Explain me 10 common heart diseases with ECG changes and ECG images of those diseases
Reading File
Finding Sources
Finding Sources
Searching the Web
common heart diseases ECG changes with ECG images labeled educational
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Searching the Web
atrial fibrillation ventricular tachycardia heart block WPW pericarditis LVH ECG images labeled free educational
Reading Web Page
https://litfl.com/atrial-fibrillation-ecg-library
Searching the Web
site:litfl.com ECG STEMI WPW pericarditis LVH bundle branch block
Loading Image
Loading Image
Loading Image
Searching the Web
STEMI anterior inferior ECG image litfl pericarditis ECG diffuse ST elevation WPW delta wave ECG image
Loading Image
Loading Image
Loading Image
Loading Image
I now have enough textbook content and ECG images to write a comprehensive, detailed answer. Let me compile everything:
10 Common Heart Diseases: ECG Changes and Images
Below is a detailed guide to 10 major cardiac conditions, their hallmark ECG changes, and representative ECG tracings. Each ECG is sourced from the LITFL ECG Library (a peer-reviewed free open-access resource) or authoritative medical textbooks (Ganong's, Harrison's).
1. ST-Elevation Myocardial Infarction (STEMI)
Pathophysiology: Complete occlusion of a coronary artery causes transmural ischemia. Three simultaneous electrical events occur - rapid repolarization, decreased resting membrane potential, and delayed depolarization - all producing ST elevation in overlying leads.
ECG Changes (by phase):
| Phase | ECG Finding |
|---|---|
| Hyperacute (minutes) | Tall, peaked "hyperacute" T waves |
| Acute (hours) | ST elevation (convex/tombstone shape) in affected leads; reciprocal ST depression opposite |
| Evolving (hours-days) | Q waves appear; T-wave inversion begins |
| Chronic (weeks+) | Persistent deep Q waves; isoelectric ST; symmetric T-wave inversion |
Lead localization:
- Anterior STEMI: V1-V4 (LAD occlusion)
- Inferior STEMI: II, III, aVF (RCA or LCx occlusion)
- Lateral STEMI: I, aVL, V5-V6
- Posterior STEMI: tall R in V1-V2 with ST depression (mirror image)
Serial ECG changes in anterior infarction (Ganong's Review of Medical Physiology - textbook Figure 29-17):
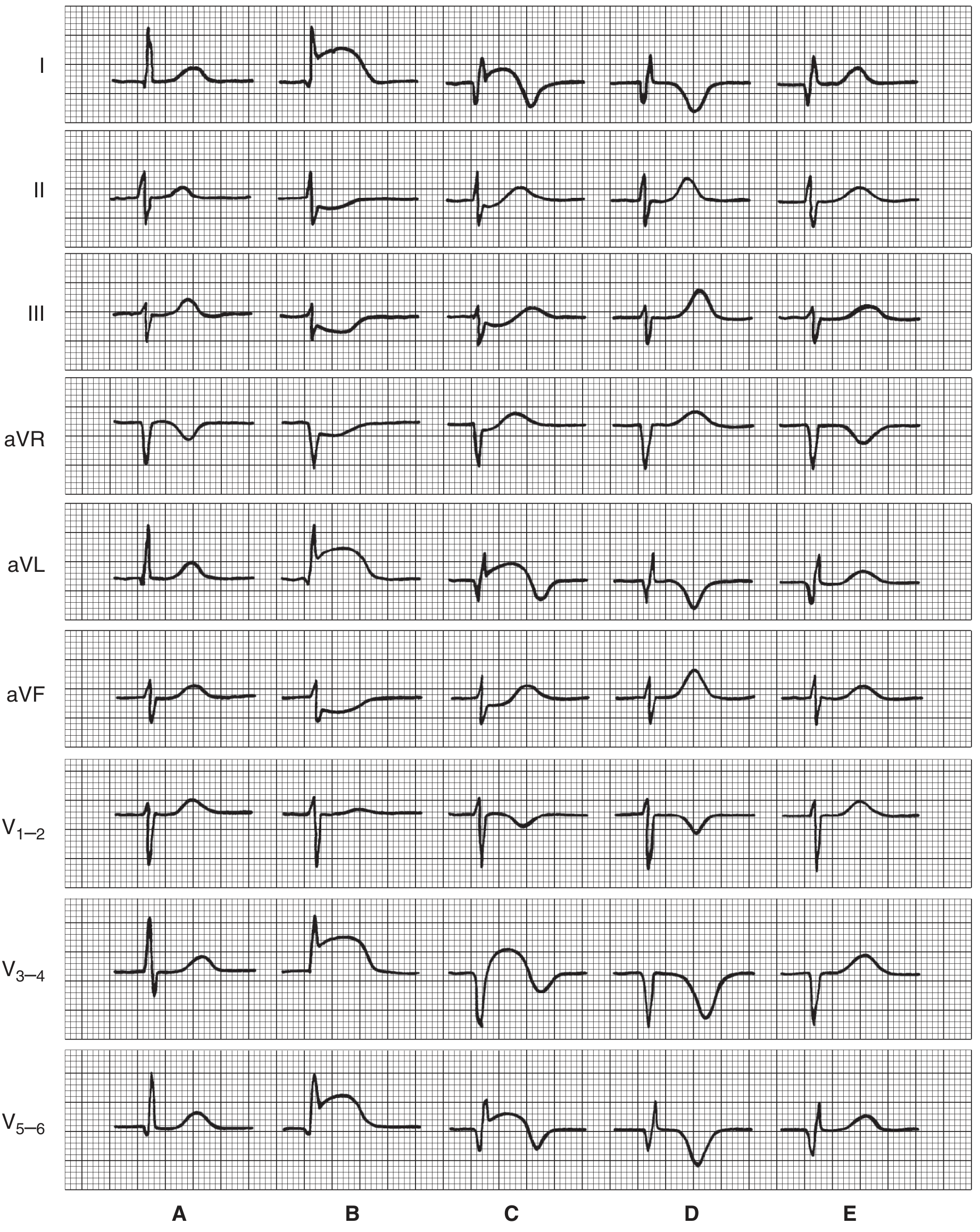
Serial ECG patterns in anterior infarction: (A) Normal baseline; (B) Early ST elevation in I, aVL, V3-5 with reciprocal depression in III/aVF; (C) Q waves and QS complexes appear in V3-4; (D) Persistent Q waves, isoelectric ST, deep T-wave inversion; (E) Late normalization possible.
Inferior STEMI ECG example (LITFL ECG Library):
Key features: ST elevation in II, III, aVF; reciprocal ST depression in I and aVL (mirror image of lead III).
2. Non-ST-Elevation MI / Unstable Angina (NSTEMI/ACS)
Pathophysiology: Partial coronary occlusion causing subendocardial ischemia without full-thickness infarction. Biomarkers (troponin) are elevated in NSTEMI but not in unstable angina.
ECG Changes:
- ST depression (horizontal or downsloping) - most common finding
- T-wave inversion, especially in anterior leads (Wellens' syndrome pattern when in V2-V3 = proximal LAD stenosis warning)
- No ST elevation, no new Q waves
- May be a completely normal ECG (does NOT exclude NSTEMI)
- Dynamic changes (evolving over serial ECGs) are diagnostically important
Key pattern - Wellens' Syndrome: Deep symmetrical T-wave inversions or biphasic T waves in V2-V3 indicate critical proximal LAD stenosis; patient is at high risk of massive anterior MI.
3. Atrial Fibrillation (AF)
Pathophysiology: Chaotic, disorganized atrial electrical activity from multiple re-entrant wavelets. Requires an initiating trigger (often pulmonary vein ectopy) and a substrate (dilated atrium, fibrosis).
ECG Changes:
- No discernible P waves - replaced by irregular fibrillatory baseline (f waves, 350-600/min)
- Irregularly irregular ventricular response - hallmark finding
- Narrow QRS complexes (unless aberrant conduction or pre-excitation)
- Ventricular rate varies (controlled = 60-100 bpm; rapid response = >100 bpm)
- Fibrillatory baseline may be coarse (coarse AF) or fine
AF ECG - Rhythm Strip (LITFL ECG Library):
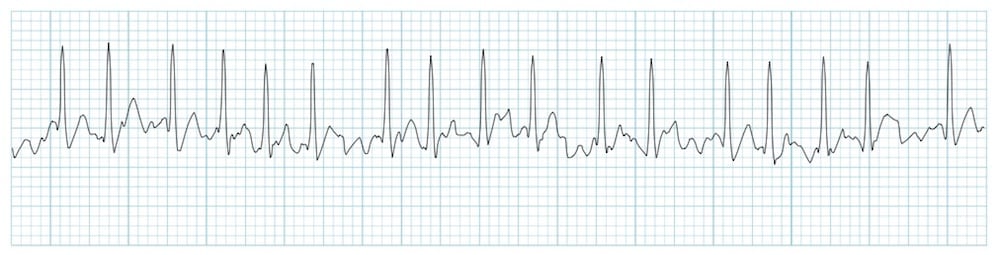
Key features: Absent P waves, irregular fibrillatory baseline, completely irregular R-R intervals (irregularly irregular), narrow QRS complexes.
4. Ventricular Tachycardia (VT)
Pathophysiology: Three or more consecutive ventricular beats at >100 bpm, originating from ventricular myocardium (below the bundle of His). Most commonly due to re-entry around scar tissue from prior MI.
ECG Changes (monomorphic VT):
- Wide QRS complexes (>120 ms), rate 100-250 bpm
- Regular rhythm
- AV dissociation (P waves march through at different rate) - pathognomonic when seen
- Fusion beats (partial capture) and capture beats (full sinus capture) = diagnostic
- Concordance: All precordial leads pointing same direction (positive = positive concordance; negative = negative concordance)
- Brugada criteria, Josephson sign (notching near nadir of S wave), Vergovich sign help differentiate from SVT with aberrancy
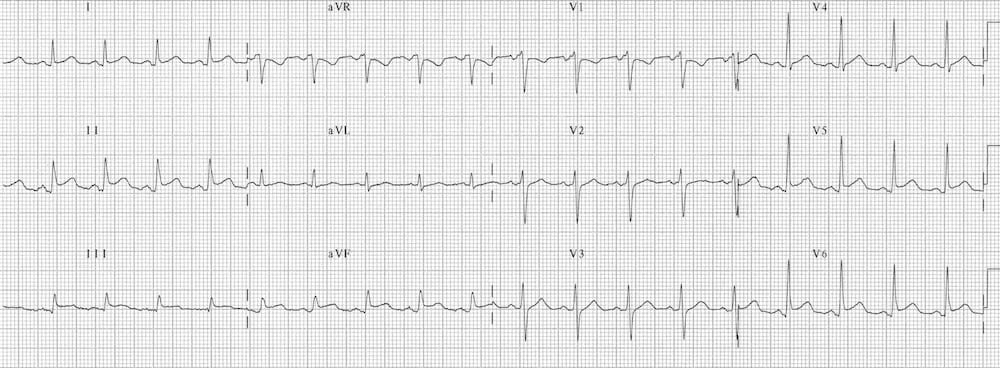
Monomorphic VT ECG (LITFL ECG Library):

Key features: Regular wide-complex tachycardia (QRS >120 ms), rate ~180 bpm. All QRS complexes identical (monomorphic). No visible P waves.
5. Complete (Third-Degree) Heart Block
Pathophysiology: Complete failure of atrial impulses to conduct to ventricles. Atria and ventricles beat independently - atria driven by SA node; ventricles by a subsidiary pacemaker (junctional or ventricular escape).
ECG Changes:
- Complete AV dissociation - P waves and QRS bear no relationship to each other
- P waves regular at normal/near-normal rate (60-100 bpm)
- QRS complexes regular but slow (escape rhythm):
- Junctional escape: narrow QRS at 40-60 bpm
- Ventricular escape: wide QRS at 20-40 bpm
- P wave "marching through" QRS complexes without capturing them
- The PP interval and RR interval are both regular but independent
Pericarditis ECG (12-lead showing diffuse changes):
(See pericarditis section below for full interpretation)
6. Acute Pericarditis
Pathophysiology: Inflammation of the pericardium causes epicardial myocarditis producing widespread repolarization abnormalities. The pattern evolves through four stages.
ECG Changes (4 stages):
| Stage | Timing | ECG Finding |
|---|---|---|
| Stage 1 | Days 1-2 | Widespread concave ("saddle-shaped") ST elevation in most leads (I, II, III, aVL, aVF, V2-6); PR depression (pathognomonic); ST elevation in aVR |
| Stage 2 | Days 3-7 | ST and PR normalize |
| Stage 3 | Week 1-3 | Diffuse T-wave inversions |
| Stage 4 | Weeks-months | ECG normalizes |
Key distinguishing features from STEMI:
- Concave (not convex) ST elevation
- PR depression (not seen in STEMI)
- No reciprocal ST depression (except aVR)
- Affects multiple territories simultaneously
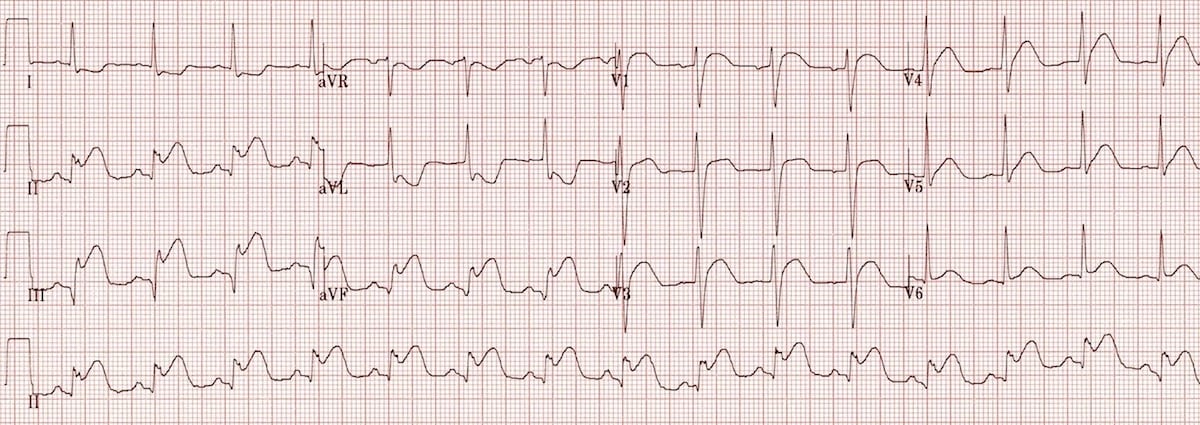
Pericarditis 12-lead ECG (LITFL ECG Library):
Key features: Diffuse concave ST elevation in I, II, aVL, V2-V6; PR segment depression especially in lead II; ST elevation in II > III (distinguishes from inferior STEMI where III > II). No reciprocal depression.
7. Left Ventricular Hypertrophy (LVH)
Pathophysiology: Increased LV muscle mass produces greater electrical forces directed leftward and posteriorly, amplifying voltages. Secondary repolarization abnormalities (the "strain" pattern) occur due to subendocardial ischemia.
ECG Changes (Sokolow-Lyon criteria most commonly used):
- High voltage: SV1 + RV5 or RV6 >35 mm (Sokolow-Lyon); RaVL >11 mm
- Left axis deviation (QRS axis -30° or more leftward)
- Repolarization abnormalities (LVH strain pattern):
- ST depression + asymmetric T-wave inversion in lateral leads (I, aVL, V5-V6)
- ST elevation in V1-V3
- Left atrial enlargement (broad notched P wave in II, biphasic P in V1)
- Prolonged QRS (may progress to LBBB)
Note from Harrison's: Prominent precordial voltages alone are a common normal variant in young/athletic individuals; repolarization abnormalities increase specificity for true LVH.
8. Left Bundle Branch Block (LBBB)
Pathophysiology: Failure of conduction in the left bundle branch forces abnormal activation of the LV - the right ventricle depolarizes first, then septum is activated from right to left (reversed), then LV depolarizes late via slow cell-to-cell spread.
ECG Changes:
- QRS duration ≥120 ms (complete LBBB)
- Broad, notched ("M-shaped") R wave in lateral leads (I, aVL, V5-V6) - the classic "M" pattern
- Deep, broad S wave or QS pattern in V1 - rS or QS
- No septal Q waves in lateral leads (I, aVL, V5-V6)
- Discordant ST/T changes - ST/T waves always opposite to main QRS deflection (secondary repolarization abnormality)
- Left axis deviation common
Clinical significance: New LBBB in a patient with chest pain = treat as STEMI equivalent until proven otherwise (Sgarbossa criteria help identify MI in LBBB).
9. Wolff-Parkinson-White (WPW) Syndrome
Pathophysiology: An accessory pathway (Bundle of Kent) bypasses the AV node, pre-exciting part of the ventricle. This creates a characteristic resting ECG pattern and predisposes to re-entrant tachycardias.
ECG Changes (classic WPW pattern - sinus rhythm):
- Short PR interval (<120 ms) - early ventricular activation bypassing AV node delay
- Delta wave - slurred upstroke at beginning of QRS (slow cell-to-cell conduction from accessory pathway insertion)
- Widened QRS (>120 ms) due to fusion of normal + pre-excited activation
- Secondary ST-T changes discordant to QRS
- Pseudo-infarct patterns - delta waves can mimic Q waves (especially inferior leads)
During tachycardia:
- Orthodromic AVRT: narrow complex tachycardia (most common, 70%)
- Antidromic AVRT: wide complex tachycardia resembling VT (5-10%)
- AF with WPW: irregular wide complex tachycardia, very rapid (>250 bpm), irregular - extremely dangerous (risk of VF)
10. Pulmonary Embolism (PE) - Right Heart Strain
Pathophysiology: Massive PE causes acute right ventricular pressure overload, RV dilation, and right axis deviation. The infarcted/ischemic RV produces characteristic ECG patterns.
ECG Changes:
- Sinus tachycardia - most common finding (in >40% of cases)
- S1Q3T3 pattern - prominent S wave in lead I, Q wave + T-wave inversion in lead III (classical but present in only ~20%)
- New right bundle branch block (RBBB) - complete or incomplete
- Right axis deviation
- T-wave inversions in V1-V4 (RV strain pattern) - most sensitive finding
- Atrial fibrillation or flutter may occur
- Right atrial enlargement (tall peaked P waves in II, "P pulmonale")
- Low QRS voltage sometimes
Key point: A normal ECG does NOT exclude PE. The finding of T-wave inversions in V1-V4 in a tachycardic patient with dyspnea should raise strong suspicion.
Quick Reference Summary Table
| # | Condition | Key ECG Findings |
|---|---|---|
| 1 | STEMI | ST elevation (convex) in territory, reciprocal depression, Q waves evolve |
| 2 | NSTEMI/ACS | ST depression, T-wave inversion, dynamic changes, possibly normal |
| 3 | Atrial Fibrillation | Absent P waves, irregularly irregular rhythm, fibrillatory baseline |
| 4 | Ventricular Tachycardia | Wide complex tachycardia, AV dissociation, fusion/capture beats |
| 5 | Complete Heart Block | AV dissociation, slow escape rhythm, P waves march independently |
| 6 | Pericarditis | Diffuse concave ST elevation, PR depression, no reciprocal changes |
| 7 | LVH | High voltage (SV1+RV5>35mm), strain pattern (ST depression/T inversion laterally) |
| 8 | LBBB | QRS ≥120ms, M-shaped R in lateral leads, no septal Q, discordant ST-T |
| 9 | WPW | Short PR, delta wave, wide QRS, pseudo-infarct pattern |
| 10 | Pulmonary Embolism | Sinus tachycardia, S1Q3T3, RBBB, T inversions V1-V4 |
Sources:
- Ganong's Review of Medical Physiology, 26th Edition (electrocardiographic changes in MI and ionic abnormalities)
- Harrison's Principles of Internal Medicine, 22nd Edition (LVH, bundle branch blocks, ischemia)
- LITFL ECG Library (Ed Burns, emergency physician) - peer-reviewed free open access ECG cases
- Tintinalli's Emergency Medicine & Goldman-Cecil Medicine (VT, arrhythmia, ACS)
This is a shared conversation. Sign in to Orris to start your own chat.