Give me basics idea and things to know about DCM ,RCM HCM make sure I understand I am beginner for fmge
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have everything needed to write a comprehensive FMGE-oriented guide. Let me compile the full answer.
Cardiomyopathies for FMGE: DCM, HCM & RCM
Source: Robbins & Kumar Basic Pathology, Table 9.5 + Chapter 9
The Big Picture First 🧠
A cardiomyopathy = primary disease of the heart muscle itself (not due to ischemia, valvular disease, or hypertension).
There are 3 main functional types — remember them by what goes wrong with the heart's job:
| Type | Core Problem | EF | Dysfunction |
|---|---|---|---|
| DCM | Can't squeeze → weak pump | < 40% | Systolic |
| HCM | Can't relax → stiff, outflow blocked | 50–80% (hyperdynamic) | Diastolic |
| RCM | Can't fill → wall too stiff | 25–50% | Diastolic |
Simple memory hook:
- DCM → Dilated → Does not contract → systolic failure
- HCM → Hypertrophied → Hard to fill/relax → diastolic failure
- RCM → Restricted → Rigid wall → diastolic failure
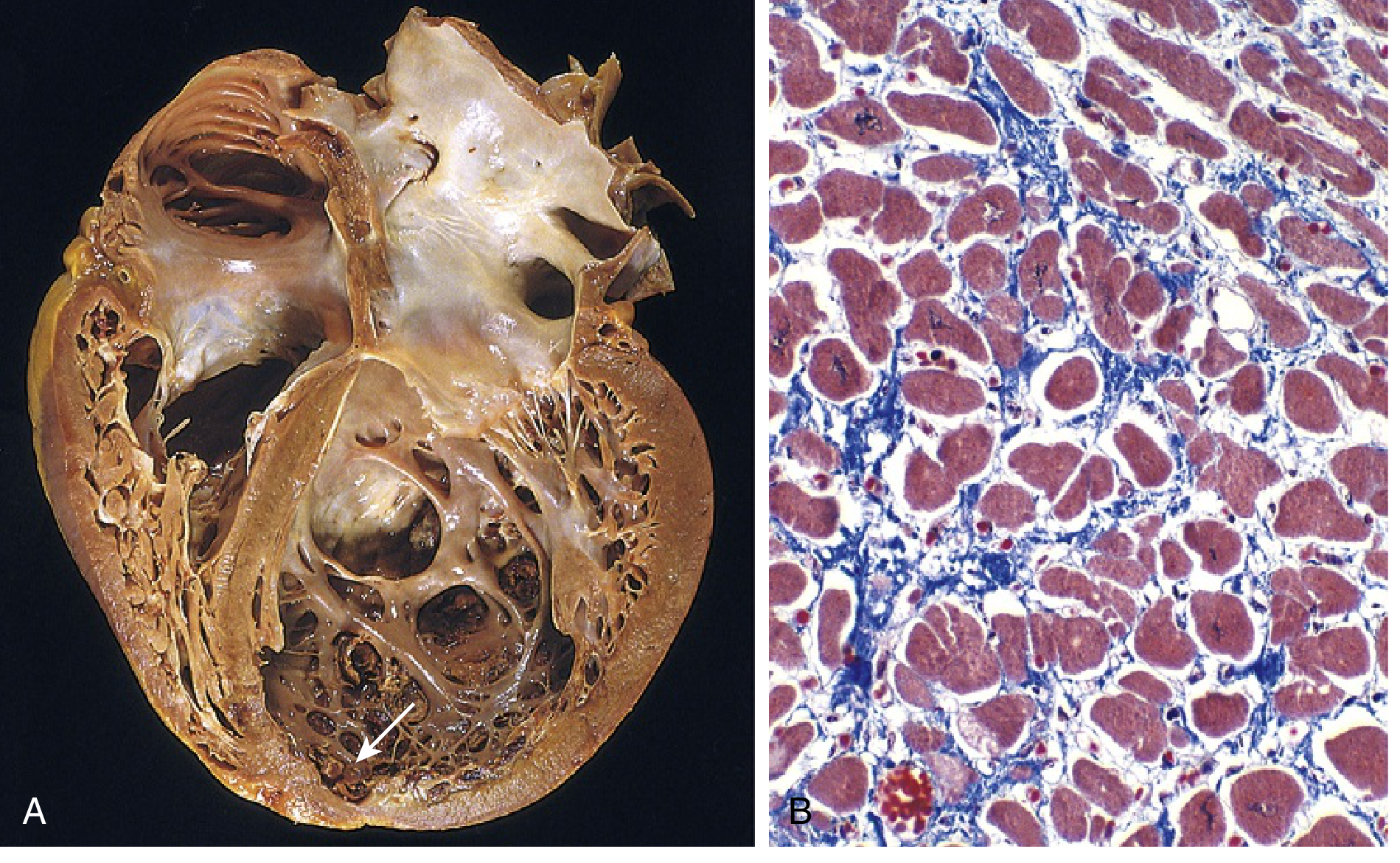
1. Dilated Cardiomyopathy (DCM)
The classic "big, floppy heart"
Pathology
- All 4 chambers dilate (especially LV)
- Wall becomes thin (despite some hypertrophy)
- Heart is enlarged up to 2–3× normal weight, looks flabby
- Mural thrombi common → risk of systemic thromboembolism
- Histo: myocyte hypertrophy + interstitial fibrosis (blue on Masson trichrome)
Causes (FMGE favorites — memorize)
| Category | Examples |
|---|---|
| Genetic (20–50%) | Titin mutations (most common), β-myosin heavy chain, dystrophin (X-linked) |
| Viral myocarditis | Coxsackievirus B, parvovirus B19, HHV-6 |
| Alcohol/Toxins | Alcohol (acetaldehyde toxic), doxorubicin (chemo), cobalt |
| Peripartum | Late pregnancy / weeks postpartum |
| Iron overload | Hemochromatosis, multiple transfusions |
| Others | Sarcoidosis, chronic anemia, idiopathic |
FMGE tip: Doxorubicin (adriamycin) → DCM. Peripartum cardiomyopathy → ~50% recover spontaneously.
Clinical Features
- Progressive heart failure (breathlessness, fatigue, leg swelling)
- Systolic dysfunction — EF < 40%
- S3 gallop, cardiomegaly on CXR
- Risk of arrhythmias and thromboemboli
- Treatment: ACE inhibitors, beta-blockers, diuretics, anticoagulation
2. Hypertrophic Cardiomyopathy (HCM)
The "thick, banana-shaped" heart — #1 cause of sudden death in young athletes
Pathology
- Massive myocardial hypertrophy WITHOUT dilation
- 90% asymmetric septal hypertrophy (ASH) — septum thicker than LV free wall
- LV cavity compressed → "banana-shaped" lumen
- Anterior mitral leaflet touches the septum → creates outflow tract obstruction (in ~1/3 cases) + mitral regurgitation
- Systolic anterior motion (SAM) of mitral valve — important on echo
Histology (classic FMGE question):
- Myocyte disarray (haphazard arrangement) ← pathognomonic
- Myocyte hypertrophy
- Interstitial fibrosis
Cause — Almost Always Genetic
- Autosomal dominant, variable expression
- Gain-of-function mutations in sarcomeric proteins
- Most common: β-myosin heavy chain > myosin-binding protein C > troponin T
- These 3 account for 70–80% of all HCM
- Other causes: Friedreich's ataxia, storage diseases, infant of diabetic mother
Key concept: Same genes mutated as in DCM, but HCM = gain-of-function vs. DCM = loss-of-function
Clinical Features
- Diastolic dysfunction — myocardium doesn't relax after systole
- EF is actually HIGH (hypercontractile) but filling is impaired
- Exertional dyspnea + angina + harsh systolic ejection murmur (LVOT obstruction)
- Murmur increases with Valsalva and standing (decreased preload → worsens obstruction)
- Murmur decreases with squatting (increased preload → reduces obstruction)
- Sudden cardiac death — #1 cause in athletes < 35 years
- Atrial fibrillation, infective endocarditis (mitral valve)
- Treatment: Beta-blockers or calcium channel blockers (promote relaxation), avoid inotropes/vasodilators; surgery (septal myectomy) or alcohol ablation for severe cases
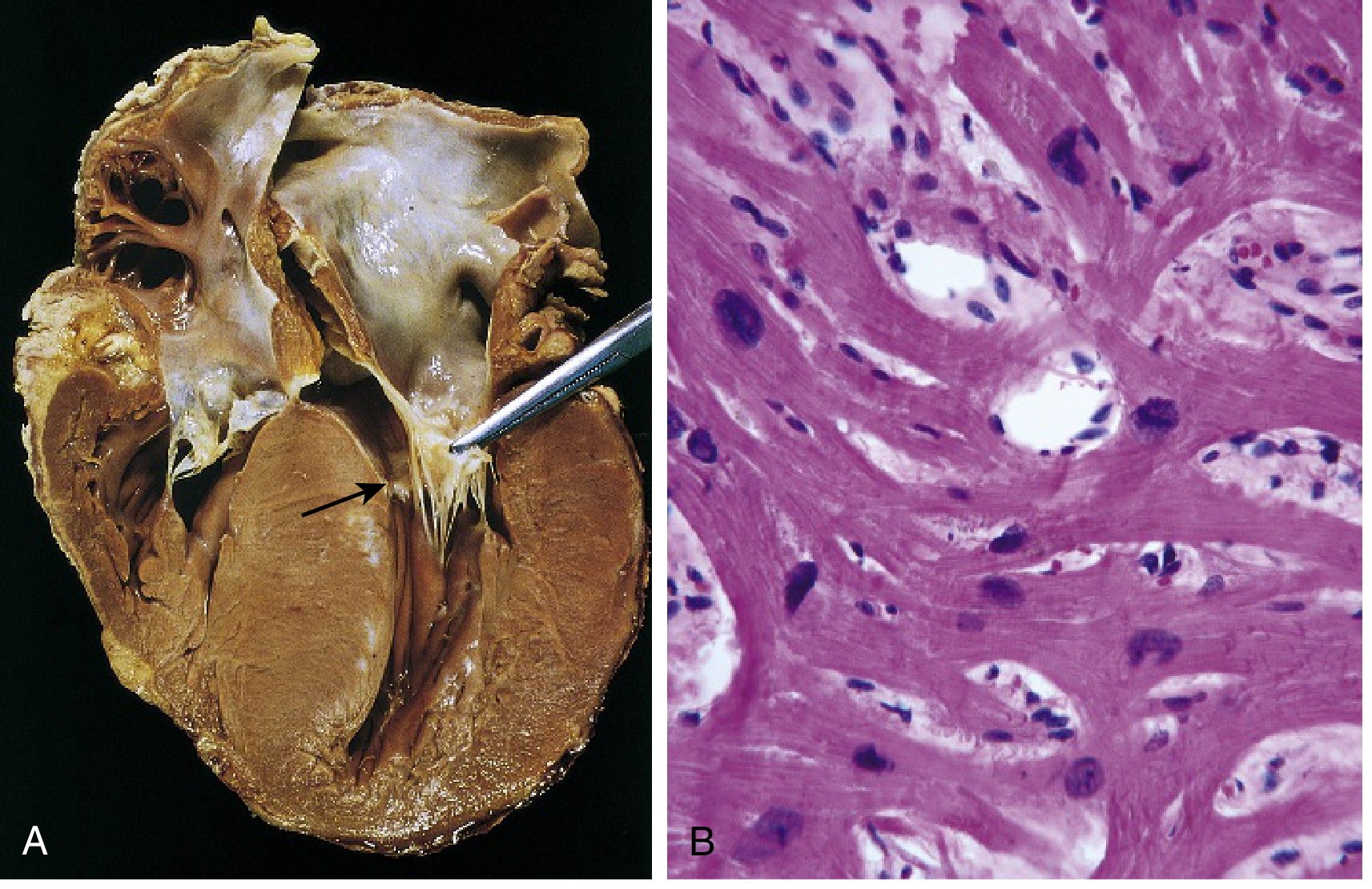
3. Restrictive Cardiomyopathy (RCM)
The "rigid, non-compliant" heart — hardest to fill
Pathology
- Ventricles are normal size or slightly enlarged, NOT dilated
- Both atria are typically dilated (blood can't get into stiff ventricles → backs up)
- Wall is firm/stiff
- EF can be relatively preserved but filling is severely impaired
- Histo: variable interstitial fibrosis
Causes (most important for FMGE)
| Cause | Key Fact |
|---|---|
| Amyloidosis | Most tested — Congo red stain, apple-green birefringence; transthyretin (TTR) amyloid in elderly; AL amyloid in myeloma |
| Endomyocardial fibrosis | Most common RCM worldwide; children/young adults in Africa; involves tricuspid & mitral valves |
| Loeffler endomyocarditis | Hypereosinophilia → eosinophil granules toxic to myocardium → fibrosis + mural thrombus |
| Sarcoidosis | Granulomas in myocardium |
| Radiation fibrosis | Post-radiation therapy |
| Hemochromatosis | Iron deposition (can also cause DCM) |
| Storage diseases | Mucopolysaccharides, sphingolipids |
Clinical Features
- Symptoms of heart failure with preserved EF
- JVP elevated with Kussmaul's sign (JVP rises on inspiration)
- Must be distinguished from constrictive pericarditis (clinically very similar — key differentiator is endomyocardial biopsy)
- Treatment: treat underlying cause; diuretics for congestion; anticoagulation in some cases
Master Comparison Table (FMGE Rapid Revision)
| Feature | DCM | HCM | RCM |
|---|---|---|---|
| Heart size | Big & dilated | Big & thick (no dilation) | Normal or slightly enlarged |
| LV wall | Thin (dilated out) | Very thick | Normal/firm |
| Dysfunction | Systolic | Diastolic | Diastolic |
| EF | ↓↓ (<40%) | ↑ or normal (50–80%) | ↓ or normal (25–50%) |
| Atrial dilation | Yes (all chambers) | LA only | Both atria markedly dilated |
| Histology | Hypertrophy + fibrosis | Myocyte disarray + fibrosis | Interstitial fibrosis / specific infiltrate |
| Genetics | Loss-of-function (titin, dystrophin) | Gain-of-function (β-MHC) | Usually NOT genetic (exceptions: TTR amyloid) |
| Key cause | Alcohol, viral, doxorubicin | Genetic (autosomal dominant) | Amyloidosis, endomyocardial fibrosis |
| Sudden death? | Yes | YES — #1 in young athletes | Less common |
| Mural thrombus | Common (LV apex) | Less common | In Loeffler's |
| Key FMGE buzz | Peripartum, doxorubicin | ASH, banana-shaped, SAM | Congo red, Loeffler's eosinophilia |
Quick Memory Mnemonics
DCM causes → "A PIIVD"
- Alcohol, Peripartum, Idiopathic, Iron (hemochromatosis), Virus, Doxorubicin
HCM genes → "β-MHC BT"
- β-myosin heavy chain, myosin-Binding protein C, Troponin T
RCM causes → "SAFE"
- Sarcoidosis, Amyloidosis, Fibrosis (radiation/endomyocardial), Eosinophilia (Loeffler's)
— Robbins & Kumar Basic Pathology, pp. 371–375
This is a shared conversation. Sign in to Orris to start your own chat.