Classification of shock.. monitoring and diagnosis of shock and management
Reading File
Finding Sources
Finding Sources
Searching PubMed
"shock" AND "management" AND "classification"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive content from Harrison's, Goldman-Cecil, Bailey & Love, Miller's, and Fischer's Surgery. I have enough to write a thorough, well-organized response covering all three areas: classification, monitoring/diagnosis, and management.
Shock: Classification, Monitoring, Diagnosis, and Management
1. Pathophysiology (Brief Overview)
Shock is defined as a state of circulatory failure resulting in inadequate tissue oxygen delivery (DO2) relative to demand, leading to cellular hypoxia and, if uncorrected, irreversible end-organ damage and death.
The key determinants of oxygen delivery are:
DO2 = CO × CaO2 CaO2 = (Hb × 1.34 × SaO2) + (PaO2 × 0.003)
Any process that reduces CO, Hb, SaO2, or increases SVR/impedance can impair DO2. Each shock type has a distinctive hemodynamic fingerprint corresponding to derangements in these variables.
- Harrison's Principles of Internal Medicine 22E
2. Classification of Shock
Shock is classified into four major physiologic categories:
- Harrison's Principles of Internal Medicine 22E, Bailey & Love's Short Practice of Surgery 28e, Miller's Anesthesia 10e
A. Distributive Shock
The most common type (~33-50% of shock presentations). The primary derangement is a reduced SVR with compensatory increase in CO. Tissue perfusion is inadequate despite normal or elevated flow, because blood is maldistributed.
Subtypes and causes:
| Subtype | Mechanism |
|---|---|
| Septic shock | Dysregulated host response to infection; vasodilation via NO, cytokines |
| Anaphylactic shock | IgE-mediated; histamine-mediated arterial and venous vasodilation; up to 35% of plasma volume can extravasate within 10 min |
| Neurogenic shock | Spinal cord injury disrupts autonomic tone; venous pooling, decreased venous return |
| Endocrine shock | Adrenal insufficiency (cortisol/aldosterone deficiency), hypothyroid/myxedema crisis |
| Pancreatitis / severe burns | Massive inflammatory mediator release |
| SIRS | Systemic inflammatory activation without infection |
- Harrison's Principles of Internal Medicine 22E
B. Cardiogenic Shock
Primary pump failure causing reduced CO despite adequate intravascular volume. SVR rises compensatorily. PCWP is elevated (LV failure) and/or CVP elevated (RV failure).
Causes:
-
Primary: Acute MI, myocarditis, cardiomyopathy
-
Electrical: Significant arrhythmias (extreme bradycardia/tachyarrhythmia)
-
Structural/Valvular: Severe aortic or mitral regurgitation; valvular stenosis
-
Subtypes: LV failure (most common), RV failure, biventricular failure
-
Fuster and Hurst's The Heart 15e, Harrison's 22E
C. Hypovolemic Shock
The most common cause of all shock. Reduced circulating volume decreases preload, CO falls, and SVR rises compensatorially.
Causes:
| Subtype | Examples |
|---|---|
| Hemorrhagic | Trauma, GI bleeding, ruptured ectopic pregnancy |
| Non-hemorrhagic | Vomiting, diarrhoea, burns, diabetic polyuria, third-spacing (bowel obstruction, pancreatitis), dehydration |
- Bailey & Love's Short Practice of Surgery 28e, Harrison's 22E
D. Obstructive Shock
Mechanical obstruction to cardiac filling or outflow causing reduced CO with elevated CVP.
Causes:
-
Tension pneumothorax
-
Cardiac tamponade
-
Massive pulmonary embolism
-
Constrictive pericarditis
-
Aortic dissection
-
Mediastinal masses
-
Harrison's 22E, Bailey & Love 28e
E. Endocrine Shock (Bailey & Love classification)
Some surgical texts list this separately: includes adrenal crisis, hypothyroid crisis, and pheochromocytoma. Harrison's incorporates these under distributive shock.
3. ATLS Classification of Hemorrhagic Shock
Hemorrhagic shock is further graded into four classes (ATLS), which guides immediate fluid resuscitation:
| Parameter | Class I | Class II | Class III | Class IV |
|---|---|---|---|---|
| Blood loss (mL) | Up to 750 | 750-1,500 | 1,500-2,000 | >2,000 |
| % Blood volume | Up to 15% | 15-30% | 30-40% | >40% |
| Pulse rate | <100 | >100 | >120 | >140 |
| Blood pressure | Normal | Normal | Decreased | Decreased |
| Pulse pressure | Normal/↑ | Decreased | Decreased | Decreased |
| Respiratory rate | 14-20 | 20-30 | 30-40 | >35 |
| Urine output (mL/hr) | >30 | 20-30 | 5-15 | Negligible |
| Mental status | Slightly anxious | Mildly anxious | Anxious, confused | Confused, lethargic |
| Fluid therapy | Crystalloid | Crystalloid | Crystalloid + blood | Crystalloid + blood |
- Goldman-Cecil Medicine International Edition, ATLS (ACS)
4. Hemodynamic Profiles of Shock Types
This is the key diagnostic tool when clinical type is unclear:
| Type of Shock | CVP | PCWP | Cardiac Output | SVR |
|---|---|---|---|---|
| Distributive | ↓ | ↓ | ↑ | ↓ |
| Cardiogenic | ↑ | ↑ | ↓ | ↑ |
| Obstructive | ↑ | ↓ or ↑ | ↓ | ↑ |
| Hypovolemic | ↓ | ↓ | ↓ | ↑ |
- Harrison's Principles of Internal Medicine 22E (Table 314-2)
5. Monitoring of Shock
Minimum Standard Monitoring
- ECG (continuous)
- Pulse oximetry (SpO2)
- Blood pressure (non-invasive, frequent)
- Urine output (hourly - Foley catheter) - the best clinical monitor of organ perfusion (goal: >0.5 mL/kg/hr or >30 mL/hr)
- Conscious level / GCS
Additional/Invasive Monitoring
- Central venous pressure (CVP): CVP alone is a poor predictor of volume status and should be assessed dynamically using fluid challenge (250-500 mL bolus): no rise = hypovolemic; large sustained rise = volume overloaded/cardiac insufficiency
- Arterial line: Continuous invasive BP monitoring; allows ABG sampling
- Cardiac output monitoring: Pulmonary artery catheter (PAC/Swan-Ganz), pulse contour analysis (PiCCO, LiDCO), or point-of-care echo
- Central venous oxygen saturation (ScvO2) / Mixed venous oxygen saturation (SvO2):
- Normal: 50-70%
- <50% indicates inadequate delivery and high extraction (hypovolemic/cardiogenic shock)
-
70% (normal in sepsis) - disordered oxygen utilization
Systemic/Biochemical Monitoring
- Serum lactate: Most sensitive marker of tissue hypoperfusion. Elevated in all types of shock. Serial lactate is used to assess response to treatment. A rising/non-clearing lactate indicates occult hypoperfusion ("occult hypoperfusion" with normal vital signs but persistent lactate acidosis). Patients in occult hypoperfusion >12 hours have 2-3x the mortality.
- Base deficit (arterial/venous blood gas): A base deficit < -6 mEq/L is significant
- ScvO2 + lactate together provide the best endpoint of resuscitation over vital signs alone
Table: Monitors for Organ/Systemic Perfusion (Bailey & Love 28e):
| System | Clinical | Investigational |
|---|---|---|
| Systemic | - | Base deficit, Lactate, SvO2 |
| Kidney | Urine output | - |
| Brain | Conscious level | Tissue O2 electrode, NIRS |
| Gut | - | Sublingual capnometry, gut mucosal pH |
| Muscle | - | Near-infrared spectroscopy |
- Bailey & Love's Short Practice of Surgery 28e
6. Diagnosis of Shock
Clinical Diagnosis
Shock = hypotension + signs of hypoperfusion
History clues:
- Fever, rash → septic/distributive shock
- Bleeding, trauma → hypovolemic/hemorrhagic shock
- JVD, orthopnea → cardiogenic/obstructive shock
- Allergen exposure → anaphylaxis
Physical findings:
- Tachycardia (most consistent early sign)
- Cold, clammy skin (vasoconstriction in hypovolemic/cardiogenic)
- Warm, flushed skin with bounding pulse (distributive/septic)
- JVD with muffled heart sounds + hypotension = tamponade (Beck's triad)
- JVD + absent breath sounds unilaterally = tension pneumothorax
- Altered mental status, oliguria
Initial Laboratory Evaluation (Harrison's 22E, Table 314-4)
- Serum lactate - diagnosis and risk stratification
- Renal function tests (BUN, creatinine)
- Liver function tests (transaminases, ALP)
- Cardiac enzymes (troponin, BNP)
- Complete blood count (Hb, WBC with differential)
- Coagulation profile (PT, PTT, INR)
- Pregnancy test (females of reproductive age)
- Urinalysis and urine sediment
- Arterial blood gas (assess oxygenation, pH, base deficit)
- ECG - arrhythmia, STEMI, RV strain pattern (PE)
- CXR - pulmonary edema, pneumothorax, widened mediastinum
- Blood, urine, sputum cultures (if sepsis suspected)
Imaging
- Bedside ultrasound (POCUS): Single most useful tool for undifferentiated shock
- Assess cardiac chambers (size, contractility)
- Pericardial effusion (tamponade)
- IVC collapsibility (volume responsiveness)
- B-lines (pulmonary edema)
- Free intraperitoneal fluid (ruptured viscus, hemorrhage)
7. Management of Shock
Overview (Goldman-Cecil Management Flowchart):
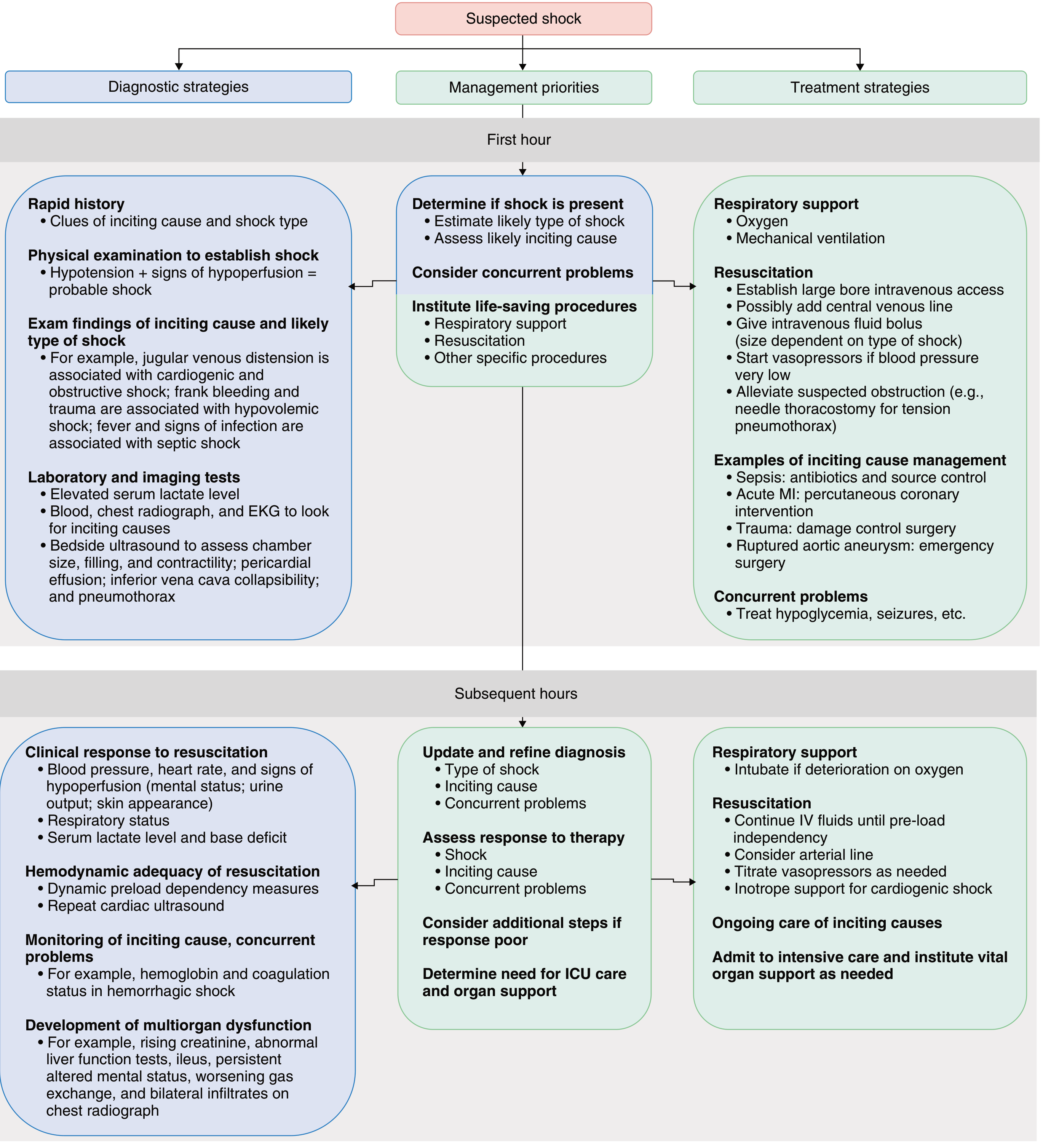
Goldman-Cecil Medicine International Edition, Fig. 92-2
General Principles - "ABCDE" + Source Control
A - Airway/Breathing:
- High-flow oxygen to all patients
- Intubate if GCS ≤8, respiratory failure, or refractory shock
B - Intravenous Access:
- 2 large-bore peripheral IVs (#16 gauge or larger) for rapid fluid infusion
- Central venous catheter (subclavian/internal jugular, ideally ultrasound-guided) for vasopressors and CVP monitoring; short, large-bore (8.5 Fr) catheter if rapid infusion also needed
C - Fluid Resuscitation:
- Initial bolus: 500 mL crystalloid (normal saline or lactated Ringer's) over 20-30 min; reassess response
- If clearly volume depleted (hemorrhage, severe sepsis): 20-30 mL/kg as a bolus
- Cardiogenic shock: cautious small bolus (125-250 mL); risk of pulmonary edema
- Resuscitate to preload independence (point on Starling curve where further fluid no longer increases CO), but avoid overfilling
- Avoid dextrose-containing fluids in shock unless free water deficits (DI)
- Hemorrhagic shock Class III-IV: 1:1:1 ratio of packed RBCs : FFP : platelets (damage control resuscitation); transfuse pRBC when Hb <7 g/dL (septic shock) or <8 g/dL (cardiogenic/MI)
D - Vasopressors and Inotropes (when fluid is insufficient):
| Agent | Mechanism | Indication |
|---|---|---|
| Norepinephrine | α1 + β1 | First-line for septic shock and most distributive shock; also used in hypovolemic shock after volume replacement |
| Vasopressin | V1 receptor | Adjunct in septic shock refractory to norepinephrine (0.03-0.04 units/min) |
| Dopamine | Dose-dependent α, β, DA | Alternative to norepinephrine; higher arrhythmia risk |
| Epinephrine | α1 + β1 + β2 | Anaphylaxis (IM first), refractory shock |
| Dobutamine | β1 (inotrope) | Cardiogenic shock - increases contractility; septic shock with myocardial depression (targeting SvO2 >70%) |
| Phenylephrine | Pure α1 | Tachyarrhythmia-associated hypotension |
| Norepinephrine + Dobutamine | Combined | Cardiogenic shock with systemic vasodilation |
Vasopressors should be given through a central line. They increase afterload, so adequate hydration first is important.
E - Treat the Etiology (Specific Interventions):
| Shock Type | Specific Intervention |
|---|---|
| Septic shock | Blood cultures → broad-spectrum antibiotics within 1 hour of recognition; source control (drainage, surgery); norepinephrine; hydrocortisone 200 mg/day if refractory |
| Anaphylactic shock | Remove trigger; epinephrine IM 0.5 mg (anterolateral thigh); IV fluids; diphenhydramine; corticosteroids |
| Cardiogenic (STEMI) | Emergent PCI (reperfusion); inotropes; mechanical circulatory support (IABP, Impella, ECMO) |
| Cardiogenic (arrhythmia) | Cardioversion/pacing as per ACLS |
| Cardiogenic (valve) | Emergency surgical valve repair/replacement |
| Tension pneumothorax | Immediate needle decompression (2nd intercostal space, mid-clavicular line) → chest drain |
| Cardiac tamponade | Pericardiocentesis (ultrasound-guided) or surgical drainage |
| Massive PE | Thrombolysis (systemic or catheter-directed); surgical embolectomy |
| Aortic dissection | Emergency vascular surgery |
| Hemorrhagic shock | Damage control surgery; tourniquet; tranexamic acid within 3 hours of trauma |
| Adrenal crisis | IV hydrocortisone 100 mg stat + 200 mg/day; fluid resuscitation |
- Harrison's Principles of Internal Medicine 22E, Goldman-Cecil Medicine
Endpoints of Resuscitation
Traditional endpoints (BP, HR, urine output) can normalize despite ongoing tissue hypoperfusion ("occult hypoperfusion"). Modern resuscitation targets:
| Parameter | Target |
|---|---|
| MAP | ≥65 mmHg |
| Urine output | ≥0.5 mL/kg/hr |
| Serum lactate | Clearance ≥10% per 2 hours; target <2 mmol/L |
| ScvO2 | ≥70% |
| Base deficit | Normalization |
- Bailey & Love's Short Practice of Surgery 28e, Goldman-Cecil Medicine
Complications of Shock
If shock is prolonged or resuscitation is delayed:
- Multiple Organ Failure (MOF) - defined as ≥2 failed organ systems; mortality ~60%; no specific treatment, only organ support (ventilation, renal replacement therapy)
- ARDS (from reperfusion injury and aggressive crystalloid resuscitation)
- Abdominal compartment syndrome (aggressive fluid resuscitation)
- Acute kidney injury
- Ischaemia-reperfusion injury - release of DAMPs, cytokines, complement activation; can only be attenuated by limiting duration of shock
- Bailey & Love's Short Practice of Surgery 28e
Key Principle: Shock management requires two simultaneous tracks - resuscitate the circulation (oxygen, fluids, vasopressors) AND treat the underlying cause (antibiotics, PCI, surgery). Neither alone is sufficient. Goals should target global perfusion endpoints (lactate, SvO2) rather than vital signs alone.
This is a shared conversation. Sign in to Orris to start your own chat.