-ray (rib notching, "3 sign")
- Echocardiography
- CT or MR aortography (confirmatory)
9. Hyperparathyroidism / Hypercalcemia
- Serum calcium
- Parathyroid hormone (PTH)
- 24-hour urine calcium
10. Acromegaly
Hypertension in ~1/3 of patients, caused by GH excess.
- Serum IGF-1 (screening)
- Oral glucose tolerance test with GH suppression (confirmatory)
- MRI pituitary
Summary Table: Cause-Specific Investigations
| Cause | Screening Test | Confirmatory / Localisation |
|---|---|---|
| Primary hyperaldosteronism | Aldosterone:renin ratio | Salt-loading test; adrenal CT; adrenal vein sampling |
| Renovascular HTN | Renal duplex USS; CTA/MRA | Catheter renal angiography |
| Pheochromocytoma | Plasma free metanephrines | CT/MRI adrenal; MIBG scan |
| Cushing's syndrome | 24-hr urinary free cortisol; LDDST | Plasma ACTH; MRI pituitary; CT chest/abdomen |
| CKD/renal parenchymal | Creatinine, eGFR, urinalysis | Renal biopsy, complement/autoimmune screen |
| OSA | Polysomnography; ABPM | Home sleep test |
| Thyroid disease | TSH, free T4 | - |
| Coarctation of aorta | Chest X-ray | Echocardiography; CT/MR aortography |
| Hypercalcemia | Serum calcium | PTH, 24-hr urine calcium |
| Acromegaly | IGF-1 | OGTT with GH; MRI pituitary |
Key clinical points:
- Unprovoked hypokalemia should always trigger workup for primary hyperaldosteronism (the most common cause in most series).
- OSA is probably the most common cause overall, especially in obese patients with resistant hypertension.
- Bilateral BP measurement discrepancy (>20 mmHg) or absent femoral pulses should prompt coarctation workup.
- A rise in creatinine ≥30% after starting an ACE inhibitor or ARB is a strong clinical clue for bilateral renal artery stenosis.
- ABPM is useful to exclude white-coat hypertension before extensive secondary workup.
Sources: Harrison's Principles of Internal Medicine 22E; Frameworks for Internal Medicine; Brenner and Rector's The Kidney; Comprehensive Clinical Nephrology 7e; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.