Pempigus vulgaris
Reading File
Finding Sources
Searching PubMed
"pemphigus vulgaris"[MeSH Terms] AND treatment
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching Images
pemphigus vulgaris oral erosions flaccid blisters skin
Reading File
Loading Image
I now have comprehensive information from the textbooks. Let me compile the full answer.
Pemphigus Vulgaris (PV)
Definition
Pemphigus vulgaris is a tissue-specific autoimmune blistering disease of the skin and mucous membranes, characterized histologically by intraepidermal blisters due to acantholysis (loss of cell-cell adhesion of keratinocytes) and immunopathologically by in vivo bound and circulating IgG autoantibodies against keratinocyte cell-surface adhesion molecules (desmogleins).
Epidemiology
- Incidence: 0.76–5 new cases per million/year worldwide; markedly higher in Ashkenazi Jews (16–32 per million/year)
- Equal sex distribution; mean age of onset 50–60 years (broad range)
- Higher incidence in Middle East, Southeast Europe, and India
- Most common form of pemphigus in most countries (~75% of cases in France, ~67% in Japan)
- HLA associations: DRB1*0402 and DQB1*0503 confer risk, particularly in Ashkenazi Jews
Pathogenesis
Target Antigens — Desmogleins
The autoantigens are desmogleins (Dsg), transmembrane glycoproteins of the cadherin superfamily located at the desmosome — the major cell-cell adhesion junction in stratified squamous epithelia.
| Antibody | Antigen | PV subtype |
|---|---|---|
| Anti-Dsg3 alone | Dsg3 (deep epidermis + all mucosa) | Mucosal-dominant PV |
| Anti-Dsg3 + Anti-Dsg1 | Both | Mucocutaneous PV |
Desmoglein Compensation Theory
The distribution of Dsg1 vs. Dsg3 in different epithelial layers explains the clinical phenotype:
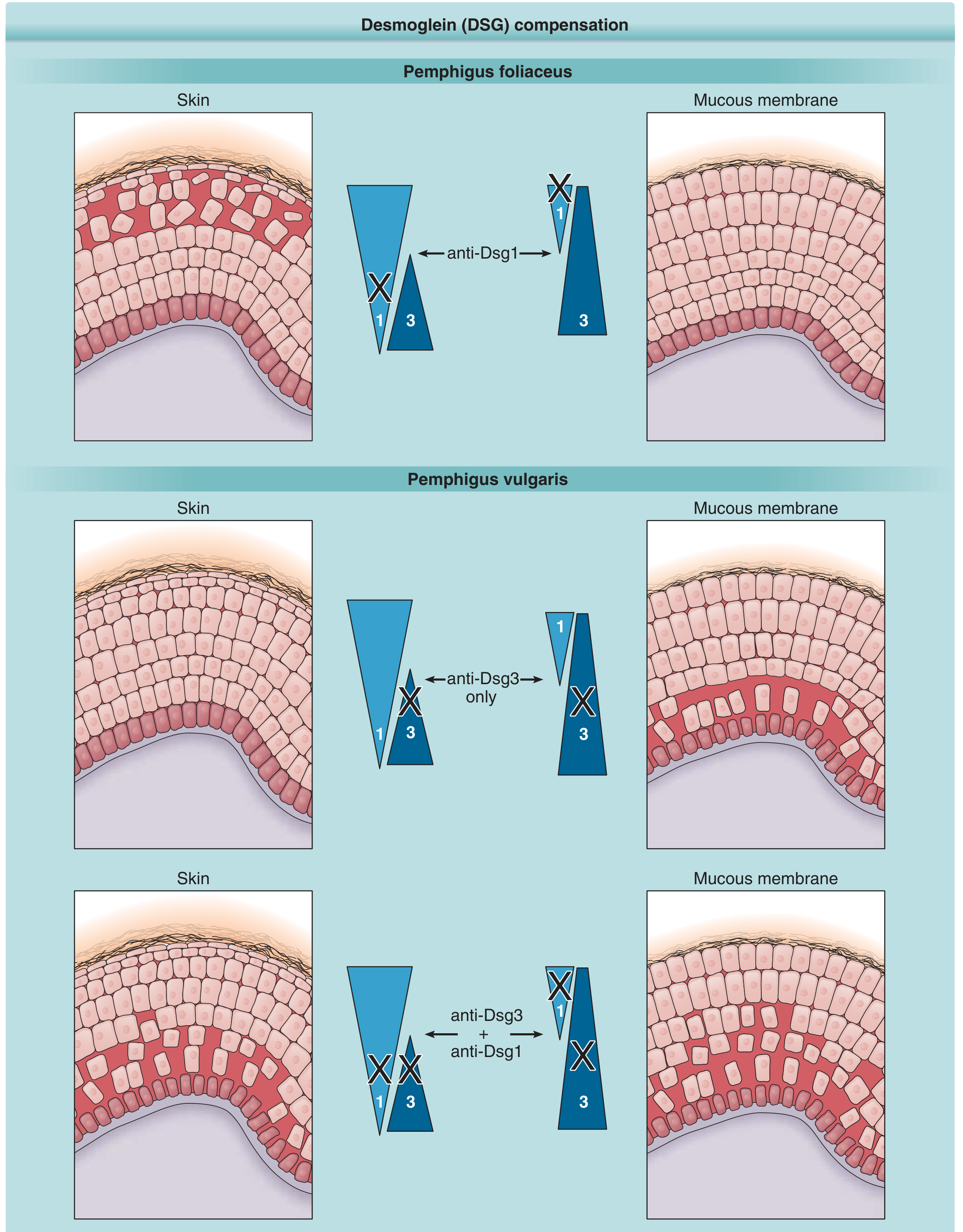
- In mucosal-dominant PV: anti-Dsg3 antibodies cause blistering only in mucosa (where Dsg3 predominates without compensatory Dsg1)
- In mucocutaneous PV: both anti-Dsg1 and anti-Dsg3 present → blisters in skin and mucosa; blisters are suprabasilar because antibodies diffuse from the dermis upward
Mechanism of Blister Formation
IgG autoantibodies (mainly IgG4) bind to the extracellular domain of Dsg3/Dsg1 at or near the adhesive interface, interfering with desmosomal adhesion → acantholysis → suprabasilar cleft formation. The antibodies are directly pathogenic: passive transfer of patient IgG to neonatal mice reproduces the disease.
Immunogenetics
- CD4+ T follicular helper cells stimulate anti-Dsg B cells
- VH1-46 gene usage shared among anti-Dsg3 B cells in PV patients (early autoimmune selection)
- Regulatory T cells may suppress autoimmunity in HLA-susceptible individuals who do not develop disease
Clinical Features
Subtypes
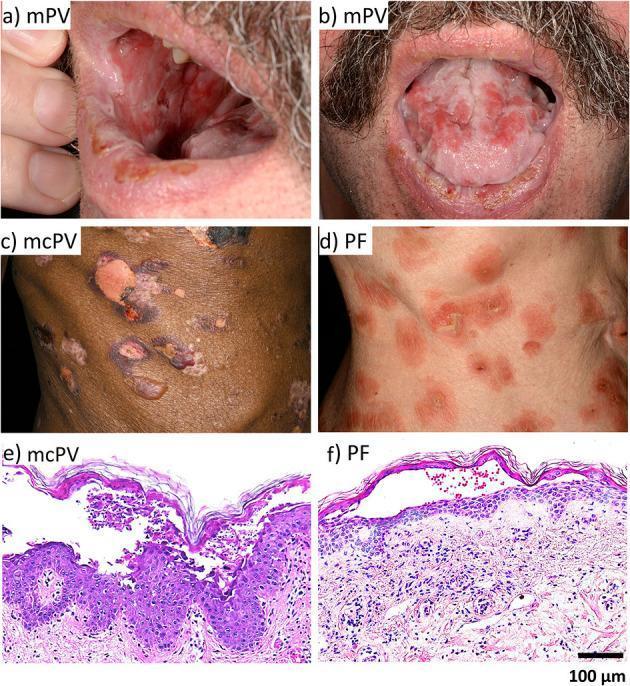
- Mucosal-dominant PV — oral/mucosal erosions, minimal skin lesions (anti-Dsg3 only)
- Mucocutaneous PV — widespread skin blisters and erosions + mucosal involvement (anti-Dsg1 + anti-Dsg3)
Oral / Mucosal Lesions
- Present in essentially all PV patients — often the first manifestation (months before skin)
- Painful erosions most common (blisters are fragile and break immediately)
- Sites: buccal and palatine mucosae most common; also throat, nasal mucosa, esophagus, conjunctiva, vagina, labia, penis, anus
- Esophageal involvement can cause sloughing of the mucosal lining as a cast
- Laryngeal involvement (55% of patients on endoscopy) often asymptomatic
- Oral disease frequently misdiagnosed, delaying diagnosis by months
Cutaneous Lesions
- Flaccid blisters on normal-appearing or erythematous skin — thin-roofed, easily ruptured
- Blisters are NOT tense (unlike bullous pemphigoid)
- Fluid: initially clear → may become hemorrhagic, turbid, seropurulent
- Rupture → large, painful erosions that ooze and bleed easily; do not heal spontaneously
- Heal with hyperpigmentation, no scarring
- Distribution: any skin surface, typically sparing palms and soles

Clinical Signs
| Sign | Description |
|---|---|
| Nikolsky sign | Lateral pressure on normal-appearing skin causes epidermis to shear off |
| Asboe-Hansen sign (Nikolsky II) | Pressure on intact bulla spreads fluid laterally under the skin |
Pemphigus Vegetans (variant)
- Vegetating/papillomatous lesions in intertriginous areas (axillae, groin, scalp)
- Suprabasilar acantholysis + intense eosinophilic infiltrate + microabscesses
- Better prognosis than typical PV; higher chance of remission
Diagnosis
Histopathology
- Suprabasilar acantholysis — cleft just above the basal layer
- Basal cells remain attached to basement membrane → "tombstone row" appearance
- Rounded-up acantholytic keratinocytes within blister cavity
- No keratinocyte necrosis
- Dermal papillae protrude into blister cavity; eosinophils in cavity and dermis
- Biopsy site: Edge of fresh blister + perilesional skin (for DIF)
Immunofluorescence
| Test | Finding |
|---|---|
| Direct IF (DIF) | IgG + C3 deposited on keratinocyte cell surfaces in an intercellular/fishnet pattern throughout epidermis |
| Indirect IF (IIF) | Circulating IgG anti-cell-surface antibodies on monkey esophagus substrate |
| ELISA (gold standard) | Anti-Dsg1 and/or anti-Dsg3 antibodies; titers correlate with disease activity |
Differential Diagnosis (key distinctions)
| Feature | Pemphigus Vulgaris | Bullous Pemphigoid |
|---|---|---|
| Blisters | Flaccid | Tense |
| Oral lesions | Common (>95%) | Uncommon |
| Nikolsky sign | Positive | Negative |
| Level of split | Suprabasilar (intraepidermal) | Sub-epidermal |
| Autoantigen | Dsg1/Dsg3 | BP180/BP230 |
| IF pattern | Intercellular | Linear BMZ |
Management
Principles
- PV should be treated at onset — even if limited, it will generalize; early disease is easier to control; delayed therapy increases mortality
- Goal: suppress autoantibody production → halt acantholysis → control disease → achieve remission
First-line Therapy
Rituximab (anti-CD20 monoclonal antibody) — now considered first-line for moderate-to-severe PV
- Depletes B cells → reduces anti-Dsg autoantibody production
- Complete remission off immunosuppressives in 50–90% of PV patients after 1+ courses
- Significantly superior to prednisolone alone in the landmark RITUX 3 trial
Systemic corticosteroids (prednisone/prednisolone)
- Historically the mainstay; still used as adjunctive therapy
- Starting dose typically 0.5–1 mg/kg/day; tapered once disease controlled
- Before glucocorticoids, PV was almost invariably fatal
Steroid-sparing Immunosuppressives (adjuvants)
| Drug | Notes |
|---|---|
| Azathioprine | Most commonly used adjuvant; reduces steroid dose/relapse risk |
| Mycophenolate mofetil | Alternative to azathioprine |
| Cyclophosphamide | For refractory disease |
| Dapsone | Adjunctive; some evidence in mild disease |
| Methotrexate | Less commonly used |
Other Therapies
- IVIg (intravenous immunoglobulin) — rapidly reduces antibody levels; used in refractory cases or acute severe disease
- Plasmapheresis — removes circulating antibodies; used with immunosuppressives to prevent rebound
- Topical corticosteroids — for localized or mild disease, especially oral
Emerging/Investigational
- BTK inhibitors (e.g., PRN1008/rilzabrutinib) — block mature B cell survival
- FcRn blockers (efgartigimod/ARGX-113) — accelerate IgG catabolism → rapidly lower autoantibody levels
- CAAR-T cell therapy — chimeric autoantibody receptor T cells expressing Dsg3, programmed to selectively kill Dsg3-specific B cells; preclinical success, disease-specific without broad immunosuppression
Prognosis
| Era/Therapy | Outcome |
|---|---|
| Pre-glucocorticoids | Almost universally fatal |
| Glucocorticoids + immunosuppressives | 10-year mortality ~10%; complete remission in ~17–50% |
| Rituximab era | Complete remission in 50–90%; achieved more quickly |
- Cause of death: most often infection (from the immunosuppressive therapy itself)
- Annual mortality rate (USA): ~0.023 per 100,000
- Inpatient mortality: 1.6–3.2%
- Risk of death 2.4–3.3× higher than controls (UK, Taiwan data)
Summary Mnemonic: "PEMPHIGUS"
| Letter | Feature |
|---|---|
| Painful oral erosions — first sign | |
| Epidermal split suprabasilar | |
| Mucous membranes universally involved | |
| Pathogenic IgG vs Dsg1/Dsg3 | |
| Historically fatal; now treatable | |
| IgG intercellular IF pattern ("fishnet") | |
| Glucocorticoids + rituximab first-line | |
| Ulcerations/erosions (no scar, hyperpigmentation) | |
| Suprabasilar acantholysis + tombstone sign |
Sources: Dermatology 2-Volume Set 5e (Bolognia et al.), pp. 614–620; Fitzpatrick's Dermatology, pp. 939–955
This is a shared conversation. Sign in to Orris to start your own chat.