im preparing for ms ortho theory examinations knruhs and imn using manish kumar varshiney book guide me where to start
KNRUHS MS Orthopaedics theory examination syllabus pattern important topics
KNRUHS MS Ortho theory exam important topics previous question papers Manish Kumar Varshney
https://dokumen.pub/practical-orthopedic-examination-made-ea…
MS Ortho Theory Exam Guide - KNRUHS (Manish Kumar Varshney)
About the Book
- 2 Essays x 20 marks = 40
- 6 Short Notes x 10 marks = 60
- Total = 100 per paper
Where to Start - Priority Order
PHASE 1: Basic Sciences Foundation (Paper I / Part I)
| Topic | Why Important | Library Resource |
|---|---|---|
| Bone structure & healing | High-yield essay - fracture healing steps, callus | Miller's Review, Section 1 |
| Calcium & Phosphate metabolism | Short note staple | Miller's Review - Calcium/PTH/Vit D |
| Collagen types | Frequently asked short note | Miller's Review - Cartilage |
| Osteonecrosis (AVN) | Ficat classification, Cruess - perennial essay | Miller's Review |
| Muscle fiber types & physiology | Short note | Miller's Review - Muscle |
| Bone graft types | Very common | Campbell's Chapter 1 |
PHASE 2: Core Traumatology Topics (Paper - Traumatology)
- Fracture Neck of Femur - Classify + management in elderly (Garden's classification, hemiarthroplasty vs THA vs DHS)
- Fracture Distal Radius - Classification (Frykman, AO), management, recent advances
- Talus fractures - Hawkins classification, AVN risk, management
- ACL injuries - Anatomy of knee, investigations, reconstruction techniques
- Tibial plateau fractures - Schatzker classification, management
- Fracture Shaft Femur - Management, complications, IMN technique
- Calcaneum fractures - Essex-Lopresti, management
- Open fractures - Gustilo-Anderson, Byrd classification, management principles
- Compartment syndrome - Pathophysiology, diagnosis, fasciotomy
- Fat embolism syndrome - Gurd's criteria, management
- Monteggia fracture dislocation (Bado classification)
- Galeazzi fracture
- Colles fracture vs Smith's fracture
- Bohler's angle
- Talar neck fractures - Hawkins sign
- Principles of external fixation
- SIGN nail / Interlocking nail mechanics
PHASE 3: Core Orthopaedics Topics (Paper - Orthopaedics)
- TB of Hip - Classification, clinical features, investigations, management (Ironside classification, Oswestry staging)
- TB of Spine (Pott's disease) - Clinical features, complications (Pott's paraplegia - Seddon), management, surgery indications
- Osteosarcoma - Classification, staging (Enneking), clinical features, management
- Osteoarthritis of Knee - Pathology, classification, management (TKA)
- Congenital Talipes Equinovarus (CTEV/Clubfoot) - Ponseti method in detail
- Developmental Dysplasia of Hip (DDH) - Diagnosis, Ortolani/Barlow, management
- Legg-Calve-Perthes Disease - Herring classification, management
- Rheumatoid Arthritis - Joint involvement, medical management, surgical options
- Cervical spondylosis - Clinical features, management, indications for surgery
- Intervertebral disc prolapse (PIVD/PLID) - Pathology, clinical features, management
- Ewing's sarcoma vs Osteosarcoma
- Kocher's method (shoulder reduction)
- Thomas test / FABER test
- Scoliosis - Cobb angle measurement
- Spinal stenosis
- Limb length discrepancy assessment
- Bone tumour staging (Enneking system)
PHASE 4: Recent Advances Paper
- Arthroscopy - knee, shoulder principles and indications
- Total Knee/Hip Arthroplasty - fixation types, bearing surfaces, complications
- Ilizarov technique and principles
- Minimally invasive surgery in orthopaedics
- Bone substitutes and tissue engineering
- Navigation and robotic surgery (awareness level)
- Biological therapies - PRP, stem cells in orthopaedics
- Locked plating principles
How to Use Varshney's Book Effectively
- Chapter-wise theory content - read for concept clarity
- Chapter 11 (Long Questions for Theory Exams) - practice writing answers
- Chapter 12 (Short Notes) - revise in last 2 weeks before exam
Library Books Available to You Here
- Miller's Review of Orthopaedics 9th Edition - excellent for MCQ-style facts, classifications, tables. Use for basic sciences and quick revision.
- Campbell's Operative Orthopaedics 15th Edition (2026) - the gold standard reference. Use it to understand surgical techniques asked in essays.
- Rockwood and Green's Fractures in Adults 10th Ed (2025) - best for fracture classification and management.
Quick Tips for KNRUHS Theory
- Always start essays with a classification - examiners expect it upfront
- Draw diagrams for fracture patterns, surgical approaches - they fetch marks
- Mention complications - early and late, always
- Recent advances paragraph - add 4-5 lines on recent advances at the end of every essay, even in Paper I and II
- Scoring pattern is generous - structured answers with headings score better than prose
top 10 paper 2 questions in order of importance
KNRUHS NTR UHS MS Orthopaedics Paper 2 theory previous question papers repeated topics orthopaedics
https://www.scribd.com/document/986361758/2023-2025-Ortho-Qu…
MS ortho Paper 2 orthopaedics theory NTRUHS KNRUHS repeated questions TB hip spine osteosarcoma DDH scoliosis
https://orthopaedicprinciples.com
https://orthopaedicprinciples.com/pg-exam-questions-2026-a/
Paper II (Orthopaedic Diseases) - Top 10 Questions, Ranked by Importance
🥇 1. Tuberculosis of Spine (Pott's Disease)
- Pathology: paradiscal, central, anterior, appendageal types
- Pott's paraplegia - Seddon's classification (early onset vs late onset)
- Investigations: X-ray (gibbus), MRI findings, Mantoux, biopsy
- Medical management: HRZE regimen
- Surgical indications + approaches: anterior (transthoracic, retroperitoneal), posterior instrumentation
- Complications: cold abscess, gibbus, kyphosis
🥈 2. TB of Hip Joint
- Stages: synovial → early arthritis → advanced arthritis → fibrous/bony ankylosis
- Wandering acetabulum, pathological dislocation
- Investigations, medical Rx, surgical options (arthrodesis, THR timing)
- Ironside classification
🥉 3. Osteosarcoma
- Enneking staging (IA, IB, IIA, IIB, III)
- Codman's triangle, sunray appearance on X-ray
- Biopsy principles (Mankin's rules)
- Limb salvage surgery vs amputation
- Neoadjuvant chemotherapy: MAP protocol (Methotrexate, Adriamycin, Cisplatin)
- Survival rates, recent advances (mifamurtide)
4. Giant Cell Tumour (GCT)
- Campanacci grading (I, II, III)
- Histology: mononuclear stromal cells + osteoclast-like giant cells
- X-ray: soap bubble, eccentric epiphyseal lesion
- Management: extended curettage + cementation/bone graft vs resection
- Denosumab for unresectable/recurrent GCT
- Recurrence rate ~25%
5. Developmental Dysplasia of Hip (DDH)
- Embryology, risk factors
- Ortolani's test (reduction click), Barlow's test (dislocation click)
- Hilgenreiner's line, Perkin's line, acetabular index, Shenton's line
- Management by age: Pavlik harness (0-6 months), closed reduction + spica (6-18 months), open reduction (>18 months), osteotomies (>2 years)
- Salter's osteotomy, Dega, Pemberton - indications
6. Osteoarthritis of Knee / Total Knee Arthroplasty (TKA)
- Pathology of OA: cartilage loss, subchondral sclerosis, osteophytes
- Kellgren-Lawrence grading
- Conservative management → HTO indications → TKA
- TKA: components (femoral, tibial, patellar), cemented vs cementless, PCL retention vs substitution
- Complications: PE, infection, stiffness, loosening
7. Legg-Calve-Perthes Disease (LCPD)
- Age group 4-8 years, 4:1 male predominance
- Pathology: AVN of femoral head → fragmentation → healing → remodeling
- Catterall classification (I-IV), Herring lateral pillar classification (A/B/B-C/C)
- Stulberg outcome classification
- Management: containment (abduction brace, femoral/pelvic osteotomy)
- Poor prognosis signs: Gage sign, calcification lateral to epiphysis, lateral subluxation, horizontal physis
8. Cervical Spondylosis / Cervical Disc Prolapse
- Pathology: disc degeneration, osteophyte formation, ligamentum flavum hypertrophy
- Clinical features: neck pain, radiculopathy (dermatomal), myelopathy (long tract signs, Lhermitte's sign, Nurick grading)
- Investigations: MRI gold standard, CT for bony detail
- Conservative management
- Surgical: ACDF (anterior cervical discectomy and fusion), posterior laminectomy/laminoplasty - indications
- Nurick grading for myelopathy
9. Rheumatoid Arthritis (Hand / Wrist / Management)
- Pathology: synovitis → pannus → cartilage/bone destruction
- Deformities: ulnar drift, boutonniere, swan-neck, Z-thumb, caput ulnae
- Felty's syndrome, extra-articular features
- ACR diagnostic criteria
- DMARDs: Methotrexate first line, biologics (TNF-alpha inhibitors, rituximab)
- Surgical options: synovectomy, arthroplasty, arthrodesis
10. Osteomyelitis (Acute Haematogenous / Chronic)
- Pathogenesis: metaphyseal predilection, subperiosteal abscess, involucrum, sequestrum, cloacae
- Cierny-Mader classification (chronic OM)
- Organisms: S. aureus most common; Salmonella in sickle cell
- Investigations: X-ray (late), MRI (early - gold standard)
- Management: antibiotics (empirical then culture-guided), surgical debridement, sequestrectomy
- Sickle-cell osteomyelitis - special entity (April 2026 short note)
Bonus Short Notes to Prepare (in case essays are predictable)
- Scoliosis (Cobb angle, classification, management)
- AVN of femoral head - Ficat staging, management
- Ewing's sarcoma (vs Osteosarcoma table)
- Thoracic outlet syndrome
- High Tibial Osteotomy (HTO)
- Limb length discrepancy
- Brachial plexus injury
Search PubMed for recent TB spine surgical techniques and outcomes, i want paper 2 trauma
"spinal tuberculosis" AND "surgical treatment" AND outcomes
KNRUHS NTR UHS MS Ortho Paper 2 Traumatology theory repeated questions essays 2022 2023 2024 2025
PMID: 38087216
PMID: 41319734
"spinal tuberculosis" AND "anterior debridement" AND "posterior instrumentation"
MS Ortho Paper 2 Traumatology theory exam 2024 2025 2026 fracture neck femur tibial plateau pelvic fracture questions
PMID: 37694053
PMID: 36655386
"spinal tuberculosis" AND kyphosis AND correction
PMID: 37975989
PMID: 37736557
Part A: PubMed Evidence - TB Spine Surgical Techniques & Outcomes (2022-2026)
Key Finding Summary
| Study | Design | Key Message |
|---|---|---|
| Arifin et al. 2024 [PMID 37975989] | Systematic Review + Meta-analysis (20 cohort studies) | Anterior approach = faster surgery, less blood loss, better kyphosis correction, fewer complications vs posterior alone |
| Duan et al. 2023 [PMID 36655386] | Retrospective, 119 LTB patients | Single posterior = less traumatic, shorter op time; Combined P-A = faster abscess healing; Outcomes equivalent |
| Yadav et al. 2023 [PMID 37694053] | Prospective study, 30 patients | Single-stage anterior + posterior: 89.5% neurological recovery, mean kyphosis correction 6.98° |
| Deng et al. 2023 [PMID 38087216] | Meta-analysis (8 studies, 523 patients) | Titanium mesh vs bone graft: no significant difference in fusion, VAS, kyphosis correction - bone graft has less subsidence |
| Murhega et al. 2026 [PMID 41319734] | Systematic Review - Cervical TB | Surgery in 71.9% of cervical TB; bone fusion in 4.1 months; surgery mortality only 1.0% |
| Shanmuganathan (Rajasekaran) et al. 2023 [PMID 37736557] | Current updates review | MDR-TB rising; tissue PCR = gold standard; uncomplicated TB = medical Rx only; surgery cornerstones = debridement + deformity correction + stable fusion |
What to Write in Your Recent Advances Paragraph (for TB Spine Essay)
- Anterior approach has fewer complications and better kyphosis correction than posterior alone (Arifin et al., Spine Deformity 2024)
- Single posterior approach is gaining ground for lumbar TB - less trauma, equivalent neurological outcomes (Duan et al., Ortho Surg 2023)
- Single-stage combined anterior-posterior surgery gives 89.5% neurological recovery for tuberculous paraplegia (Yadav et al. 2023)
- Titanium mesh cage vs autologous bone graft - no significant difference in fusion rate, VAS, or kyphosis correction (Deng et al., BMC Surg 2023)
- Bone graft still preferred by some due to lower subsidence rates (RR 9.30 for mesh subsidence)
- MRI remains gold standard for early diagnosis
- Tissue PCR (Gene Xpert/Xpert MTB/RIF) is now gold standard for microbiological diagnosis - faster and detects rifampicin resistance
- Epidural/paravertebral abscess with cord involvement seen in 72.9% of cervical TB cases on MRI
- Rising MDR-TB is the biggest challenge to the WHO "End TB Strategy" (Rajasekaran et al. 2023)
Part B: Paper II (Traumatology) - Top 10 Questions in Order of Importance
🥇 1. Fracture Neck of Femur
- Garden's classification (I-IV); AO/OTA classification
- Blood supply of femoral head (Trueta) - ascending cervical branches, retinacular vessels
- Management by age + displacement: young patient (ORIF, DHS, cannulated screws) vs elderly displaced (hemiarthroplasty - Austin Moore/bipolar vs THA)
- Complications: AVN (30-35%), non-union, implant failure
- Recent advance: Femoral Neck System (FNS) - asked as short note April 2026 Paper IV
🥈 2. Tibial Plateau Fractures
- Schatzker classification (I-VI)
- Luo's Three-Column Theory (recent advance) - medial, lateral, posterior columns
- CT scan mandatory for surgical planning
- Management: conservative (undisplaced <3mm), ORIF (buttress plating), arthroscopy-assisted
- Complications: compartment syndrome, stiffness, post-traumatic OA, peroneal nerve injury
🥉 3. Pelvic Ring Fractures
- Young-Burgess classification (LC, APC, VS, CM types)
- Tile's classification (A stable, B rotationally unstable, C both unstable)
- ATLS resuscitation - life before limb
- Management: pelvic binder (first aid), external fixator (damage control), ORIF (definitive)
- Surgical approaches: Pfannenstiel (pubic symphysis), ilioinguinal approach, Kocher-Langenbeck (posterior)
- C-clamp for posterior ring instability
4. Open Fractures
- Gustilo-Anderson classification (Type I, II, IIIa, IIIb, IIIc) - know the criteria by heart
- Byrd and Spicer soft tissue classification
- 6-hour rule (historical) - current evidence: no strict time limit but early surgery preferred
- Management: ABC, wound debridement, fracture stabilisation (ex-fix in III), wound coverage
- Antibiotics: Type I/II = 1st gen cephalosporin; Type III = add gentamicin ± metronidazole
- Wound closure: primary (Type I), delayed primary (Type II), flap (Type IIIb)
5. Fracture Distal Radius
- Frykman classification, AO/OTA classification
- Colles (dorsal tilt), Smith's (volar tilt), Barton's (intraarticular), die-punch
- Acceptable reduction criteria (volar tilt 0-22°, radial inclination >15°, ulnar variance ≤+1mm)
- Management: cast (undisplaced), ORIF with volar locking plate (displaced/intraarticular)
- Complications: malunion, EPL rupture, CRPS, median nerve symptoms
- Recent advance: arthroscopic-assisted reduction
6. Compartment Syndrome
- Pathophysiology: rising ICP → ischaemia → muscle necrosis → Volkmann's ischaemia
- Clinical features: 6 P's (Pain, Pressure, Paraesthesia, Paralysis, Pallor, Pulselessness - last 2 late signs)
- Diagnosis: compartment pressure >30mmHg or within 30mmHg of diastolic BP
- Whitesides technique for pressure measurement
- Treatment: remove compressive dressings → fasciotomy (4-compartment leg fasciotomy through 2 incisions)
- Late complication: Volkmann's ischaemic contracture - Holden classification
7. Fractures of Talus
- Hawkins classification (I - undisplaced, II - subtalar subluxation, III - complete dislocation, IV - TNJ dislocation)
- Blood supply of talus - deltoid branch (most important), artery of tarsal canal, artery of sinus tarsi
- Hawkins sign (subchondral osteopenia at 6-8 weeks) = good prognostic sign, indicates viable bone
- AVN rate: Hawkins I = 0-13%, II = 20-50%, III = 80-100%
- Management: ORIF (displaced), conservative (undisplaced)
8. ACL Injury
- Anatomy: anteromedial and posterolateral bundles
- Clinical tests: Lachman test (most sensitive), anterior drawer test, pivot shift test
- MRI findings
- Conservative vs surgical (reconstruction - autograft choices: BPTB vs hamstring)
- Double bundle vs single bundle reconstruction
- ACL in children: transphyseal vs physeal-sparing technique (April 2026)
- Complications: graft failure, cyclops lesion, tunnel widening
9. Fracture Shaft of Femur
- AO classification (transverse, oblique, spiral, comminuted)
- Emergency management: Thomas splint, skin/skeletal traction
- Definitive: Closed IMN (interlocking nail) - standard of care
- Nail mechanics: static vs dynamic locking
- Fat embolism syndrome - Gurd's criteria
- Complications: malrotation, non-union, knee stiffness
10. Calcaneum Fractures
- Essex-Lopresti classification: joint-depression type vs tongue type
- Sanders classification (CT-based, I-IV)
- Bohler's angle (normal 25-40°, reduced in fractures)
- Gissane's angle (normal 120-145°)
- Management: conservative (undisplaced, elderly, diabetic), ORIF via extensile lateral approach (Sanders II-III)
- Complications: peroneal tendon injury, wound dehiscence (10-25%), malunion, subtalar OA
Bonus High-Yield Short Notes for Paper II Trauma
- TENS (Titanium Elastic Nail System) - asked April 2026
- Burst fracture D12 with neurological deficit - asked April 2026
- Posterior malleolus fracture - asked April 2026
- Pathological fractures + Mirel's score - asked April 2026
- Hoffa's fracture - asked April 2026
- Gamekeeper's thumb (UCL injury) - asked April 2026
- Monteggia fracture (Bado classification)
- Galeazzi fracture
- Fat embolism syndrome
- Floating knee injury
femoral head blood supply as an essay question structered answer and for viva 10 marks
Blood Supply of the Femoral Head
Structured Answer - 10 Marks (Essay + Viva Ready)
Introduction (1 mark)
Sources of Blood Supply (3 marks)
1. Medial Femoral Circumflex Artery (MFCA) - MOST IMPORTANT
- Branch of the deep femoral artery (profunda femoris), occasionally from the femoral artery directly
- Runs posteriorly between iliopsoas and pectineus, then between obturator externus and quadratus femoris
- At the superior border of quadratus femoris, it gives the deep branch which enters the posterior capsule
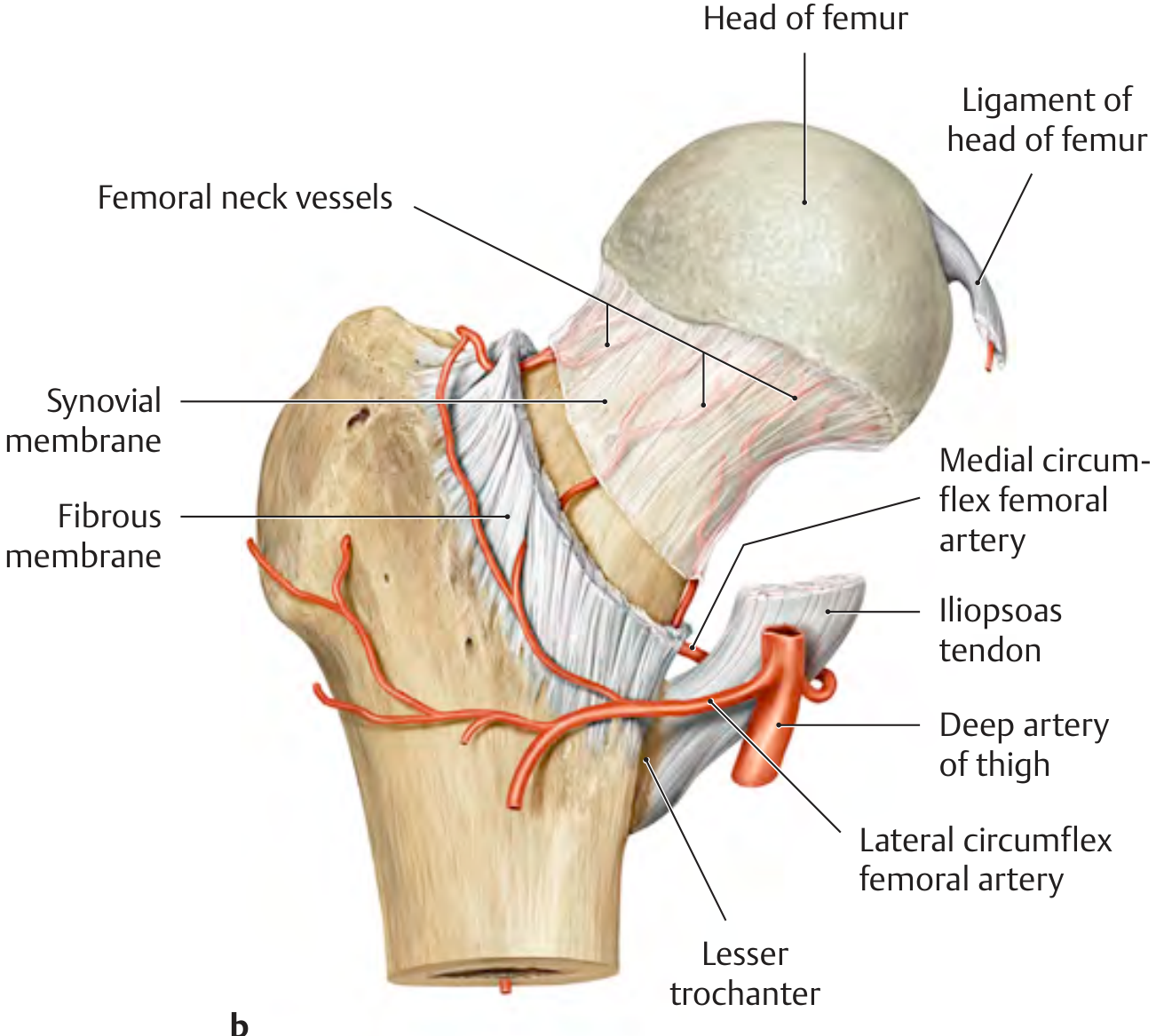
- Ascends along the femoral neck as retinacular vessels (posterosuperior and posteroinferior retinacular arteries) beneath the synovial reflection of the joint capsule
- Terminates as the lateral epiphyseal artery (also called the superior retinacular artery) - the single most important vessel to the femoral head in adults
- Supplies ~80% of the femoral head in adults
- Critical point: the MFCA deep branch passes just superior to the quadratus femoris muscle - this is why the quadratus femoris must NOT be completely transected during a posterior hip approach (Miller's Review, 9th Ed)
2. Lateral Femoral Circumflex Artery (LFCA)
- Also a branch of the profunda femoris
- Gives the inferior retinacular artery (anteroinferior retinacular vessels)
- Contributes minimally in adults - mainly supplies the anteroinferior head
- More important in neonates and infants
3. Artery of the Ligamentum Teres (Foveal Artery)
- Branch of the posterior division of the obturator artery (occasionally medial circumflex)
- Travels within the ligamentum teres to reach the fovea capitis on the femoral head
- Supplies only the area around the fovea (~10-15% of femoral head)
- Clinically insignificant in adults but important in children (up to 4 years)
- Can sustain the femoral head in hip dislocations if the retinacular vessels are disrupted
Age-Related Changes in Blood Supply (2 marks)
| Age | Primary Blood Supply |
|---|---|
| Birth to 4 years | MFCA + LFCA equally; Ligamentum teres (obturator artery) also significant |
| 4 years to adolescence | MFCA becomes dominant; LFCA contribution negligible; Ligamentum teres minimal |
| Adult | MFCA exclusively via lateral epiphyseal artery; ligamentum teres insignificant |
Anatomical Course and Retinacular Vessels (2 marks)
- After the MFCA gives its deep branch, it runs between the obturator externus below and the hip capsule above
- The vessels then travel along the femoral neck beneath the synovial reflection of the capsule (between capsule and bone)
- They are arranged in groups:
- Posterosuperior retinacular vessels (most important) - from MFCA deep branch
- Posteroinferior retinacular vessels - from MFCA
- Anterosuperior and anteroinferior - from LFCA (minor)
- These vessels enter the bone at the subcapital region (head-neck junction)
- The entire pathway is intracapsular but extrasynovial
- Posterior capsulotomy can damage retinacular vessels → risk of AVN
- The capsule attaches at the intertrochanteric line anteriorly but only mid-neck posteriorly → the posterior neck is extracapsular
Clinical Correlations (2 marks)
1. Femoral Neck Fracture - Why AVN Occurs
- A displaced intracapsular femoral neck fracture (Garden III/IV) tears the retinacular vessels against the capsule
- Haematoma under the capsule can also cause tamponade of retinacular flow
- Subcapital fractures have higher AVN rates (20-30%) than basicervical (extracapsular - very low AVN risk)
- This is why time to surgery matters in young patients with displaced fractures - urgent reduction and fixation may restore perfusion before irreversible ischaemia
2. Hip Dislocation
- Posterior dislocation tears the posterosuperior retinacular vessels
- AVN rate after traumatic hip dislocation = 10-25%, higher if reduction is delayed >6 hours
- Reduction within 6 hours is the most important determinant of AVN prevention
3. SCFE (Slipped Capital Femoral Epiphysis)
- The slip occurs through the zone of hypertrophy at the physis
- Retinacular vessels on the posterosuperior neck are at risk → AVN in ~10-15% of cases
- Risk higher with unstable (acute on chronic) SCFE
4. Surgical Approach Implications
- Posterior approach (Kocher-Langenbeck): must preserve at least 50% of quadratus femoris to protect MFCA deep branch
- Pediatric IMN: avoid piriformis starting point → use trochanteric entry point to protect posterosuperior retinacular vessels
- Hip resurfacing arthroplasty: posterior approach must meticulously preserve the MFCA
5. Legg-Calve-Perthes Disease
- Idiopathic interruption of MFCA in children 4-8 years → AVN of capital epiphysis
- Because ligamentum teres supply is already negligible at this age, there is no collateral rescue
Summary Table for Quick Recall
| Vessel | Source | Contribution | Significance |
|---|---|---|---|
| MFCA (deep branch → retinacular) | Profunda femoris | 80% (adults) | MOST IMPORTANT - damaged in neck fractures, hip dislocations |
| LFCA (retinacular) | Profunda femoris | 15% (adults) | Anteroinferior head; more in infants |
| Foveal artery | Obturator (posterior division) | 5% (adults) | Significant only in children <4 yrs |
Viva Questions & Model Answers
course of mcfa diagrams only
Course of the Medial Circumflex Femoral Artery (MFCA) - Diagrams
Diagram 1 - Overview: Origin from Profunda Femoris (Anterior View)
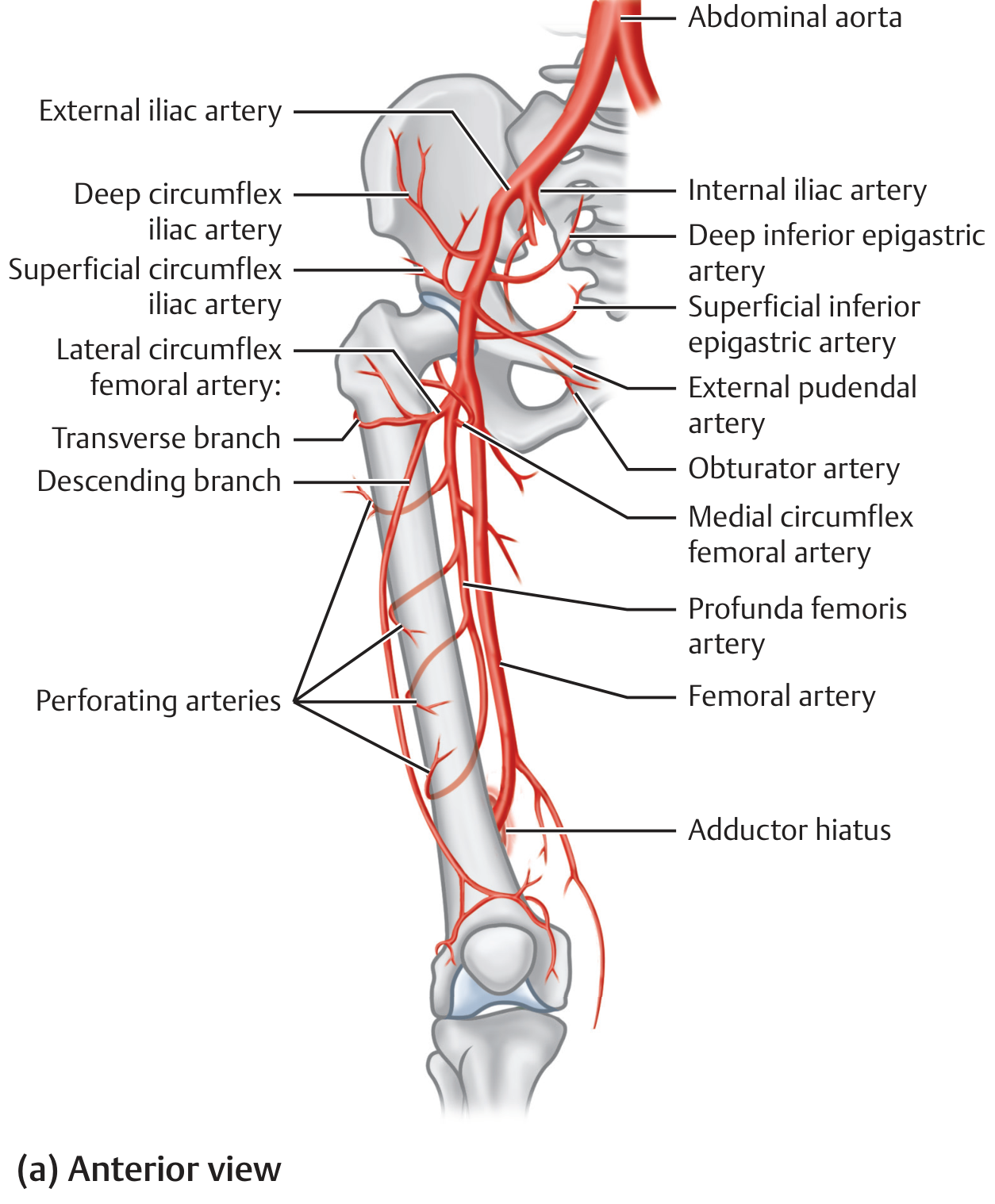
Diagram 2 - Anterior and Posterior Course with Cruciate Anastomosis
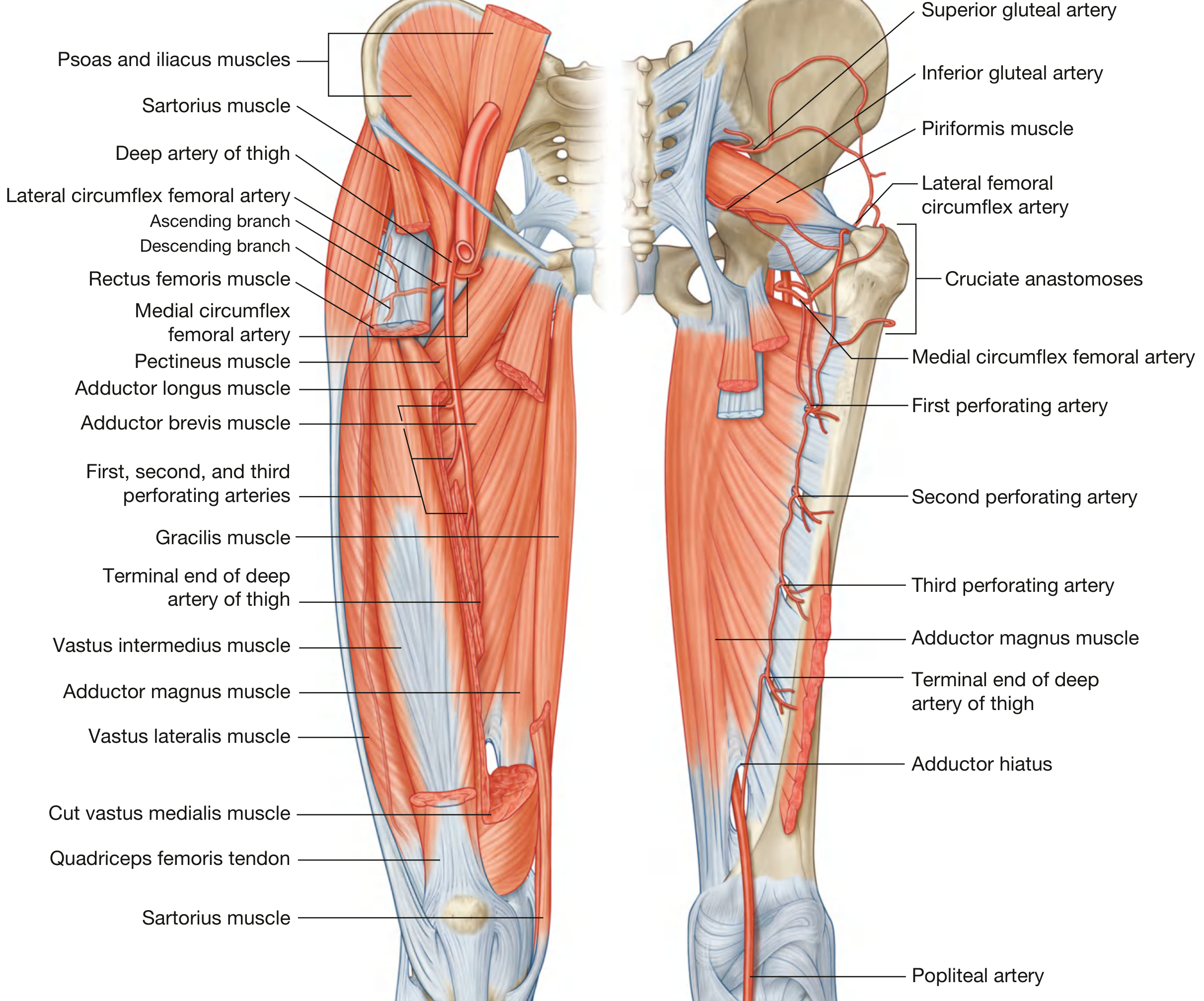
- Anterior view (left): MFCA passes medially between pectineus and iliopsoas, then between obturator externus and adductor brevis
- Posterior view (right): MFCA courses posteriorly to reach the trochanteric fossa, forming the cruciate anastomosis with LFCA transverse branch, inferior gluteal, and 1st perforating artery
Diagram 3 - Posterior View: MFCA giving Posterior Retinacular Arteries
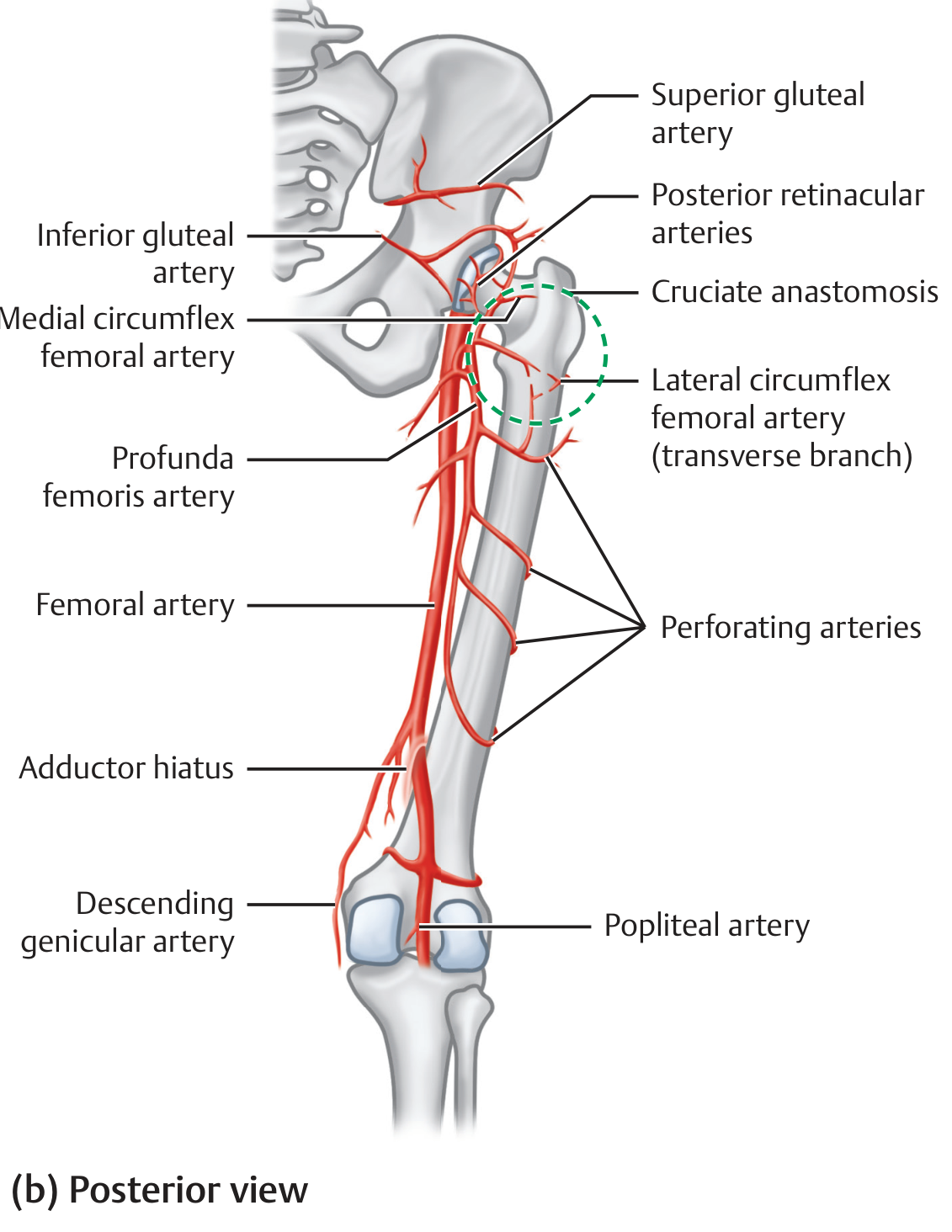
Diagram 4 - Deep Dissection: MFCA passing Superior to Quadratus Femoris
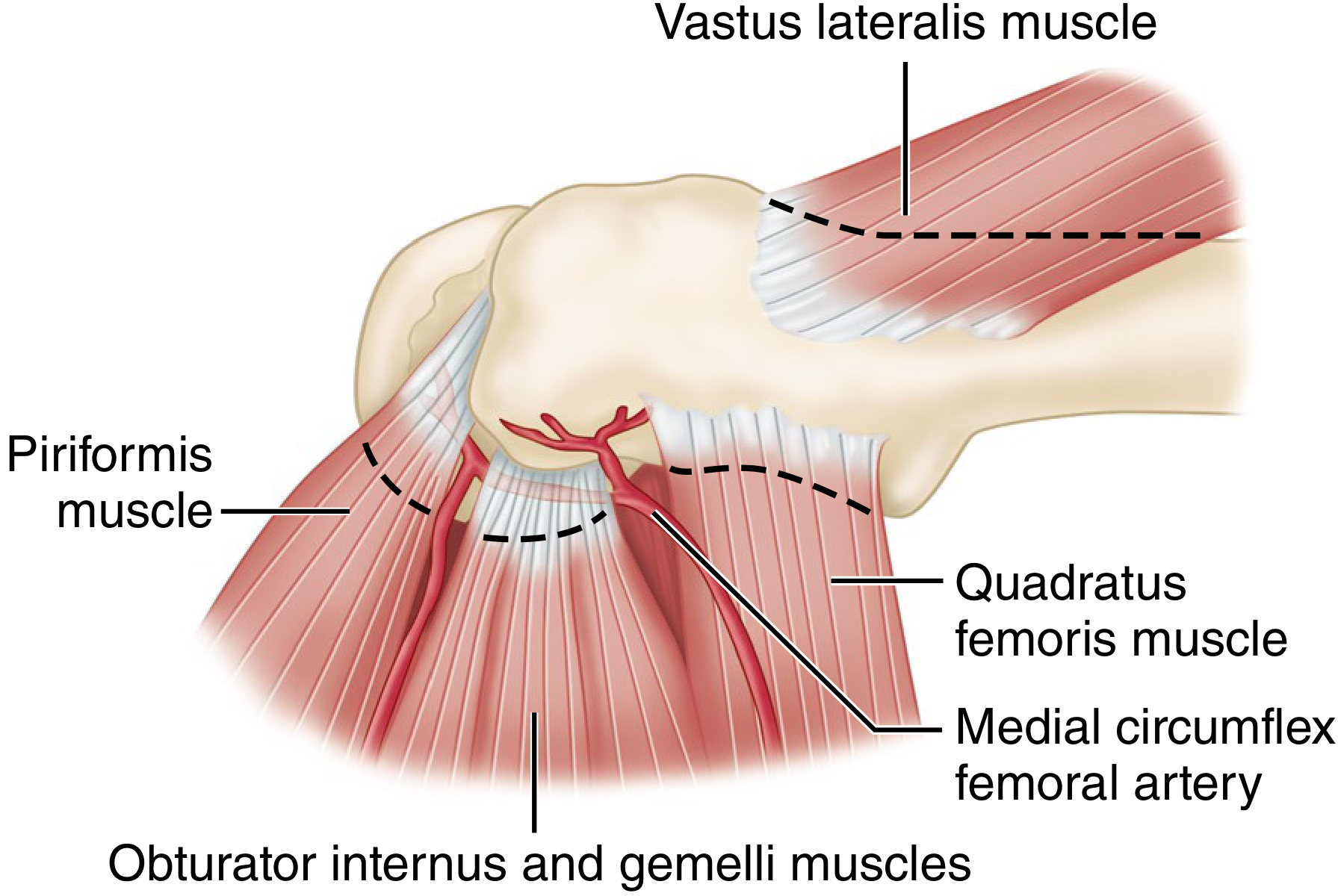
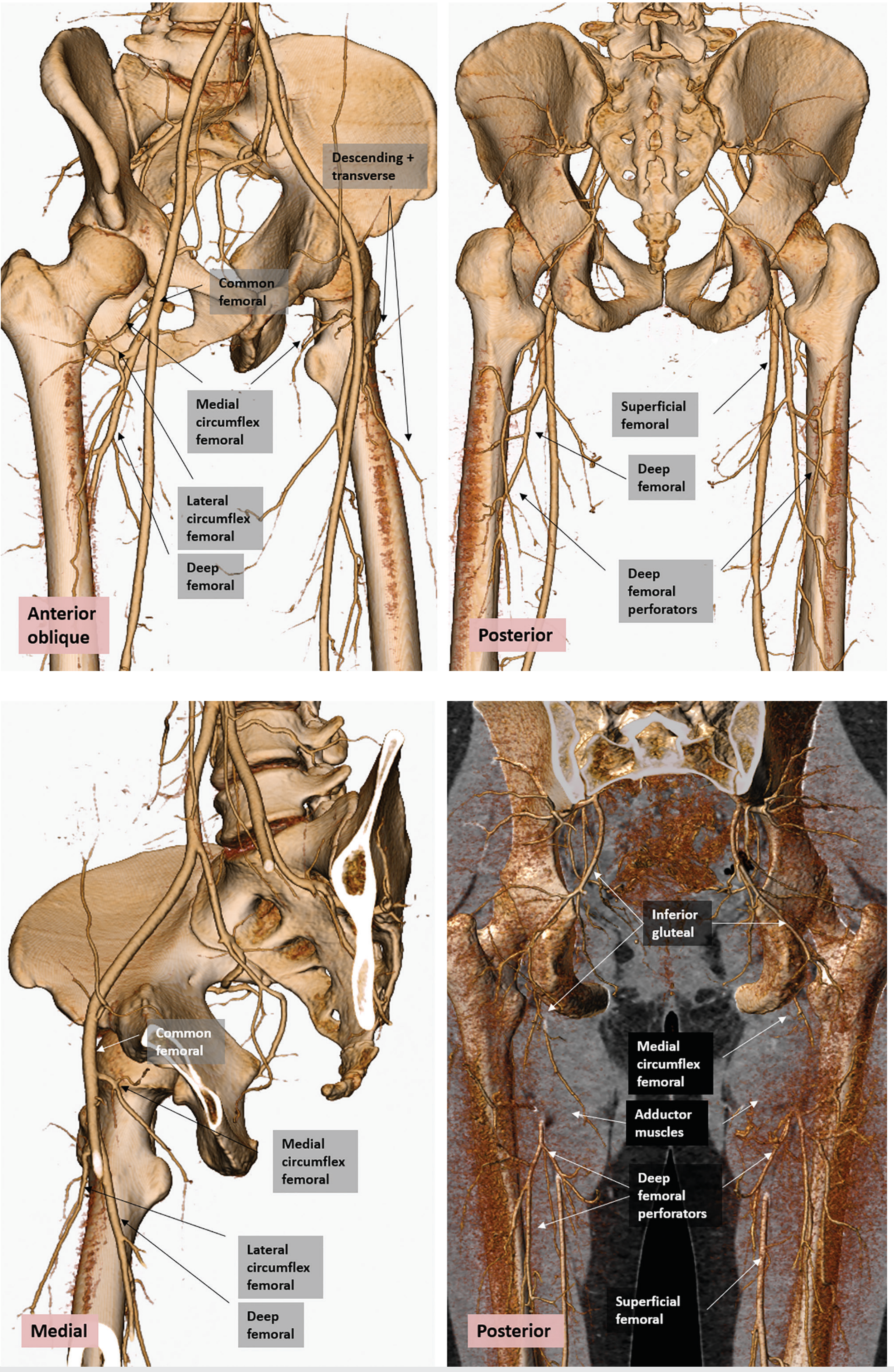
Diagram 5 - CT Angiogram: Real Anatomy, Multiple Views
Summary of MFCA Course in One Line
Origin (profunda femoris) → passes medially between pectineus + iliopsoas → between obturator externus + adductor brevis → crosses superior border of adductor magnus → passes deep to quadratus femoris → enters posterior capsule as retinacular vessels → ascends along femoral neck as posterosuperior retinacular artery → enters femoral head at subcapital region as lateral epiphyseal artery
recent advances
"avascular necrosis" AND "femoral head" AND treatment
"osteonecrosis" AND "femoral head" AND "stem cell" OR "core decompression" OR "bisphosphonate"
PMID: 37533122
PMID: 40554507
PMID: 39051378
PMID: 40490143
PMID: 37338665
Recent Advances in Femoral Head Blood Supply & AVN
Exam-Ready Answer (add as final paragraph to any AVN / FNF / Blood Supply essay)
1. New Understanding of MFCA Anatomy
- Duplex ultrasonography and MR angiography can now non-invasively map the MFCA course pre-operatively, allowing surgeons to plan hip approaches with vessel preservation
- 3D CT angiography (as seen in Imaging Anatomy Atlas Vol 3) has confirmed that MFCA anatomical variants exist in up to 20% of patients - the MFCA may arise directly from the femoral artery rather than the profunda femoris
- Zone-specific retinacular vessel mapping has shown that the posterosuperior retinacular vessels enter the head at a consistent "safe zone" between 10 and 2 o'clock - this forms the basis of the Safe Surgical Dislocation approach (Ganz osteotomy)
2. Post-COVID AVN - A New Etiology (Very Exam-Relevant)
- Post-COVID AVN is now a recognised entity, asked directly in April 2026 Paper IV
- Systematic review of 104 patients (Hassan & Khalifa, Rheumatol Int 2023 - [PMID 37338665]):
- Mean age 42.2 years - younger than typical AVN
- 13 of 14 reports: corticosteroid use during COVID management was the primary culprit (mean prednisolone equivalent 1238 mg total)
- 70.1% presented at Ficat Stage II at diagnosis
- Most hips (80.8%) managed non-surgically with good outcomes if caught early
- Mean interval from COVID diagnosis to AVN detection: 142 days - screening at 3-6 months post-COVID + steroid use is now recommended
- Other proposed mechanisms: COVID-19-related hypercoagulable state, direct vascular endothelial damage by SARS-CoV-2
3. Core Decompression - Still the Gold Standard for Early AVN, Now Enhanced
- Core decompression (Ficat I and II) remains first-line surgical treatment
- Enhanced by stem cell augmentation - the most important recent advance:
- Meta-analysis of 11 RCTs + 7 retrospective studies, 1257 hips (Li et al., J Orthop Surg Res 2023 - [PMID 37533122]):
- Lower femoral head collapse rate with CD + stem cells vs CD alone (P=0.001)
- Lower THA conversion rate overall (P<0.0001)
- Best results when stem cells are extracted (concentrated) + combined with mechanical support (structural graft)
- Meta-analysis of 11 RCTs + 7 retrospective studies, 1257 hips (Li et al., J Orthop Surg Res 2023 - [PMID 37533122]):
4. Bone Marrow Stem Cell (BMSC) Therapy - Level 1 Evidence Now Available
- Most comprehensive meta-analysis of RCTs only (Novriansyah et al., PLoS One 2025 - [PMID 40554507]):
- 10 RCTs, 593 patients, 779 hips
- BMSC therapy significantly reduced femoral head collapse (OR 0.15, P<0.00001)
- Reduced THA conversion rate (OR 0.20, P<0.00001)
- Harris Hip Score improved by 10.7 points (MD=10.70, P<0.00001)
- Pain (VAS) reduced by 8 points (P<0.00001)
- 70% of included RCTs had low risk of bias - this is now high-quality evidence
- Technique: Bone marrow aspirated from iliac crest → centrifuged → concentrated BMSC injected into core decompression channel
- Mechanism: BMSCs differentiate into osteoblasts, secrete angiogenic growth factors (VEGF, bFGF), stimulate neovascularisation
5. Conservative / Pharmacological Advances
| Agent | Mechanism | Status |
|---|---|---|
| Bisphosphonates (Alendronate, Zoledronate) | Inhibit osteoclast-mediated subchondral bone resorption, prevent collapse | Promising for early AVN (Ficat I-II); reduce collapse rate but do not regenerate bone |
| Statins (Pravastatin) | Anti-apoptotic, promote angiogenesis | Protective in steroid-induced AVN; reduce incidence when given with corticosteroids |
| Anticoagulants (Enoxaparin) | Prevent microvascular thrombosis | Used in thrombophilia-related AVN |
| ESWT (Extracorporeal Shockwave Therapy) | Stimulates neoangiogenesis, osteogenesis | Non-invasive; trials show pain reduction and retarded progression |
| Hyperbaric oxygen therapy | Increases oxygen supply to ischaemic bone | Limited evidence; used as adjunct |
| PRP (Platelet-Rich Plasma) | Growth factors stimulate healing | Emerging; combined with core decompression |
6. Vascularised Fibular Grafting - Updated Evidence
- Free vascularised fibular graft (FVFG) remains the preferred joint-preserving surgical option for pre-collapse AVN (Ficat II-III) in young patients
- Provides structural support AND vascular supply to the necrotic segment
- 10-year survivorship: ~70% in pre-collapse stages
- Recent modification: pedicled iliac crest graft (based on deep circumflex iliac artery) for smaller lesions
7. Surgical Trends - Global Perspective
- Corticosteroid use = #1 risk factor (75% of cases)
- THA is the dominant treatment (22.6% underwent THA within 1 year of diagnosis)
- Joint-preserving procedures declining in Western countries but increasing in younger patients
- Asian centres (South Korea, Japan) favour joint-preserving surgery more than Western centres - geographic variation is significant
- Call for consensus-driven international guidelines given this variation
8. Femoral Neck System (FNS) - New Implant to Protect Blood Supply
- FNS (Femoral Neck System) - asked directly as a short note in April 2026 Paper IV
- Single implant combining a sliding lag screw with an anti-rotation screw, inserted via a minimally invasive approach
- Advantage over sliding hip screw: smaller incision = less soft tissue disruption = less risk to retinacular vessels
- Advantage over 3 cannulated screws: better rotational control
- Indicated for: Garden I-II and selected Garden III-IV fractures in younger patients
- Early results: comparable to dynamic hip screw with potentially lower AVN rates (ongoing trials)
Viva Quick-Fire on Recent Advances
fns and ficet staging garden staging
Garden Classification + Ficat Staging + FNS
Complete Exam Answer - Short Note / Viva Ready
1. GARDEN CLASSIFICATION of Femoral Neck Fractures (1961)
| Grade | Description | Trabecular Pattern | Displacement | AVN Risk |
|---|---|---|---|---|
| I | Valgus-impacted, incomplete subcapital fracture, intact medial calcar | Femoral head trabeculae form an angle with acetabular trabeculae (valgus tilt) | None - impacted | 0-10% |
| II | Complete fracture, undisplaced | Trabecular lines in head are collinear with acetabulum and distal neck | None | 10-20% |
| III | Incomplete displacement, angulation present | Trabecular lines angulated - not collinear | Partial | 20-35% |
| IV | Complete displacement | Femoral head rotates freely - trabecular lines in head become parallel to acetabular lines again (head realigns with acetabulum, neck has migrated) | Complete | 30-50% |
Key Points for Viva
- Garden I + II = Undisplaced → treat with internal fixation (3 cannulated screws or FNS)
- Garden III + IV = Displaced → in elderly: hemiarthroplasty or THA; in young (<60 yrs): urgent reduction + internal fixation
- Practical use: Interobserver agreement is poor across all 4 grades (only 22%) - but agreement is good when simplified to undisplaced (I+II) vs displaced (III+IV)
- Garden II is rare in practice - only 1.2% of femoral neck fractures in a large multicenter study of 1503 cases (Rockwood & Green 10th Ed)
- Garden Alignment Index (post-reduction check): AP 160°, lateral 180° - acceptable range AP 155-180°, lateral 155-180°
- In Garden IV, the head is completely free and rotates back to align with the acetabulum - the trabeculae look parallel/normal again on X-ray. The neck has displaced but the head has swung back. This paradox distinguishes it from Garden I (which is impacted in valgus).
2. FICAT CLASSIFICATION (Ficat & Arlet) of AVN of Femoral Head
| Stage | Symptoms | X-Ray | Bone Scan | MRI | Pathology | Treatment |
|---|---|---|---|---|---|---|
| 0 | None | Normal | Decreased uptake (cold spot) | Abnormal | Infarction beginning | Observation / treat cause |
| 1 | None / mild | Normal | Cold spot on femoral head | Oedema (earliest MRI sign) | Dead marrow, osteoblasts | Bisphosphonates, core decompression |
| 2 | Mild | Sclerosis and/or cysts, normal joint line, normal head contour | Increased uptake | Necrotic area visible | Spontaneous repair, new bone on dead trabeculae | Core decompression ± stem cells, vascularised fibular graft |
| 3 | Mild-moderate | Crescent sign (subchondral fracture), flattening begins, joint space preserved | Increased uptake | Collapse visible | Subchondral fracture, compaction, fragmentation | Vascularised fibular graft, osteotomy (in young), THA in older |
| 4 | Moderate-severe | Joint space narrowing, acetabular changes, osteoarthritic changes | Increased uptake | Full collapse + OA changes | Degenerative changes in acetabular cartilage too | THA |
Additional Classifications (Also Know These for Viva)
Memory Aid for Ficat:
"Normal → Sclerosis → Crescent → Collapse"
- Stage 1: Normal X-ray, abnormal MRI
- Stage 2: Sclerosis/cysts, still round head
- Stage 3: Crescent sign (the hallmark)
- Stage 4: Collapse + OA
3. FEMORAL NECK SYSTEM (FNS) - Recent Advance


What is FNS?
- A large-diameter sliding lag screw for compression along the femoral neck
- A small-diameter anti-rotation screw placed parallel to it (prevents rotational displacement)
- A short side plate with only 2 cortical screws in the shaft
How it Differs from Existing Implants
| Feature | Cannulated Screws (3) | Dynamic Hip Screw (DHS) | FNS |
|---|---|---|---|
| Anti-rotation | Weak (3 independent screws) | Poor | Built-in anti-rotation screw |
| Controlled sliding compression | No | Yes (single plane) | Yes (single plane) |
| Neck shortening | High (42-66%) | Moderate | Lower |
| Incision | Minimal | Larger | Minimal (MIS) |
| Soft tissue damage | Least | More | Minimal |
| MFCA protection | Moderate risk | Less risk | Best - minimal dissection |
| Stability | Weakest | Good | Similar to DHS, superior to 3 screws |
Evidence for FNS (from Campbell's 15th Ed)
- Biomechanical stability equal to DHS, superior to multiple cannulated screws
- Decreased rates of AVN compared to cannulated screws (less soft tissue damage = better retinacular vessel preservation)
- Decreased femoral neck shortening
- Less fluoroscopy use, better functional outcomes
- Systematic review and meta-analysis (Patel et al., Eur J Orthop Surg 2023): FNS leads to better outcomes than cannulated screws in adults
Indications for FNS
- Garden I and II (undisplaced) femoral neck fractures in any age
- Garden III-IV (displaced) in young patients (<60 years)
- High Pauwels angle fractures (Type III - most unstable, vertical fracture line) - where rotational control is most needed
Why FNS Protects Blood Supply Better
- Inserted via a small lateral incision over the trochanteric region
- No posterior dissection → retinacular vessels on the posterior neck are undisturbed
- No capsulotomy required
- Compare to: posterior approach for open reduction which risks the MFCA deep branch
Viva Quick-Fire
BED SORE CLASSIFICATION AND MANAGEMENT IN PARAPLEGIA PATIENT 5+5