Why in neurosurgery no need of anaesthesia
awake craniotomy neurosurgery no general anaesthesia reasons
Clarifying the Premise
Why the Brain Itself Feels No Pain
What is Awake Craniotomy?
- Speech and language (Broca's and Wernicke's areas, usually left hemisphere)
- Motor function (primary motor cortex)
- Sensory function (primary sensory cortex)
- Memory (mesial temporal structures)
"Awake craniotomy allows for speech, motor, or sensory cortical mapping in real time, hence facilitating a more aggressive resection of the tumor and minimizing risk to function."
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e
"Awake craniotomies are performed when tumors or epileptic foci lie close to cortical areas required for either speech or motor function, or to mesial-temporal structures critical to short-term memory."
- Miller's Anesthesia, 10e
How is the Patient Managed (If Not Under GA)?
1. Scalp Nerve Block / Field Block
- Supratrochlear nerve
- Supraorbital nerve
- Zygomaticotemporal nerve
- Auriculotemporal nerve
- Lesser occipital nerve
- Greater occipital nerve
2. Sedation Techniques
| Technique | Description |
|---|---|
| Sedation throughout | Patient lightly sedated the entire time (propofol, dexmedetomidine, or remifentanil infusions) |
| Asleep-Awake-Asleep | General anaesthesia (with supraglottic airway) for opening and closing; airway device removed during the mapping phase so the patient can speak and respond |
3. Intraoperative Cortical Mapping
Conditions Treated with Awake Craniotomy
- Brain tumours near eloquent cortex (especially gliomas)
- Epilepsy surgery (resection of seizure foci in temporal lobe)
- Arteriovenous malformations near speech/motor areas
Complications to Watch For
- Disinhibited or uncooperative patient
- Oversedation (unable to complete neuropsychological testing)
- Respiratory depression / airway obstruction
- Intractable brain oedema
- Intraoperative seizures - treated with cold saline poured on the cortex + small bolus of propofol (20 mg IV)
- Uncontrollable pain
Key Takeaway
How to read pet scan image
how to read interpret PET scan image FDG radiology guide
How to Read a PET Scan Image
1. What a PET Scan Actually Measures
- FDG is injected intravenously
- Cells with high glucose demand (cancer, inflammation, active brain, heart) absorb more FDG
- Unlike real glucose, FDG gets trapped inside the cell after phosphorylation - it cannot be metabolised further
- Trapped FDG emits positrons, which produce pairs of gamma rays detected by the scanner
- A 3D map of metabolic activity is reconstructed
"FDG competes with glucose for transport into the cell and for enzymatic phosphorylation by hexokinase. Unlike glucose, once phosphorylated to FDG-6-phosphate, it does not undergo further metabolism and is trapped inside the cell."
- Fishman's Pulmonary Diseases and Disorders
2. The Colour Scale (Colour Map)
| Colour (hot scale) | Meaning |
|---|---|
| Black / dark blue | No or minimal uptake (metabolically inactive) |
| Green / yellow | Moderate uptake |
| Orange / red / white | Very high uptake ("hot spot") |
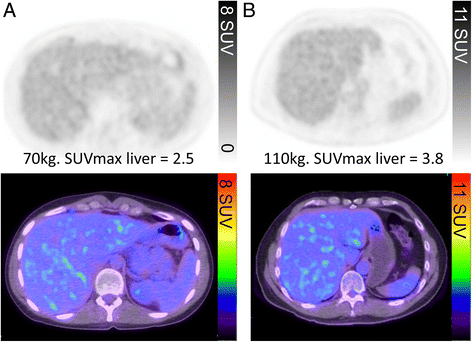
3. The SUV - The Most Important Number
SUV = Tracer uptake in region (MBq/mL) ÷ [Administered activity (MBq) / Body weight (kg)]
| Metric | What it means |
|---|---|
| SUVmax | Highest uptake in a single pixel (voxel) within the region - reflects the most aggressive part of a tumour |
| SUVmean | Average uptake across the whole region - correlates with overall tumour aggressiveness and survival |
- SUV < 2.5 - generally considered benign (e.g. pulmonary nodule)
- SUV 2.5 - 4 - equivocal, needs clinical correlation
- SUV > 4-5 - suspicious for malignancy in most contexts
- SUV of lymphoma, aggressive cancers - can exceed 10-20
4. PET/CT - Reading the Fusion
- PET alone shows WHERE metabolic activity is (but the anatomy is blurry)
- CT shows the precise anatomical structure
- Fused PET/CT tells you BOTH what is metabolically active AND exactly where it is
| Step | What to do |
|---|---|
| 1. Look at the CT first | Identify normal anatomy and any structural abnormality |
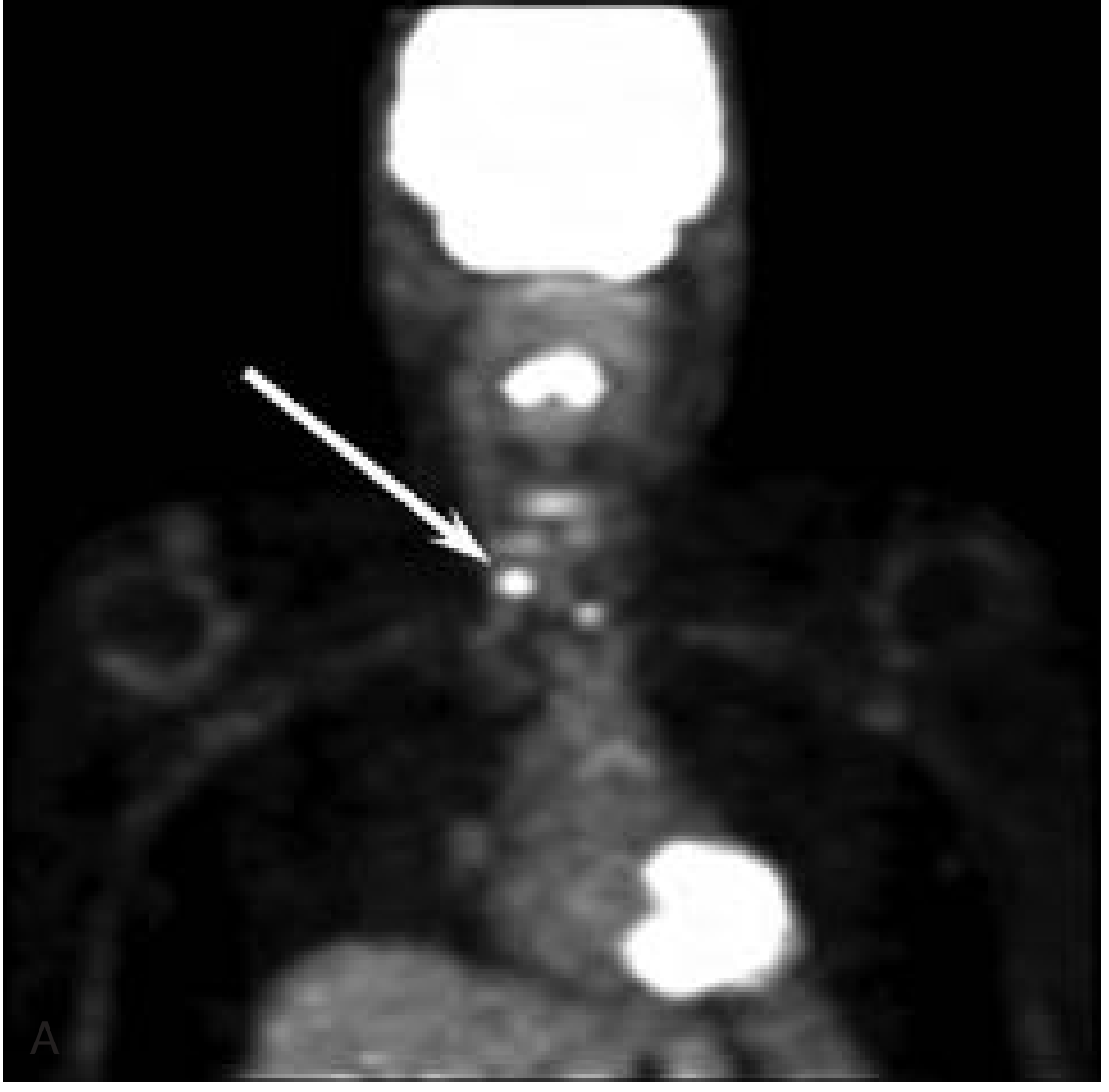
| 2. Look at PET (MIP) | Maximum Intensity Projection - a whole-body rotating 3D view - scan top to bottom for any hot spots |
| 3. Check normal structures | Confirm expected physiologic uptake is present (brain, heart, liver, kidneys, bladder) |
| 4. Flag abnormal uptake | Any area brighter than surrounding tissue or reference organ (usually liver) |
| 5. Fuse and localise | Use fused images to place abnormal uptake in its exact anatomical location |
| 6. Measure SUV | Read the SUVmax of flagged lesions |
5. Normal (Physiologic) Uptake - Do NOT Mistake These for Disease
| Structure | Why it's hot |
|---|---|
| Brain (cortex) | High baseline glucose metabolism |
| Heart (myocardium) | Especially in fed state; uses glucose as fuel |
| Liver | Background uptake - used as reference standard |
| Spleen | Moderate uptake |
| Kidneys and ureters | FDG is excreted in urine |
| Urinary bladder | Very hot - FDG accumulates here |
| GI tract (variable) | Bowel wall can show uptake |
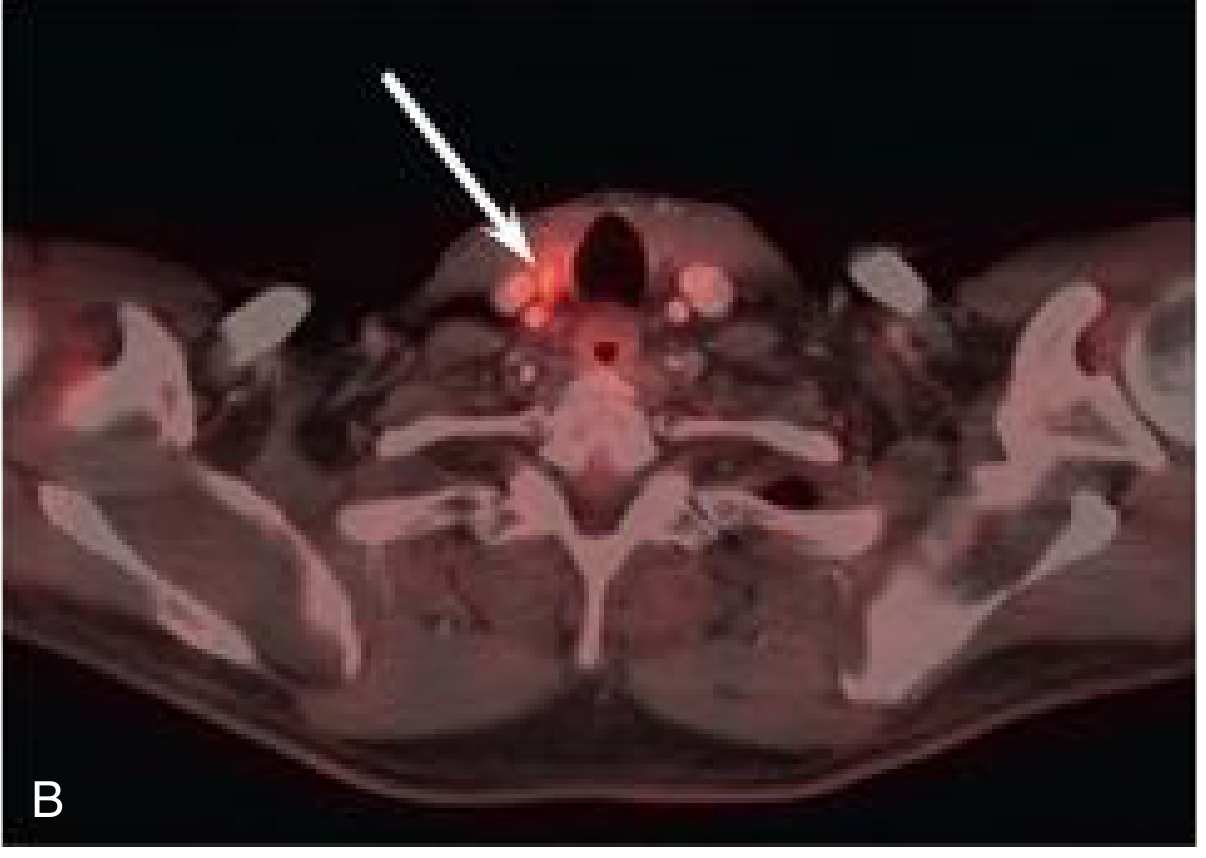
| Vocal cords / neck muscles | If patient was talking - can mimic tumour |
| Brown fat (neck/supraclavicular) | In cold conditions, especially young patients |
"Physiologic uptake of FDG is prevalent in the head and neck, especially during contraction of muscles (e.g., neck and thyroarytenoid muscles), and it may therefore be confused with tumor uptake."
- Cummings Otolaryngology Head and Neck Surgery
6. Causes of False Positives and False Negatives
False Positives (uptake that is NOT cancer):
- Infection / abscess - inflammatory cells have the same high glucose metabolism as cancer
- Post-surgical inflammation - scan should not be done until 8+ weeks after therapy
- Benign tumours (e.g. brown fat, sarcoidosis, thyroid disease)
- Muscle activity - patient was moving/tense during scan
False Negatives (cancer that is NOT seen):
- Hyperglycemia - high blood glucose competes with FDG for uptake, reducing signal (this is why patients must fast 4-6 hours before the scan)
- Well-differentiated / low-grade tumours - less metabolically active (e.g. mucinous CRC, some prostate cancers)
- Small lesions < 10 mm - below resolution threshold
- Slowly growing tumours (carcinoid, some thyroid cancers)
7. Key Advanced Metrics
| Metric | Definition | Use |
|---|---|---|
| MTV (Metabolic Tumour Volume) | Volume of tissue with pathologically elevated FDG in 3D | Reflects total tumour burden |
| TLG (Total Lesion Glycolysis) | SUVmean × MTV | Best overall predictor of prognosis |
| SUVmax | Peak voxel uptake | Most commonly reported |
| Dual time-point imaging | Scan at 1h AND 2h post-injection | Malignant lesions keep rising; benign lesions plateau or drop |
8. Common Non-FDG Tracers (Beyond Glucose)
| Tracer | Target | Clinical use |
|---|---|---|
| 18F-DOPA | Dopamine synthesis | Parkinson's disease, gliomas |
| 18F-FET (fluoroethyl-L-tyrosine) | Amino acid transport | Brain tumour recurrence vs radiation necrosis |
| 68Ga-DOTATATE | Somatostatin receptors | Neuroendocrine tumours |
| Amyloid tracers | Beta-amyloid plaques | Alzheimer's disease |
| TAU tracers | TAU protein | Frontotemporal dementia |
| PSMA | Prostate-specific membrane antigen | Prostate cancer staging/recurrence |
Summary
- Identify hot spots - any focal area of increased uptake beyond background
- Decide if it is physiologic or pathologic - know your normal structures
- Quantify with SUV - number gives you an objective measure of metabolic intensity
- Sources: Fishman's Pulmonary Diseases and Disorders, Cummings Otolaryngology Head and Neck Surgery, Scott-Brown's Otorhinolaryngology, Current Surgical Therapy 14e, Grainger & Allison's Diagnostic Radiology
I want Ga 68 PSMA image reading full body scan with bony metastasis
Ga-68 PSMA PET CT full body scan bone metastasis prostate cancer reading interpretation
"PSMA PET" "bone metastasis" prostate cancer
https://pmc.ncbi.nlm.nih.gov/articles/PMC7067527
Ga-68 PSMA PET/CT Full Body Scan: Complete Reading Guide with Bony Metastasis
1. What is PSMA and Why it Works
- Binds directly to cancer cells (not just bone reaction like a bone scan)
- Rapid clearance from non-target tissue = high tumour-to-background contrast
- Works even at very low PSA levels (detects disease where conventional imaging cannot)
- Now FDA approved for intermediate- and high-risk prostate cancer staging and biochemical recurrence
"68Ga-PSMA PET scans have shown promise in identifying nodal and bone metastasis that would have otherwise been missed with conventional CT scans."
- Smith and Tanagho's General Urology, 19e
"This scan is now FDA approved for patients with intermediate- and high-risk prostate cancer and is substantially more sensitive and accurate in the detection of metastases compared to conventional imaging."
- Harrison's Principles of Internal Medicine, 22e
2. Normal Physiologic Uptake on Ga-68 PSMA (What You Expect to See)
| Structure | Uptake level | Reason |
|---|---|---|
| Salivary glands (parotid, submandibular) | Very high (intense bilateral) | PSMA expressed in normal salivary glands - hallmark of normal scan |
| Lacrimal glands | Moderate-high | PSMA expression in glandular tissue |
| Liver | Moderate | Used as background reference |
| Spleen | Moderate | |
| Kidneys and ureters | High - excreted via kidneys | Renal clearance pathway |
| Urinary bladder | Very high (pooled tracer) | Urinary excretion - can obscure pelvic disease |
| Small bowel | Variable, mild | PSMA expressed in duodenal mucosa |
| Blood vessels (vascular walls) | Mild - related to neovasculature | PSMA on tumour neovasculature |
| Ganglia (celiac, sympathetic chain) | Focal uptake - mimics nodes | Important pitfall |
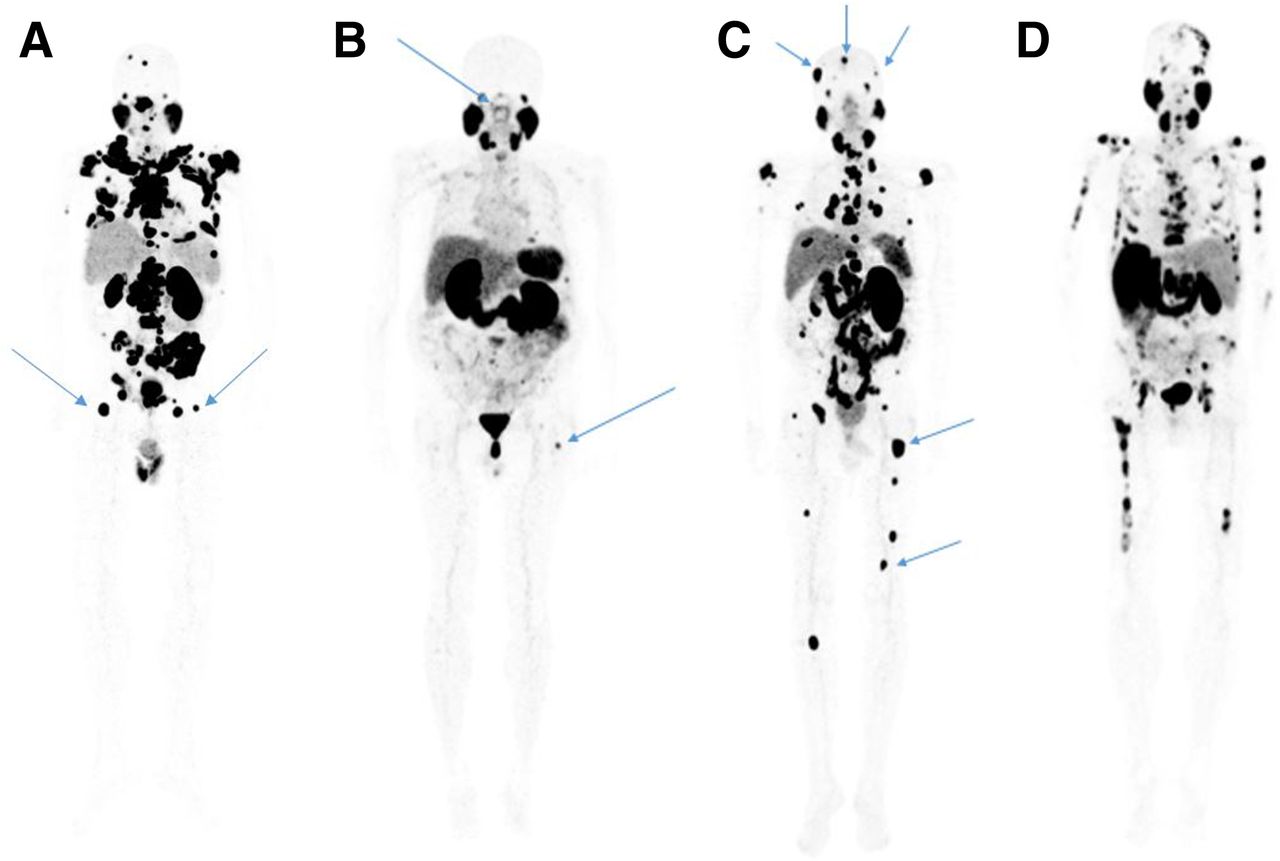
3. How to Read the MIP (Maximum Intensity Projection) - The First View

- Orient yourself - identify salivary glands (top), liver/spleen (mid-abdomen), kidneys (flanks), bladder (pelvis)
- Scan top to bottom - skull, cervical spine, thorax/ribs, thoracic spine, lumbar spine, pelvis, femora
- Mark any hot spot outside of expected physiologic uptake
- Note symmetry - bilateral symmetric uptake = usually benign; asymmetric focal = suspicious
- Fuse with CT - every suspicious PET finding must be localised on CT to confirm bony vs. soft tissue
4. Distribution of Bone Metastases on PSMA PET
Where Bone Metastases Appear - in Order of Frequency
| Bone Region | Frequency (among patients with bone mets) |
|---|---|
| Pelvis (ilium, sacrum, pubis, ischium) | 70% - most common |
| Ribs, clavicle, sternum | 59% |
| Spine (vertebral bodies) | 57% |
| Skull | Less common |
| Long bones (femur, humerus) | Less common - but important to include in FOV |
What a Bone Metastasis Looks Like
- On MIP: A focal dark spot (greyscale inversion - hot = dark on standard PSMA display) outside of normal physiologic sites
- On PET axial slice: Focal intense PSMA uptake
- On fused PET/CT: The PET hot spot colocalises with either:
- A sclerotic lesion on CT (blastic met - white on CT)
- A lytic lesion on CT (dark/destructive on CT)
- No visible CT change (early micrometastasis - PSMA detects before CT changes occur)
PSMA detects bone metastases by targeting the cancer cells directly, not the bone reaction. This is why it detects early lesions that are invisible to conventional bone scan.
5. PSA Level and Bone Metastasis Detection Rate
| PSA Level | Bone Metastasis Detection Rate |
|---|---|
| < 5 ng/mL | 17.6% |
| 5-10 ng/mL | 34.4% |
| 10-20 ng/mL | 40.8% |
| > 20 ng/mL | 41.4% |
6. Interpreting the Bone Lesion - What to Report
| Parameter | What to assess |
|---|---|
| Location | Exact bone, region (e.g., L3 vertebral body, right iliac wing) |
| SUVmax | Quantify uptake intensity |
| CT correlate | Sclerotic / lytic / no CT change |
| Number of lesions | Oligometastatic (1-3) vs. polymetastatic (4-5) vs. widespread (>5) |
| Cortical breach | Any risk of pathological fracture? |
| Cord involvement | Vertebral mets - is the spinal canal compromised? |
Oligometastatic vs. Widespread Disease - Clinical Significance
| Disease burden | Definition | Clinical impact |
|---|---|---|
| Solitary lesion | 1 bone met | May be eligible for SBRT / metastasis-directed therapy |
| Oligometastatic | 2-3 lesions | Still potentially curable with aggressive focal therapy |
| Polymetastatic | 4-5 lesions | Systemic therapy preferred |
| Widespread | >5 lesions | Systemic therapy; Lu-177 PSMA theranostics option |
7. PSMA vs. Conventional Bone Scan - Head-to-Head
| Modality | Sensitivity | Specificity |
|---|---|---|
| Ga-68 PSMA PET | Higher | Higher |
| Tc-99m bone scan | Lower | Lower (false positives from trauma, arthritis) |
- Bone scan detects osteoblastic reaction (indirect signal) - misses early lesions and lytic metastases
- PSMA PET detects cancer cells directly - positive even before bone reaction starts
- Bone scan cannot detect nodal or visceral disease simultaneously
- PSMA PET is a whole-body staging tool in one examination
8. Pitfalls and False Positives to Know
| Pitfall | What it looks like | How to differentiate |
|---|---|---|
| Sympathetic ganglia (celiac, stellate) | Focal uptake mimicking a node or met | Typical location, no CT lesion, bilateral symmetric |
| Paget's disease | Very high bone uptake | CT shows classic expanded coarsened trabeculae |
| Fracture / healing bone | Mild uptake | CT shows fracture line; no aggressive bone destruction |
| Haemangioma | Vertebral focal uptake | CT shows classic striated "corduroy" pattern |
| Ureter/urine contamination | Linear activity in pelvis | Follow on sequential images; activity moves |
| Bladder masking pelvic nodes/prostate bed | Bladder obscures uptake nearby | Late imaging or furosemide flush to empty bladder |
9. Theranostics - PSMA as Treatment
- 177Lu-PSMA-617 (Lutetium-177) - beta emitter for treatment of metastatic CRPC
- 225Ac-PSMA (Actinium-225) - alpha emitter for more resistant disease
"A targeted radio-ligand therapy, 177Lu-PSMA-617, targets prostate-specific membrane antigen, which is highly expressed in prostate cancer, as demonstrated by a positive prostate-specific membrane antigen PET."
- Goldman-Cecil Medicine
10. Reporting Checklist for a Full Body Ga-68 PSMA Scan
- PSMA-avid lesion in prostate/bed? SUVmax?
- Pelvic nodes (internal iliac, external iliac, obturator, presacral)
- Para-aortic / retroperitoneal nodes
- Mediastinal / supraclavicular nodes
- Skull and calvarium
- Cervical spine (C1-C7)
- Thoracic spine (T1-T12)
- Ribs and sternum, clavicles
- Lumbar spine (L1-L5)
- Sacrum and pelvis (iliac wings, acetabulum, pubis, ischium)
- Proximal femora and humeri
- Distal long bones (if total-body FOV)
- Liver, lung, adrenal lesions
In t12 metastasis seen 18
Ga-68 PSMA PET SUVmax 18 T12 bone metastasis prostate cancer clinical significance management
T12 Metastasis with SUVmax 18 on Ga-68 PSMA PET - Full Interpretation
What This Finding Means
SUVmax of 18 - How Significant Is It?
| SUVmax Range on PSMA PET | Interpretation |
|---|---|
| < 3-4 | Likely benign / background level |
| 4 - 8 | Low-moderate PSMA avidity - equivocal, needs CT correlation |
| 8 - 15 | High PSMA avidity - strongly suspicious for metastasis |
| > 15 (your finding: 18) | Intensely PSMA-avid - confirmed malignant, highly aggressive |
PSMA is expressed 100-1000 fold higher in prostate cancer cells vs. normal tissue, giving very high lesion-to-background ratios. An SUVmax of 18 far exceeds physiologic background at any spinal level.
Why T12 Specifically Matters
"The thoracic spinal column is most commonly involved... Prostate and ovarian cancers occur disproportionately in the sacral and lumbar vertebrae, probably from spread through Batson's plexus, a network of veins along the anterior epidural space."
- Harrison's Principles of Internal Medicine, 22e
What to Look for on the Fused CT at T12
| CT finding at T12 | What it means |
|---|---|
| Sclerotic (dense/white) lesion | Blastic met - classic for prostate cancer; bone reacting to tumour |
| Lytic (dark/destructive) lesion | Less common in prostate; risk of collapse/fracture |
| Mixed sclerotic-lytic | Aggressive or treated lesion |
| No CT change | Early micrometastasis - PSMA detected it before bone reacts |
| Cortical breach / pedicle destruction | High fracture risk - urgent surgical/ortho-oncology review |
| Posterior element involvement | Risk of epidural extension and cord compression |
| Reduced vertebral height | Pathological compression fracture - urgent intervention |
Urgent Red Flags to Assess Clinically
- Back pain at T12 level (worse at night, with coughing/movement)
- Bilateral leg weakness or heaviness
- Numbness / tingling in lower limbs or saddle area
- Bowel or bladder dysfunction (conus = early sphincter involvement)
"Pain is usually the initial symptom of spinal metastasis; it may be aching and localized or sharp and radiating... A recent onset of persistent back pain, particularly if in the thoracic spine (which is uncommonly involved by spondylosis), should prompt consideration of vertebral metastasis."
- Harrison's Principles of Internal Medicine, 22e
"Up to 40% of patients who present with cord compression at one level are found to have asymptomatic epidural metastases elsewhere - imaging of the entire length of the spine is important."
- Harrison's Principles of Internal Medicine, 22e
Mandatory Next Step: MRI Spine
- Epidural extension (tumour pushing into the spinal canal)
- Degree of cord compression if any
- Vertebral height and structural integrity
- Other unsuspected vertebral lesions not yet causing bone reaction
Clinical Management Pathway for T12 Met (SUVmax 18)
If This is the ONLY Bone Lesion (Oligometastatic)
| Option | Details |
|---|---|
| Stereotactic Body Radiotherapy (SBRT) | High-dose focused radiation to T12 in 1-5 fractions. Preferred for oligometastatic disease and radioresistant histology. Can sterilise the lesion. |
| Metastasis-directed therapy (MDT) | SBRT + continuation/intensification of systemic therapy |
| Surgery | If structural instability, cord compression, or radioresistance |
"Stereotactic body radiotherapy, which delivers high doses of focused radiation, is preferred for radioresistant tumor types and for patients requiring re-irradiation."
- Harrison's Principles of Internal Medicine, 22e
If Multiple Bone Lesions (Polymetastatic)
| Option | Details |
|---|---|
| Systemic therapy | ADT + abiraterone, enzalutamide, or docetaxel depending on castration status |
| 177Lu-PSMA-617 (Lutetium) | If PSMA-avid disease confirmed (SUVmax 18 qualifies strongly) - targeted radionuclide therapy |
| Palliative RT to T12 | If symptomatic - 8 Gy single fraction or 20 Gy/5 fractions for pain control |
| Zoledronic acid / Denosumab | Bone-protective agents to reduce skeletal-related events |
If Cord Compression Signs Present
- Dexamethasone 10 mg IV immediately - reduces cord oedema
- Maintain on dexamethasone 4 mg every 6 hours orally
- Urgent MRI whole spine - same day
- Urgent surgical/neurosurgical review - decompression if indicated
- Radiotherapy as definitive treatment post-surgery or as primary treatment
"Motor deficits (paraplegia or quadriplegia), once established for >12 h, do not usually improve, and beyond 48 h, the prognosis for substantial motor recovery is poor."
- Harrison's Principles of Internal Medicine, 22e
Summary Box
| Parameter | Your Findings | Clinical Significance |
|---|---|---|
| Tracer | Ga-68 PSMA | Directly targets prostate cancer cells |
| Location | T12 vertebra | Thoracolumbar junction - high-risk site |
| SUVmax | 18 | Intensely avid - unambiguous metastasis |
| Disease stage | M1b (bone metastasis) | Metastatic prostate cancer |
| Immediate next step | MRI whole spine | Assess cord compression, structural integrity |
| Urgent clinical check | Neurology exam | Rule out impending cord compression |
| Lu-177 eligibility | Yes (PSMA-avid confirmed) | Theranostic candidate if polymetastatic |
Which suture is good for injury over anterior leg by sharp object
best suture material anterior leg pretibial laceration sharp injury wound closure
https://emedicine.medscape.com/article/1127693-overview
Suture Choice for Sharp Laceration Over the Anterior Leg
Why the Anterior Leg is a Special Problem
- Skin here is thin, tightly adherent, with minimal subcutaneous fat
- Sits directly over the tibia with almost no subcutaneous cushion
- Blood supply is poor - the skin is a watershed zone
- Particularly in elderly patients, the skin is extremely fragile and tears easily around sutures
- High tension on wound edges (from oedema, dependent swelling)
- Healing is slow - on average 60 days even with good closure
- Minimally reactive (to avoid inflammatory breakdown)
- Non-cutting (monofilament preferred over braided to reduce drag)
- Tension-distributed (suture technique matters as much as material)
Recommended Suture: 3-0 or 4-0 Nylon (Monofilament Non-Absorbable)
First Choice: Monofilament Nylon (Ethilon / Dermalon)
| Property | Detail |
|---|---|
| Type | Non-absorbable, monofilament, synthetic |
| Size | 3-0 (thick/gaping wound) or 4-0 (standard laceration) |
| Tissue reaction | Very low - synthetic monofilament causes minimal inflammation |
| Tensile strength | High - retains up to 2/3 of strength even after 11 years in tissue |
| Infection risk | Low - single strand = no interstices for bacteria to harbour |
| Handling | Stiff, needs extra throws on knot (3-4 throws minimum) |
| Removal | Required at 10-14 days for lower leg (longer than face) |
"Nylon: General surgical use - skin closure, abdominal wall mass closure, hernia repair, plastic surgery, neurosurgery, microsurgery, ophthalmic surgery. Contraindications: None."
- Bailey and Love's Short Practice of Surgery, 28e
Second Choice: Polypropylene (Prolene / Surgipro)
What NOT to Use on the Anterior Leg
| Suture | Why to Avoid |
|---|---|
| Silk | High tissue reaction, promotes infection, moderate reactivity - unsuitable for routine skin closure. "Risk of infection and tissue reaction makes silk unsuitable for routine skin closure" - Bailey and Love |
| Braided polyester (Mersilene/Ethibond) | Multi-filament = bacterial wicking risk in a poorly vascularised area |
| Catgut / Chromic catgut | Unpredictable absorption, high tissue reaction, loses strength within 7-21 days - too early for a slow-healing pretibial wound |
| Vicryl (polyglactin) for skin | Absorbable - adequate strength only 2-3 weeks; anterior leg needs support for longer. Can cause suture abscess if used percutaneously |
| Staples | Avoid over thin pretibial skin - high risk of tearing; poor cosmesis |
Suture Size Guide for the Anterior Leg
| Wound | Size (USP) | Metric equivalent |
|---|---|---|
| Deep layer (if any subcutaneous tissue present) | 3-0 Vicryl (absorbable - buried) | Metric 2 |
| Skin closure - standard laceration | 3-0 or 4-0 Nylon | Metric 2 / 1.5 |
| Skin - thin elderly skin, delicate closure | 4-0 Nylon | Metric 1.5 |
| Very fine skin edges | 5-0 Nylon | Metric 1 |
"The distance of insertion from the edge of the wound should correspond to the thickness of the tissue being sutured. Each successive suture should be placed at twice this distance apart."
- Bailey and Love's Short Practice of Surgery, 28e
Best Technique: Simple Interrupted Sutures
- If one suture cuts through the fragile skin, the entire closure does not fail
- Allows wound inspection between sutures
- Can be selectively removed if infection develops
- Place sutures 5-8 mm apart and 5 mm from wound edge (adjust for tissue thickness)
- Do not tie too tightly - oedema will cause sutures to cut through if overtightened at the time of placement
Alternative Technique: Vertical Mattress Suture
- Evert the wound edges (reduces dead space)
- Distribute tension over a wider area (critical in thin pretibial skin)
- Prevent skin edge inversion which causes poor healing
"Mattress sutures... are very useful in producing an accurate approximation of wound edges, especially when the edges to be anastomosed are irregular in depth or disposition."
- Bailey and Love's Short Practice of Surgery, 28e
Deep Layer (If Wound is Deep)
- Use 3-0 Vicryl (polyglactin 910) as a buried absorbable deep layer first
- This reduces wound tension on the skin edges before nylon skin closure
- Vicryl retains ~60% tensile strength at 2 weeks, ~30% at 3 weeks
When NOT to Close Primarily (Important!)
- Wound is contaminated or > 6-8 hours old (risk of infection)
- Skin flap is ischaemic or purple/congested - primary closure will necrose
- Elderly/fragile skin with large flap - tension closure risks total flap loss
Summary Recommendation
| Decision | Answer |
|---|---|
| Best suture material | 3-0 or 4-0 Monofilament Nylon (Ethilon) |
| Alternative | 3-0 or 4-0 Polypropylene (Prolene) |
| Deep layer | 3-0 Vicryl (buried, absorbable) |
| Technique | Simple interrupted OR vertical mattress |
| Needle type | Cutting or reverse-cutting (for skin) |
| Suture removal | 12-14 days (longer than most body sites) |
| Avoid | Silk, catgut, braided materials, staples on thin pretibial skin |

Read this report and tell me the interpretation and how to treat and advise
AEC 1388 IgE >1000 eosinophilia high IgE causes investigation treatment young male
absolute eosinophil count 1388 IgE >1000 young adult workup treatment India parasitic
Lab Report Interpretation - Mr. Dhaval Dama, Male, 28 Years
The Two Key Findings at a Glance
| Test | Result | Normal | Severity |
|---|---|---|---|
| Absolute Eosinophil Count (AEC) | 1388 /cmm | 20-500 /cmm | 🔴 HIGH - nearly 3x upper limit |
| Total IgE (Immunoglobulin E) | >1000 IU/mL | ≤100 IU/mL | 🔴 MARKEDLY HIGH - 10x upper limit |
Understanding Each Finding
1. Elevated AEC = 1388 /cmm
| AEC Level | Grade |
|---|---|
| 500-1500 /cmm | Mild eosinophilia |
| 1500-5000 /cmm | Moderate eosinophilia |
| >5000 /cmm | Severe (Hypereosinophilic syndrome) |
- Parasitic (helminth) infections
- Allergic/atopic conditions
- Certain drugs and autoimmune conditions
"Eosinophilia is present if blood eosinophils exceed ~0.35-0.5 × 10⁹/L. Reactive eosinophilia is typically associated with allergic processes and parasitic infections."
- Henry's Clinical Diagnosis and Management by Laboratory Methods
2. Elevated Total IgE = >1000 IU/mL
- Mediates immediate hypersensitivity (Type I allergic) reactions
- Is produced in large quantities in response to helminthic parasites
- Triggers mast cell and basophil degranulation (allergic symptoms)
Why These Two Together Are Very Significant
"Moderate to severe peripheral eosinophilia is most commonly associated with infection by helminths, including nematodes, trematodes, and cestodes."
- Henry's Clinical Diagnosis and Management by Laboratory Methods
"Key causes of eosinophilia: Parasitic - trichinosis, filariasis, schistosomiasis; Allergic - urticaria, hay fever, asthma"
- Henry's Clinical Diagnosis (Box 34.4)
Differential Diagnosis - Most Likely to Least Likely
🔴 Most Likely: Parasitic (Helminthic) Infection
| Parasite | Why to consider | Clue |
|---|---|---|
| Roundworm (Ascaris lumbricoides) | Most common in India | Abdominal pain, vomiting |
| Hookworm (Ancylostoma/Necator) | Very common, rural India | Anaemia, soil contact |
| Toxocara canis/cati (Visceral Larva Migrans) | Dog/cat contact | Hepatomegaly, wheeze |
| Filariasis (Wuchereria bancrofti) | Endemic India - Gujarat | Limb swelling, nocturnal fever |
| Strongyloides stercoralis | Highest IgE elevation of all GI parasites | Diarrhoea, urticarial rash |
| Trichinella spiralis | Less common | Muscle pain, periorbital oedema |
🟡 Also Consider: Allergic / Atopic Conditions
- Bronchial asthma (exogenous/allergic type)
- Allergic rhinitis / hay fever
- Atopic dermatitis / eczema
- Urticaria
🟢 Less Likely but Must Rule Out
- Drug reaction (check current medications)
- Hyper-IgE syndrome (Job's syndrome) - rare, would have recurrent skin abscesses + IgE usually >2000
- Hodgkin lymphoma (if constitutional symptoms present)
- Churg-Strauss syndrome / EGPA (if asthma + systemic features)
What Further Investigations to Order
First-Line (Essential - Order Now)
| Investigation | What it detects |
|---|---|
| Stool for ova and cyst / parasites × 3 samples | Direct detection of GI helminths |
| Peripheral blood smear | Rule out filarial microfilariae; assess eosinophil morphology |
| CBC with differential | Full blood picture - rule out hypereosinophilic syndrome |
| Chest X-ray | Loeffler syndrome (migratory pulmonary infiltrates in larval migration) |
| Urine routine | Baseline; filariasis may cause chyluria |
Second-Line (Based on Clinical Suspicion)
| Investigation | What it detects |
|---|---|
| Serology: Toxocara ELISA | If abdominal pain/hepatomegaly/wheeze |
| Filarial antigen card test / nocturnal blood smear | If from filaria-endemic area (Gujarat can have cases) |
| Skin prick test / specific IgE (RAST) | If allergic cause suspected |
| Ultrasound abdomen | Liver/spleen for granulomas, eosinophilic infiltration |
| Spirometry | If asthma suspected |
| ANA, ANCA, ESR | If autoimmune/Churg-Strauss suspected |
Treatment
Step 1 - Empirical Anthelmintic Therapy
- Effective against: roundworm, hookworm, whipworm, Strongyloides, Toxocara
- Repeat dose after 2 weeks for hookworm/strongyloides
- Ivermectin 200 mcg/kg single dose - especially if Strongyloides suspected (causes very high IgE)
- Diethylcarbamazine (DEC) 6 mg/kg/day × 12 days - if filariasis suspected
Step 2 - Treat Allergic Component (if present)
| Drug | Dose | Purpose |
|---|---|---|
| Cetirizine / Levocetirizine | 10 mg / 5 mg OD at night | Antihistamine for allergic symptoms |
| Montelukast | 10 mg OD | Anti-leukotriene - especially if asthma component |
| Inhaled corticosteroid | If asthma confirmed on spirometry | Long-term controller |
Step 3 - If No Parasites Found (After Thorough Workup)
- Allergist/Immunologist - for specific IgE testing and allergy management
- Haematologist - if AEC rises > 1500 or organ involvement suspected (Hypereosinophilic syndrome)
Patient Advice (What to Tell Mr. Dhaval Dama)
🔵 Lifestyle and Hygiene
- Wash hands thoroughly before eating and after toilet
- Wear footwear always outdoors - especially in soil/garden areas (prevents hookworm entry through feet)
- Drink only boiled/filtered water - do not drink tap or well water directly
- Avoid eating unwashed raw vegetables and undercooked meat
- Deworm the entire household - all family members should take albendazole 400 mg single dose (as routine deworming)
- Pet hygiene - if dogs/cats at home, deworm pets regularly; wash hands after contact
🔵 Diet
- No raw/undercooked pork or meat (Trichinella, Taenia risk)
- Avoid walking barefoot in soil (especially after rain)
- Wash fruits and vegetables with clean water before eating
🔵 Symptoms to Watch For (Return Immediately)
| Symptom | Possible Reason |
|---|---|
| Swelling of limbs especially legs | Filariasis (lymphoedema) |
| Cough + difficulty breathing | Loeffler syndrome (larval migration) |
| Chest pain / palpitations | Eosinophilic myocarditis (if AEC rises) |
| Severe abdominal pain | Intestinal obstruction from worm load |
| Jaundice | Biliary ascariasis |
| Skin rash / urticaria | Allergic/larval migration |
🔵 Follow-Up
- Repeat AEC in 4-6 weeks after treatment - should fall significantly if parasitic cause
- Repeat IgE in 3 months - will take longer to normalise
- Bring stool report to follow-up visit
Summary for Clinician
| Point | Detail |
|---|---|
| Diagnosis | Likely parasitic eosinophilia (helminthic) with/without atopy |
| AEC severity | Mild-moderate (1388 /cmm) |
| IgE severity | Markedly elevated (>1000 - 10x normal) |
| Most urgent exclusion | Rule out hypereosinophilic syndrome if AEC >1500 or organ symptoms |
| First treatment | Albendazole 400 mg stat + repeat CBC in 4-6 weeks |
| Referral needed | Only if no improvement or AEC continues to rise |