
20260601_184550.jpg
Interpret this ecg
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is the full interpretation of this ECG:
ECG Interpretation
Patient/Technical Details
- Date: 01-06-2026, recorded at Valluvanad Hospital
- Settings: 25 mm/s paper speed, 10 mm/mV gain, 0.67-25 Hz filter, AC50
- Machine-printed diagnosis: Sinus Arrhythmia + Ventricular Pre-excitation Type A
Measured Intervals (from printout)
| Parameter | Value |
|---|---|
| HR | 98 bpm |
| PR | 76 ms (short - normal is 120-200 ms) |
| QRS | 119 ms (widened - normal <100 ms) |
| QT/QTc | 364/467 ms |
| P/QRS/T axis | 36/40/0 degrees |
| RV5/SV1 | 0.83/4.0/0.000 mV |
Key ECG Findings
1. Short PR Interval (76 ms)
This is the hallmark of antegrade accessory pathway conduction. The normal AV node with its decremental conduction produces a PR of 120-200 ms. Here, the sinus impulse bypasses the AV node via the accessory pathway and reaches the ventricle almost immediately, producing this dramatically short PR.
2. Delta Wave + Widened QRS (119 ms)
Because the accessory pathway inserts directly into ventricular myocardium (which conducts slowly, cell-to-cell), the initial part of the QRS is a broad, slurred upstroke - the delta wave. Once the AV node conduction catches up, the His-Purkinje system rapidly activates the rest of the ventricle, creating an inflection point in the QRS. The result is a fusion beat - part preexcited (slow myocardial), part normal (fast Purkinje).
3. Type A WPW Pattern
Type A means the dominant QRS deflection in V1 is positive (tall R or R' in V1-V2). This indicates a left-sided accessory pathway (posteroseptal or left free wall), as the accessory pathway depolarizes the left ventricle first, generating a rightward/anterior initial vector that appears positive across V1-V2. This is confirmed by the machine-printed delta wave transition between V1 and V2 noted in the report.
- V1-V3: positive dominant R waves with slurred upstroke (delta waves)
- Inferior leads (II, III, aVF): upright complexes with delta waves
- aVR: negative delta waves (reciprocal)
4. Sinus Arrhythmia
The varying R-R intervals visible on the tracing reflect normal respiratory variation in sinus node firing rate - faster on inspiration, slower on expiration. This is a normal variant, especially common in younger patients.
5. Secondary ST-T Changes
ST depression and T-wave changes visible in left precordial leads are "secondary" changes - they result from the abnormal ventricular depolarization order, not from ischemia. Do not interpret these as ischemic.
Diagnosis
Wolff-Parkinson-White (WPW) Syndrome - Type A (Left-sided accessory pathway)
This is a manifest accessory pathway (conducts antegradely), producing the classic triad:
- Short PR interval (<120 ms)
- Delta wave (slurred QRS upstroke)
- Widened QRS (>100 ms)
Clinical Significance and What to Do Next
| Concern | Details |
|---|---|
| Risk of AVRT | Orthodromic AVRT (narrow QRS, most common) or antidromic AVRT (wide QRS) can occur |
| Risk of AF with rapid conduction | Up to 30% of WPW patients develop AF. If AF conducts down the accessory pathway, ventricular rates can reach 200-300 bpm and degenerate into VF - potentially fatal |
| Avoid AV nodal blockers in AF | Digoxin, verapamil, diltiazem, beta-blockers are contraindicated if AF with WPW occurs - they can unmask rapid accessory pathway conduction and cause VF |
| Definitive treatment | Radiofrequency catheter ablation of the accessory pathway is curative (>95% success rate) and is the first-line recommendation for symptomatic patients |
| Risk stratification | Electrophysiology (EP) study to assess the effective refractory period (ERP) of the accessory pathway - a short ERP (<250 ms) indicates higher risk for sudden death |
| Acute tachycardia | Orthodromic AVRT: adenosine/vagal maneuvers. Antidromic or pre-excited AF: procainamide or electrical cardioversion. Never give AV nodal blockers for wide-complex tachycardia in WPW |
Reference: Classic WPW ECG from Braunwald's Heart Disease
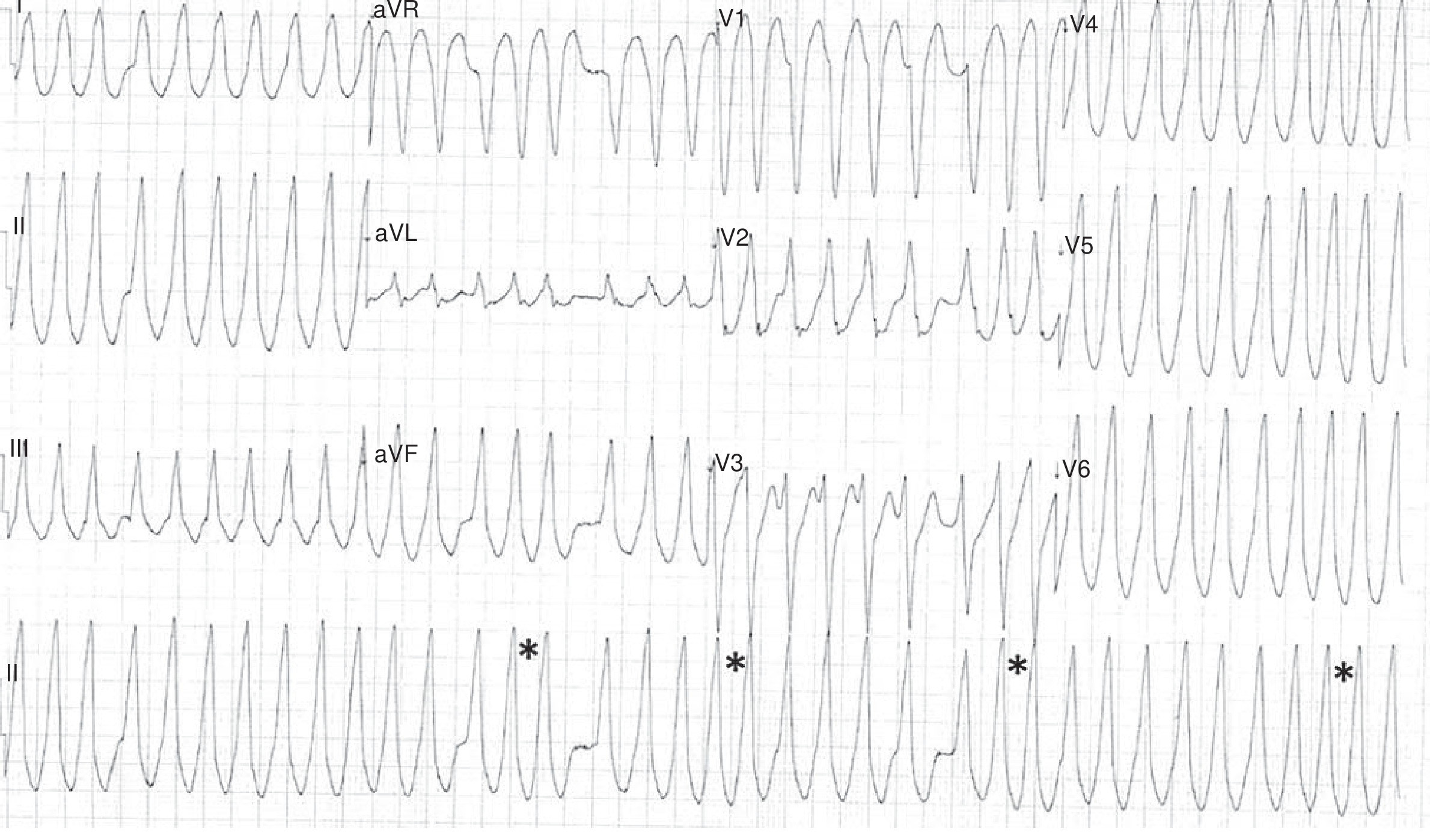
Reference ECG from Braunwald's Heart Disease showing WPW with preexcited AF - asterisks () indicate dangerously short R-R intervals (~240 ms). Your patient's tracing shows resting sinus rhythm with preexcitation, not tachycardia at this point, which is the favorable finding.*
Bottom line: This ECG shows classic WPW Type A in sinus rhythm. The patient should be referred to a cardiologist/electrophysiologist for risk stratification and likely catheter ablation, even if currently asymptomatic. The left-sided pathway localization guides the ablation approach (typically transseptal or retrograde aortic).
Sources: Braunwald's Heart Disease 12e, p.511-512; Rosen's Emergency Medicine 10e, p.1058
Disclaimer: This interpretation is for educational purposes. Clinical decisions must be confirmed by a qualified physician reviewing the original tracing in the context of the patient's full clinical picture.
This is a shared conversation. Sign in to Orris to start your own chat.