Heparin post thrombolysis in ACS STEMI patients
Reading File
Finding Sources
Finding Sources
Searching PubMed
heparin anticoagulation post-thrombolysis STEMI
Reading File
Reading File
Finding Sources
Searching PubMed
STEMI fibrinolysis anticoagulant guideline
Reading File
Reading File
Finding Sources
Searching PubMed
STEMI thrombolysis anticoagulation enoxaparin
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
I have comprehensive information to synthesize a thorough answer. Let me now compile everything.
Anticoagulation (Heparin) Post-Thrombolysis in ACS/STEMI
Why Anticoagulation Is Needed After Fibrinolysis
Fibrinolytic agents dissolve the fibrin clot but leave a highly thrombogenic residual plaque and paradoxically activate thrombin. Adjunctive anticoagulation is therefore mandatory after thrombolysis to:
- Prevent re-occlusion of the infarct artery
- Suppress residual thrombus propagation
- Reduce reinfarction and recurrent ischemia
- Bridge patients to planned angiography/PCI (pharmacoinvasive strategy)
All STEMI patients receiving fibrinolysis should receive DAPT plus at least 48 hours of anticoagulation — Washington Manual of Medical Therapeutics
Anticoagulant Options After Fibrinolysis
1. Unfractionated Heparin (UFH)
The traditional agent — indicated especially when early angiography/PCI is planned.
| Parameter | Recommendation |
|---|---|
| Indication | Adjunct to fibrinolysis; preferred if PCI anticipated soon after |
| Duration | ≥48 hours after fibrinolysis |
| Dose (AHA/ACC) | Bolus 60 units/kg IV (max 4,000 units), then infusion 12 units/kg/h (max 1,000 units/h) |
| Dose (ESC) | 70–100 units/kg IV bolus (no GP IIb/IIIa); 50–60 units/kg if combined with GP IIb/IIIa |
| Monitoring | aPTT titrated to twice the upper limit of normal (~50–70 seconds) |
| Stopping | Cease after 48h to reduce risk of HIT; switch to another agent if longer anticoagulation needed |
Limitation: Highly unpredictable bioavailability — fewer than half of patients are adequately anticoagulated within 24 hours in clinical trials. Requires frequent aPTT checks and dose adjustments. — Tintinalli's Emergency Medicine
2. Enoxaparin (LMWH) — Preferred over UFH post-fibrinolysis
Large clinical trials (including EXTRACT-TIMI 25) demonstrated that enoxaparin improves outcomes in STEMI patients treated with aspirin + fibrinolysis compared to UFH.
A meta-analysis of 6 trials showed a 0.9% absolute reduction in death or recurrent MI with enoxaparin vs. UFH. The benefit is amplified in higher-risk patients (TIMI risk score >3), with a significant reduction in death, MI, and recurrent ischemia requiring PCI at 14 days. — Tintinalli's Emergency Medicine
| Parameter | Recommendation |
|---|---|
| Preferred when | Fibrinolysis chosen as reperfusion strategy (not first-line for primary PCI) |
| Renal restriction | Only if serum Cr <2.5 mg/dL (men) or <2.0 mg/dL (women) |
| Dosing | 30 mg IV bolus → 15 min later: 1 mg/kg SC q12h |
| Age ≥75 years | Omit IV bolus; reduce to 0.75 mg/kg SC q12h |
| Duration | Throughout index hospitalization, not to exceed 8 days |
| If PCI needed | Continue enoxaparin (do NOT switch to UFH — SYNERGY trial showed increased bleeding with antithrombin switching) |
| If CABG planned | Hold for 12–24 hours; bridge with UFH |
3. Fondaparinux
A synthetic factor Xa inhibitor; studied in the OASIS-6 trial.
- Has similar efficacy to UFH in STEMI patients receiving fibrinolytics
- Lower bleeding compared to enoxaparin in NSTEMI managed conservatively
- Cannot be used as monotherapy for PCI — if patient proceeds to PCI, must add UFH or bivalirudin before the procedure
- ESC does not recommend fondaparinux for PCI; ACC/AHA cautions against sole use during PCI
4. Bivalirudin (Direct Thrombin Inhibitor)
- Agent of choice in HIT (heparin-induced thrombocytopenia)
- Has not been extensively studied in STEMI patients receiving fibrinolysis
- If switching from UFH: discontinue UFH for 30 minutes before starting bivalirudin
- Dose: 0.75 mg/kg bolus → 1.75 mg/kg/h infusion
Post-Fibrinolysis Strategy: Pharmacoinvasive Approach
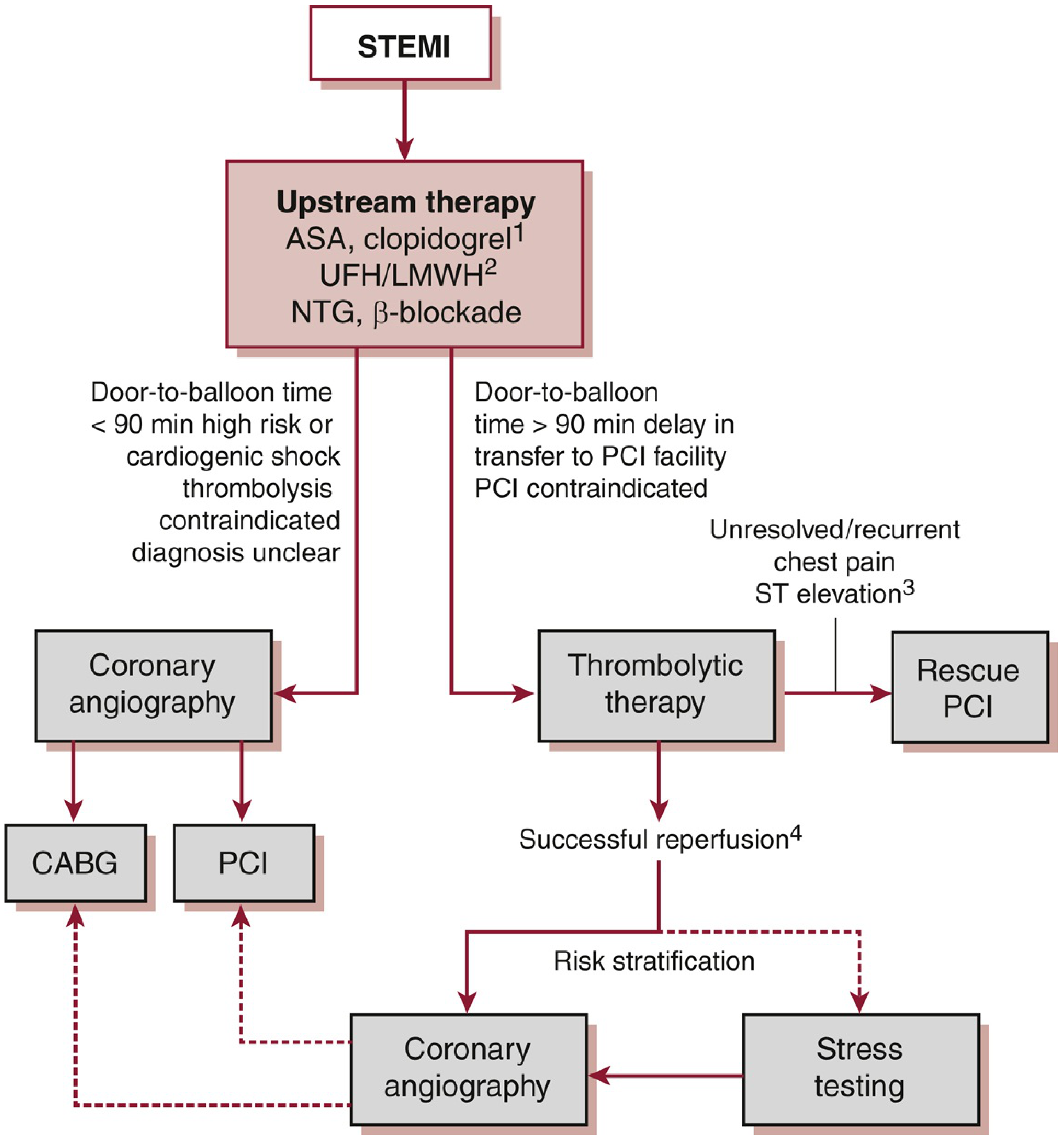
Note: LMWH and fondaparinux are preferred over UFH when fibrinolysis is the reperfusion strategy. UFH is acceptable for both fibrinolysis and PCI.
All patients who receive fibrinolysis should be transferred to a PCI-capable facility for routine coronary angiography within 3–24 hours (pharmacoinvasive strategy). This has been shown to reduce adverse cardiac events compared to rescue PCI alone (TRANSFER-AMI trial: 6.2% absolute reduction in composite endpoint of death, reinfarction, ischemia, HF, or cardiogenic shock at 30 days).
Signs of successful reperfusion (to guide urgency of angiography):
- Relief of chest pain/angina
-
50% reduction in ST-segment elevation at 90 minutes
- Reperfusion arrhythmia (accelerated idioventricular rhythm) within 2 hours
Rescue PCI is indicated for failed fibrinolysis (persistent ST elevation, ongoing chest pain, hemodynamic instability).
Practical Decision Summary
STEMI → Fibrinolysis chosen
↓
Anticoagulation for ≥48h (up to 8 days with enoxaparin):
• Enoxaparin: PREFERRED (if CrCl adequate)
- 30 mg IV bolus + 1 mg/kg SC q12h
- Omit bolus if age ≥75; dose-reduce if eGFR <30
• UFH: acceptable; PREFERRED if early PCI planned
- 60 units/kg IV bolus (max 4000 u) + 12 units/kg/h (max 1000 u/h)
- Titrate aPTT to 2× ULN
- Stop at 48h or continue through PCI
• Fondaparinux: option; CANNOT use alone at PCI
• Bivalirudin: HIT only; limited fibrinolysis data
↓
Transfer for angiography 3–24h post-fibrinolysis (pharmacoinvasive)
Key Points
- Enoxaparin is preferred over UFH in STEMI patients receiving fibrinolytics — superior outcomes in major RCTs, more predictable anticoagulation
- UFH is preferred when early catheterization is planned due to ease of reversal and cath lab familiarity
- Do not switch antithrombins mid-treatment (e.g., enoxaparin in ED → UFH in cath lab) — SYNERGY trial showed this increases bleeding without benefit
- Minimum 48 hours anticoagulation; enoxaparin can be continued up to 8 days
- HIT patients: use bivalirudin (avoid all heparins including LMWH)
- Fondaparinux cannot be used alone at PCI — must supplement with UFH or bivalirudin
Sources: Tintinalli's Emergency Medicine (9th ed.), Washington Manual of Medical Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.