Principlesof sclera buckling with complications
Reading File
Finding Sources
Finding Sources
Reading File
Searching Images
scleral buckling retinal detachment surgery
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content from Kanski's Clinical Ophthalmology. Let me compile the full answer.
Scleral Buckling: Principles and Complications
Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed.
Definition & Core Concept
Scleral buckling (SB) is an external (conventional) approach to retinal detachment (RD) surgery, in contrast to the internal approach of pars plana vitrectomy (PPV). An explant — a piece of soft or hard silicone — is sutured onto the outer sclera, creating an inward indentation called the buckle.
Dual Purpose
- Close retinal breaks by apposing the RPE (retinal pigment epithelium) to the detached sensory retina
- Reduce dynamic vitreoretinal traction at sites of local vitreoretinal adhesion
Scleral buckling is always indicated for retinal detachment secondary to post-traumatic dialysis.
Explant Specifications
| Feature | Detail |
|---|---|
| Material | Soft or hard silicone |
| Ideal coverage | ~2 mm of buckle surrounding the entire break |
| Anterior extent | Must cover the vitreous base anterior to the tear (prevents re-opening and anterior SRF leakage) |
| Size estimation | Break dimensions assessed by comparison with the optic disc diameter |
Buckle Configurations
- Radial — perpendicular to the limbus; good for U-tears
- Segmental — covers a localised area of breaks
- Circumferential — parallel to the limbus; spans multiple break locations
- Encircling — a 360° band around the globe
Configuration chosen depends on the size, shape, and number of retinal breaks.
Surgical Technique
- Peritomy — conjunctival incision for access
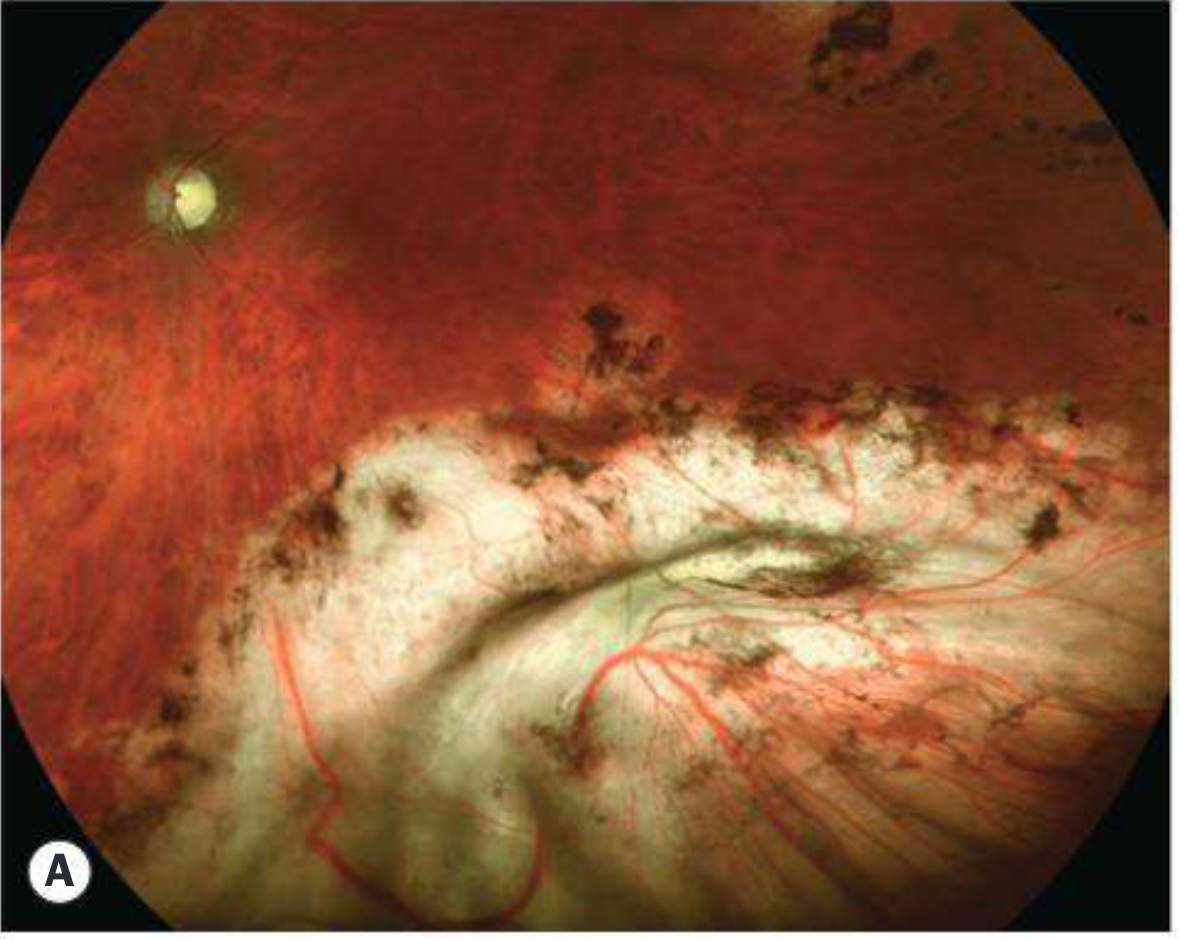
- Break localisation — breaks are identified and marked externally (Fig. 16.30A)
- Cryotherapy — applied around the break to create chorioretinal adhesion
- Explant placement — sutured to the sclera using mattress sutures; position of buckle checked relative to break (Fig. 16.30B–D)
- Verification — buckle height and position confirmed intraoperatively
Drainage of Subretinal Fluid (SRF)
SRF can be drained externally through the sclera (the D-ACE sequence: Drainage → Air → Cryotherapy → Explant).
Indications for SRF drainage:
- Bullous (high) detachment where the explant cannot adequately close the break without drainage
- Long-standing RD where SRF is viscous and slow to reabsorb
- Inferior breaks
- Elderly patients (slow reabsorption)
- Situations where postoperative position cannot be controlled (e.g., very young children)
Avoiding SRF drainage (non-drain technique) is preferred when possible as drainage carries its own risks (see below).
Complications
Intraoperative Complications
| Complication | Mechanism / Notes |
|---|---|
| Retinal incarceration | Retina gets sucked into the drainage sclerostomy site — a visually devastating complication |
| Subretinal haemorrhage | Choroidal vessel laceration during drainage; can be massive |
| Vitreous haemorrhage | From choroidal or retinal vessel trauma |
| Iatrogenic retinal break | From scleral suture perforation |
Postoperative Complications
Buckle/Explant-related:
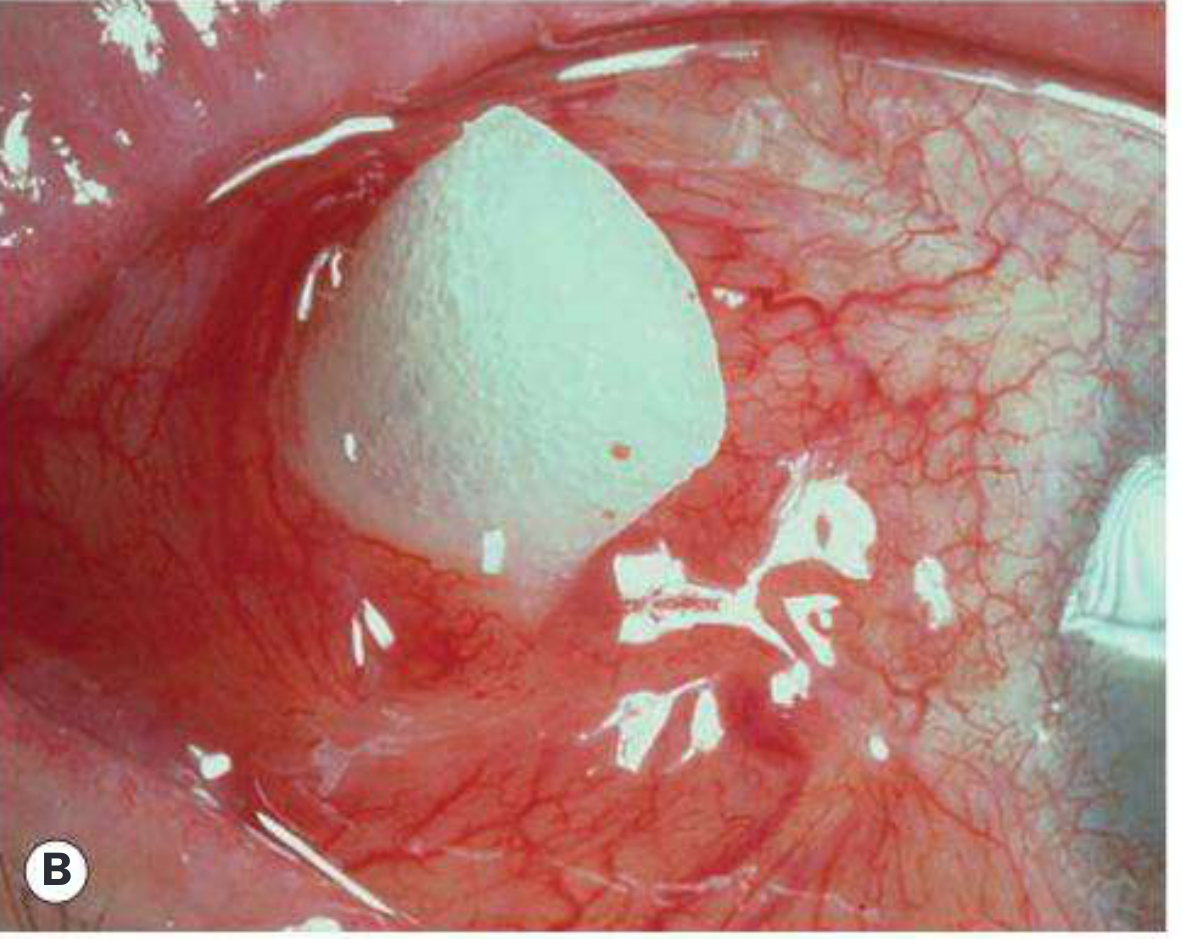
- Buckle extrusion — implant erodes through conjunctiva and becomes exposed (Fig. 16.32A — shows visible buckle material under conjunctiva)

- Buckle infection — requires explant removal
- Buckle migration — changes position over time
Ocular Motility:
- Diplopia / ocular motility disturbance — from extraocular muscle trauma, adhesion, or mechanical effect of an encircling band
- Induced myopia — axial length increase from the encircling band compressing the globe
Anterior Segment:
- Anterior segment ischaemia — from tightening of encircling band compromising anterior ciliary arteries; features: corneal oedema, anterior uveitis, iris ischaemia
- Raised intraocular pressure — angle closure or choroidal effusion
- Choroidal effusion — from vortex vein compression by the buckle
Posterior Segment:
- Macular pucker (epiretinal membrane) — postoperative fibrocellular proliferation
- Cystoid macular oedema — post-surgical inflammation
- "Fish-mouthing" — large superior equatorial U-tear widens following buckling in a bullous RD; the flaps gape open rather than close, requiring further intervention
Surgical Failure
| Cause | Notes |
|---|---|
| Inadequate buckle size | Break not fully supported |
| Incorrect positioning | Explant not aligned under the break |
| Inadequate buckle height | Can treat with SRF drainage or intravitreal gas injection; PPV may be preferred |
| Proliferative vitreoretinopathy (PVR) | Most common cause of late failure — tractional forces re-open old breaks and create new ones; typically presents weeks postop with re-detachment |
| Re-opening of break (no PVR) | Inadequate cryotherapy or buckling, or reduction of buckle height over time / after elective removal |
Key teaching point — The three commonest causes of failed retinal detachment surgery are:
- Proliferative vitreoretinopathy (PVR)
- Failure to close all breaks
- Development of new breaks
Contraindications to Scleral Buckling
PPV is preferred over scleral buckling when breaks are unlikely to be closed by buckling alone:
- Giant tears (≥ 90° circumference)
- Large posterior breaks
- Established PVR
— Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition, Chapter 16
More elaborate
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Diabetic retinopathy
Reading File
Finding Sources
Finding Sources
Diabetic retinopathy clinical research , net DR CR NET
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.