

Messenger_creation_D2B7FC08-49E7-4C1A-AE20-F71271FF4241.jpeg
IMG_20260512_212018.jpg
A patient 45 years old he have no heart kidney or liver problem but you are so much in sunlight so this is her skin and what is the problem in her skin heart is your diagnosis and heart is your treatment
Reading File
Finding Sources
Finding Sources
Searching the Web
chronic sun exposure skin hyperpigmentation dark macules lichenification dry scaling forearm elbow diagnosis treatment
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive information. Here is the full clinical assessment:
⚠️ Important Disclaimer
This is educational information only. A physical examination and dermatologist consultation are required for a definitive diagnosis.
Clinical Findings from the Images
| Feature | Observation |
|---|---|
| Location | Sun-exposed areas — dorsum of hand/wrist and elbow |
| Skin texture | Thickened, rough, leathery (lichenification) |
| Pigmentation | Hyperpigmentation (darkening) of the skin |
| Lesions | Scattered small dark macules/papules (Image 1) |
| Surface | Dry, scaling, white flaky patches (Image 2) |
| Skin folds | Appear relatively spared |
Diagnosis: Chronic Actinic Dermatitis (CAD)
Also previously called: persistent light reactivity, actinic reticuloid, photosensitive eczema.
This is the most likely diagnosis given:
- 45-year-old male with extensive sun exposure
- Eczematous, lichenified, hyperpigmented plaques on sun-exposed areas (hands, forearms, elbows)
- Scaling and dryness consistent with chronic photosensitivity reaction
- Sparing of skin folds (a hallmark of CAD)
- No systemic disease (rules out metabolic or drug causes)
From Fitzpatrick's Dermatology (Fig. 97-5): "Chronic actinic dermatitis — note the lichenification and hyperpigmentation on sun-exposed areas, and sparing of skin folds." — exactly matching the patient's photos.
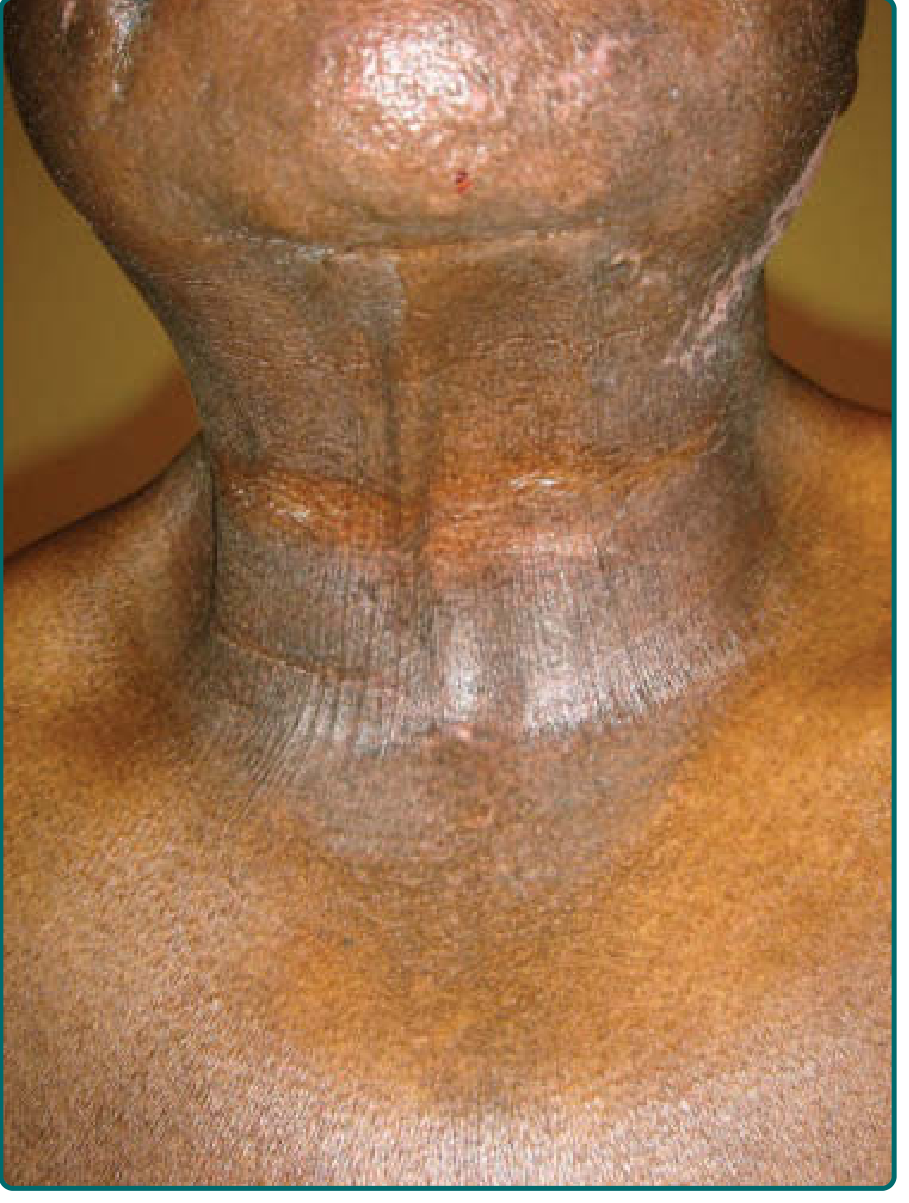
CAD predominantly affects middle-aged or elderly men, particularly those with darker skin types (Fitzpatrick types V–VI), who are disproportionately affected. The skin lesions consist of edematous, scaling, thickened patches and plaques occurring primarily on sun-exposed skin.
Treatment Plan
(Source: Andrews' Diseases of the Skin, Clinical Dermatology)
Step 1 — Sun Protection (Essential)
- Maximum sun avoidance — wear long sleeves, hat, and gloves outdoors
- Broad-spectrum sunscreen (SPF 50+, UVA + UVB protection) — apply daily, even on cloudy days
- Avoid peak sun hours (10 AM – 4 PM)
- Identify and avoid any topical photosensitizers via photopatch testing
Step 2 — Topical Treatment (First-Line)
| Drug | Use |
|---|---|
| Topical tacrolimus 0.1% ointment | Effective in many patients; first-line non-steroid option |
| Topical corticosteroids (moderate-to-potent) | Reduce inflammation; short-term use |
| Emollients / moisturizers | For dryness and scaling — apply twice daily |
Step 3 — Systemic Treatment (If Refractory)
- Azathioprine 50–200 mg/day — most reproducibly effective; may be needed during high-sun seasons
- Cyclosporine — for severe/refractory cases
- Mycophenolate mofetil — alternative immunosuppressant
- Systemic corticosteroids — short courses only (chronic use limited by toxicity)
- Hydroxyurea 500 mg twice daily — adjunctive option
Step 4 — Phototherapy (Specialist-Supervised)
- Narrowband UVB (NB-UVB) or low-dose PUVA — paradoxically used to desensitize the skin; requires specialist supervision
- Extended duration of treatment is often needed
Prognosis
With careful management, approximately 1 in 3 patients lose photosensitivity within 15 years, and most improve over time. Only 1 in 20 worsen.
Referral Recommended
This patient should see a dermatologist for:
- Formal phototesting (to confirm UVA/UVB sensitivity range)
- Photopatch testing (to rule out contact photosensitizers)
- Possible skin biopsy to confirm diagnosis and exclude lymphoma (mycosis fungoides can mimic CAD)
This is a shared conversation. Sign in to Orris to start your own chat.