Perforater of lower limb
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have very comprehensive data. Let me compile the full answer.
Perforators of the Lower Limb
Perforator (communicating/perforating) veins connect the superficial venous system to the deep venous system by piercing the deep fascia. Under normal circumstances, blood flows from superficial to deep (inward), aided by valves. When these valves become incompetent, high intramuscular pressures (150-200 mmHg during calf contraction) are transmitted to the superficial system, causing venous hypertension.
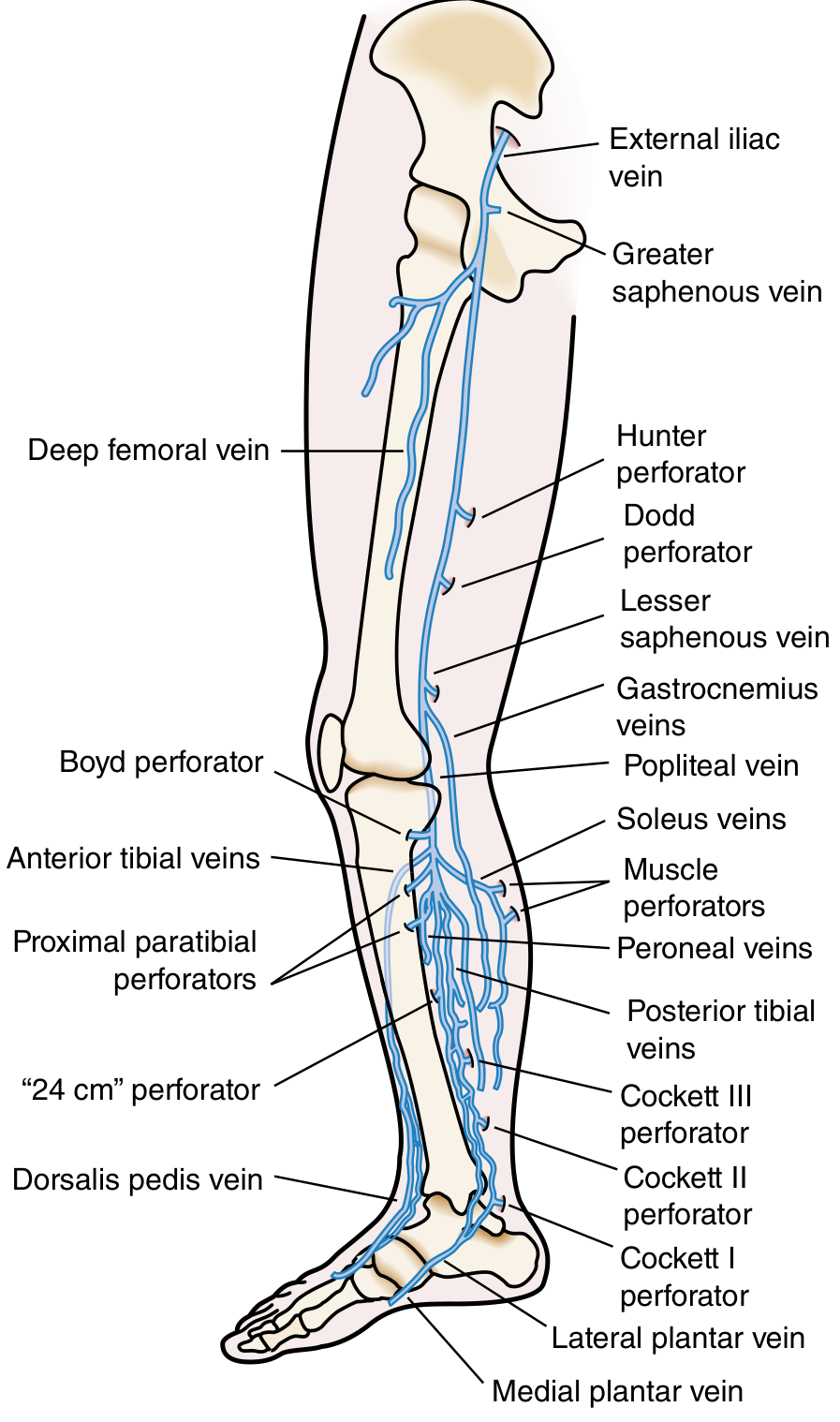
Perforating veins of the lower limb (Sabiston Textbook of Surgery)
Classification by Location
The lower limb is divided into three main regions for perforators:
1. Thigh Perforators
| Name (Modern) | Old Eponym | Connection | Level |
|---|---|---|---|
| Femoral canal perforators | Dodd (distal) / Hunter (mid-thigh) | GSV → femoral vein | Mid-to-distal thigh |
| Inguinal perforators | - | GSV → femoral vein | Proximal thigh |
| Posterior thigh perforators | - | Posteromedial / posterolateral thigh tributaries | Posterior thigh |
- Hunter perforator: upper thigh, connecting GSV to femoral vein through the adductor (Hunter's) canal
- Dodd perforator: lower thigh, connecting GSV to the popliteal or femoral vein
2. Knee Perforators
| Name | Connection |
|---|---|
| Popliteal fossa perforator | SSV (small saphenous vein) to popliteal vein |
| Boyd perforator (paratibial) | GSV → posterior tibial veins, upper medial leg (just below knee) |
| Medial/lateral knee perforators | Various superficial tributaries to deep system |
3. Leg Perforators
These are the most clinically important, especially the medial group:
| Name (Modern) | Old Eponym | Connection | Level |
|---|---|---|---|
| Posterior tibial perforators | Cockett I, II, III | Posterior arch vein → posterior tibial veins | Distal/mid medial leg |
| Paratibial perforators | Boyd | GSV → posterior tibial veins | Upper 1/3 medial leg |
| Gastrocnemius perforators | - | SSV → gastrocnemius veins | Posterior leg |
| Intergemellar perforators | - | SSV → soleal vein | Posterior leg |
| Para-Achillean perforators | - | SSV → fibular veins | Posterior leg |
| Anterior perforators | - | Anterior tributaries → anterior tibial veins | Anterior leg |
Cockett perforators (posterior tibial perforators) are the most clinically significant. Cockett I is near the ankle (~7 cm above the medial malleolus), Cockett II at ~13 cm, and Cockett III at ~18 cm.
Anatomy and Normal Physiology
- Perforators pierce the deep fascia at defined anatomical points; fascial defects (gaps/pits) can be palpated when incompetent
- They contain bicuspid valves that normally direct flow from superficial to deep
- The calf muscle pump generates pressures of 150-200 mmHg during exercise; competent perforators shield the superficial system from this pressure
- Valves are most numerous distally; the IVC, common iliac veins, and cranial sinuses are valveless
Incompetent Perforators - Pathophysiology
When perforator valves fail:
- High deep compartment pressure is transmitted outward to superficial veins
- Superficial venous hypertension develops
- Results in: varicose veins, skin changes (lipodermatosclerosis, haemosiderin pigmentation), venous eczema, and ultimately venous ulceration
The most common site for venous ulcer is above the medial malleolus, over Cockett's perforator - classic "gaiter area."
Clinical Tests for Incompetent Perforators
| Test | Principle |
|---|---|
| Brodie-Trendelenburg test | Tourniquet at SFJ: slow fill from below = incompetent perforators; rapid fill from above when released = SFJ incompetence |
| Tourniquet test (multiple levels) | Tourniquet moved down leg in steps to localize the level of the incompetent communicating vein |
| Fegan's method | Palpate along varicosities with leg elevated - fascial gaps/pits indicate perforator sites |
| Perthes' test | Tests deep vein patency; filling with tourniquet on calf + exercise = deep obstruction |
| Schwartz test | Percussion wave transmitted along vein = absent/incompetent valves |
| Morrissey's cough impulse test | Expansile impulse at saphenous opening on coughing = SFJ incompetence |
Key sites of incompetence in LSV system (S. Das):
- Sapheno-femoral junction (most important)
- Mid-thigh perforator
- Lower-thigh perforator
- Lower leg perforators on the medial side (Cockett's)
Surgical Relevance
- Subfascial endoscopic perforator surgery (SEPS): minimally invasive ligation of incompetent perforators
- Fegan's technique: sclerotherapy at identified perforator sites
- Open ligation (Linton's procedure): historical, rarely done now
- Duplex ultrasound is the investigation of choice for mapping incompetent perforators pre-operatively
- CEAP classification (C0-C6) grades chronic venous disease severity; perforator incompetence commonly contributes to C4-C6
Sources:
- Sabiston Textbook of Surgery, p. 2401 (Perforating veins of the lower limb diagram and physiology)
- Schwartz's Principles of Surgery, p. 1009 (Named perforators, modern nomenclature table)
- Gray's Anatomy for Students (varicose veins and perforating vein physiology)
- S. Das Manual on Clinical Surgery, 13th Ed., pp. 106-108 (clinical tests for perforators)
- Fitzpatrick's Dermatology (full classification table of named perforators)
This is a shared conversation. Sign in to Orris to start your own chat.