Which BP medicine given in which condition
Antihypertensive Drugs: Which Drug for Which Condition
Drug Treatment Algorithm for Uncomplicated Hypertension
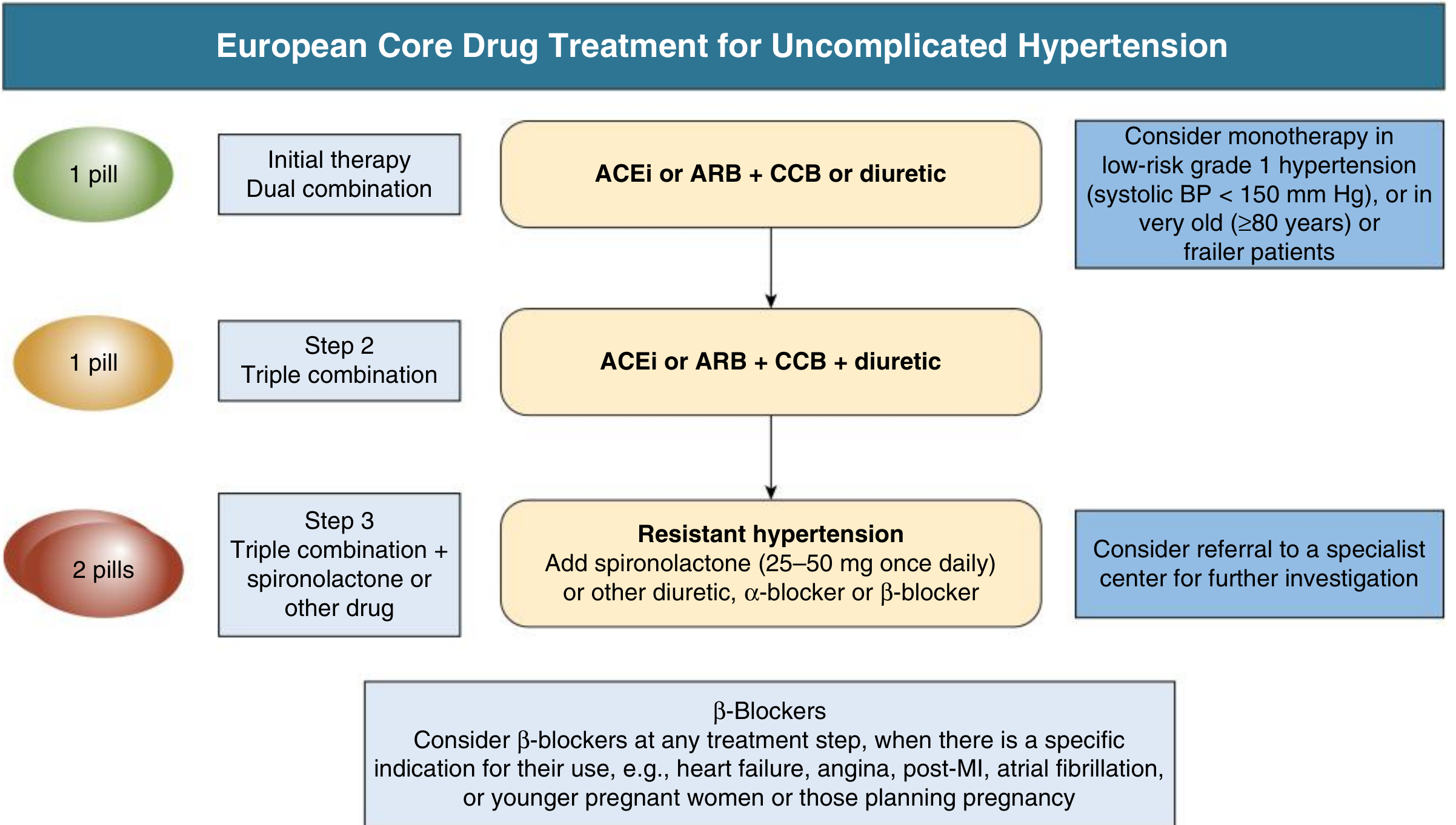
Beta-blockers are added at any step when there is a specific indication: heart failure, angina, post-MI, atrial fibrillation, or younger pregnant women.
Compelling Indications Table (JNC 7 / ACC-AHA)
| Condition | Diuretic | Beta-Blocker | ACE Inhibitor | ARB | CCB | MRA (Spironolactone) |
|---|---|---|---|---|---|---|
| Heart Failure | ✓ | ✓ | ✓ | ✓ | - | ✓ |
| Post-MI | - | ✓ | ✓ | - | - | ✓ |
| High CAD Risk | ✓ | ✓ | ✓ | - | ✓ | - |
| Diabetes Mellitus | ✓ | ✓ | ✓ | ✓ | ✓ | - |
| Renal Disease (CKD) | - | - | ✓ | ✓ | - | - |
| Recurrent Stroke Prevention | ✓ | - | ✓ | - | - | - |
Detailed Drug-by-Drug Breakdown
1. Thiazide/Thiazide-like Diuretics (e.g., Hydrochlorothiazide, Chlorthalidone)
- Indications: Uncomplicated HTN (first-line), heart failure, high CAD risk, diabetes, stroke prevention
- Mechanism: Inhibit Na-Cl cotransporter in distal convoluted tubule
- Side effects: Hypokalemia, hyponatremia, hyperuricemia, impaired glucose tolerance, dyslipidemia
- Note: Chlorthalidone preferred over HCTZ (longer duration, better CV outcomes)
2. Loop Diuretics (e.g., Furosemide)
- Indications: HTN with volume overload, heart failure with fluid retention, CKD with low GFR (<30)
- Mechanism: Inhibit Na-K-2Cl cotransporter in thick ascending limb
- Side effects: Hypokalemia, ototoxicity, fewer metabolic effects than thiazides
3. ACE Inhibitors (e.g., Ramipril, Lisinopril, Enalapril)
- Indications: Heart failure, post-MI, CKD (especially with proteinuria), diabetes, high CAD risk, stroke prevention
- Mechanism: Block conversion of angiotensin I to angiotensin II
- Side effects: Dry cough (10-15%), hyperkalemia, elevated creatinine, angioedema, teratogenic (avoid in pregnancy)
4. Angiotensin Receptor Blockers/ARBs (e.g., Losartan, Valsartan, Telmisartan)
- Indications: Same as ACEi - heart failure, CKD, diabetes; preferred when patient cannot tolerate ACEi (due to cough)
- Mechanism: Block angiotensin II at the AT1 receptor
- Side effects: Similar to ACEi but NO cough; also teratogenic (avoid in pregnancy)
5. Calcium Channel Blockers/CCBs
| Subclass | Examples | Indications | Notes |
|---|---|---|---|
| Dihydropyridine | Amlodipine, Nifedipine | HTN + angina, elderly, diabetes, high CAD risk | Peripheral vasodilation; edema as side effect |
| Non-DHP (Diltiazem) | Diltiazem | HTN + angina + atrial fibrillation | AV node blockade; bradycardia |
| Non-DHP (Verapamil) | Verapamil | HTN + SVT, angina | AV node blockade; constipation; avoid in HFrEF |
6. Beta-Blockers (e.g., Metoprolol, Carvedilol, Atenolol, Labetalol)
- Indications: HTN + heart failure (HFrEF), post-MI, angina, atrial fibrillation (rate control), hypertensive urgency in pregnancy (labetalol)
- Side effects: Reduced exercise tolerance, depression, bronchospasm (non-selective BB), impaired glucose masking
- Contraindication: Asthma/COPD (use cardioselective if essential), severe bradycardia, decompensated HF acutely
7. MRA - Mineralocorticoid Receptor Antagonists (e.g., Spironolactone, Eplerenone)
- Indications: Resistant hypertension (4th-line add-on), heart failure (HFrEF), post-MI with HF, primary hyperaldosteronism
- Side effects: Hyperkalemia, gynecomastia (spironolactone), menstrual irregularities
8. Alpha-Blockers (e.g., Doxazosin, Prazosin)
- Indications: HTN + benign prostatic hyperplasia (BPH), pheochromocytoma (phentolamine)
- Note: Not first-line for HTN alone due to increased CV events in ALLHAT trial
9. Central Alpha-2 Agonists (e.g., Methyldopa, Clonidine)
- Indications: Hypertension in pregnancy (methyldopa is drug of choice), resistant HTN
- Side effects: Sedation, dry mouth, rebound HTN on abrupt withdrawal (clonidine)
Special Situations - Drug of Choice
| Clinical Situation | Preferred Drug(s) |
|---|---|
| Pregnancy | Methyldopa, Labetalol, Nifedipine (extended-release) |
| Hypertensive emergency | IV Labetalol, IV Nicardipine, IV Nitroprusside, IV Clevidipine, Fenoldopam |
| Hypertensive emergency + aortic dissection | IV Esmolol + IV Nitroprusside (reduce HR and BP simultaneously) |
| Hypertension + pheochromocytoma | Phentolamine (alpha-blocker) FIRST, then beta-blocker |
| Hypertension + BPH | Doxazosin (alpha-blocker) |
| Isolated systolic hypertension in elderly | Dihydropyridine CCB (amlodipine) or thiazide diuretic |
| Hypertension + metabolic syndrome | ACEi or ARB (avoid thiazide + beta-blocker combination - worsens glucose control) |
| Black/African patients | CCB or thiazide diuretics (RAS blockers less effective as monotherapy) |
| CKD + proteinuria | ACEi or ARB (renoprotective) |
| Post-MI | Beta-blocker + ACEi + MRA |
| Atrial fibrillation | Beta-blocker or non-DHP CCB (rate control) |
Hypertensive Emergency - Drug Guide
| Emergency Type | First-Line IV Agents | Avoid |
|---|---|---|
| Hypertensive encephalopathy | Nicardipine, Labetalol, Clevidipine | Nitroprusside |
| Acute ischemic stroke | Nicardipine, Labetalol, Clevidipine | Nitroprusside, Nimodipine (usually) |
| Aortic dissection | Esmolol + Nitroprusside | Hydralazine (reflex tachycardia) |
| Acute pulmonary edema | IV Nitroglycerine, Furosemide, Nicardipine | Beta-blockers |
| Acute MI | Beta-blocker, Nitroglycerine, ACEi | Hydralazine |
| Eclampsia | IV Hydralazine, IV Labetalol, IV MgSO4 (seizure prophylaxis) | ACEi, ARBs |
Drugs to Avoid in Specific Conditions
| Condition | Avoid |
|---|---|
| Bilateral renal artery stenosis | ACEi, ARBs |
| Pregnancy | ACEi, ARBs, Direct renin inhibitors |
| Asthma/COPD | Non-selective beta-blockers |
| AV block (2nd/3rd degree) | Verapamil, Diltiazem, Beta-blockers |
| Hyperkalemia | ACEi, ARBs, Potassium-sparing diuretics, MRA |
| Gout | Thiazide diuretics (worsen hyperuricemia) |
| Decompensated heart failure (acute) | Verapamil, Non-DHP CCBs |
Create a quick-reference PDF chart of BP medications I can print
ls /home/daytona/workspace/ 2>/dev/null || echo "workspace empty or not found"
mkdir -p /home/daytona/workspace/bp-chart && python3 -c "import reportlab; print('reportlab ok')" && python3 -c "from reportlab.lib import colors; print('colors ok')"
~/bp-chart/generate_bp_chart.py
from reportlab.lib.pagesizes import A4, landscape
from reportlab.lib import colors
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.units import mm, cm
from reportlab.platypus import (
SimpleDocTemplate, Table, TableStyle, Paragraph,
Spacer, HRFlowable, KeepTogether
)
from reportlab.lib.enums import TA_CENTER, TA_LEFT
from reportlab.platypus import PageBreak
OUTPUT = "/home/daytona/workspace/bp-chart/BP_Medications_QuickRef.pdf"
# ── Colour palette ──────────────────────────────────────────────────────────
NAVY = colors.HexColor("#1a3a5c")
TEAL = colors.HexColor("#1a7a8a")
AMBER = colors.HexColor("#d4830a")
RED = colors.HexColor("#c0392b")
GREEN = colors.HexColor("#1e7d44")
LTBLUE = colors.HexColor("#dceef5")
LTTEAL = colors.HexColor("#d4f0f0")
LTAMBER = colors.HexColor("#fdf3dc")
LTRED = colors.HexColor("#fde8e6")
LTGREEN = colors.HexColor("#e6f5ec")
GREY1 = colors.HexColor("#f2f4f6")
GREY2 = colors.HexColor("#dce0e5")
WHITE = colors.white
BLACK = colors.black
# ── Styles ──────────────────────────────────────────────────────────────────
styles = getSampleStyleSheet()
title_style = ParagraphStyle(
"Title", fontSize=20, textColor=WHITE, fontName="Helvetica-Bold",
alignment=TA_CENTER, spaceAfter=2
)
subtitle_style = ParagraphStyle(
"Subtitle", fontSize=9, textColor=colors.HexColor("#cce0ee"),
fontName="Helvetica", alignment=TA_CENTER, spaceAfter=0
)
section_style = ParagraphStyle(
"Section", fontSize=11, textColor=WHITE, fontName="Helvetica-Bold",
alignment=TA_CENTER
)
cell_body = ParagraphStyle(
"CellBody", fontSize=7.5, fontName="Helvetica", leading=10,
alignment=TA_LEFT
)
cell_bold = ParagraphStyle(
"CellBold", fontSize=7.5, fontName="Helvetica-Bold", leading=10,
alignment=TA_LEFT
)
cell_center = ParagraphStyle(
"CellCenter", fontSize=7.5, fontName="Helvetica", leading=10,
alignment=TA_CENTER
)
cell_center_bold = ParagraphStyle(
"CellCenterBold", fontSize=8, fontName="Helvetica-Bold", leading=11,
alignment=TA_CENTER
)
small_note = ParagraphStyle(
"SmallNote", fontSize=6.5, fontName="Helvetica-Oblique", leading=9,
textColor=colors.HexColor("#555555"), alignment=TA_CENTER
)
# ── Helper ───────────────────────────────────────────────────────────────────
def p(text, style=cell_body):
return Paragraph(text, style)
def tick(yes=True):
return p("✔" if yes else "—", cell_center)
# ─────────────────────────────────────────────────────────────────────────────
# PAGE 1 – Compelling Indications + Drug Classes
# ─────────────────────────────────────────────────────────────────────────────
def build_page1():
elems = []
# ── Header banner ─────────────────────────────────────────────────────
header_data = [[
p("BP MEDICATIONS | QUICK REFERENCE CHART", title_style)
]]
header_tbl = Table(header_data, colWidths=[267*mm])
header_tbl.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), NAVY),
("TOPPADDING", (0,0), (-1,-1), 10),
("BOTTOMPADDING",(0,0),(-1,-1), 6),
("LEFTPADDING", (0,0), (-1,-1), 6),
("RIGHTPADDING",(0,0), (-1,-1), 6),
("ROUNDEDCORNERS",(0,0),(-1,-1), 6),
]))
elems.append(header_tbl)
elems.append(Spacer(1, 4*mm))
# ── SECTION 1: Compelling Indications ─────────────────────────────────
sec1_hdr = Table([[p("COMPELLING INDICATIONS (JNC 7 / ACC-AHA 2018)", section_style)]],
colWidths=[267*mm])
sec1_hdr.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), TEAL),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING",(0,0),(-1,-1), 5),
("ROUNDEDCORNERS",(0,0),(-1,-1), 4),
]))
elems.append(sec1_hdr)
elems.append(Spacer(1, 2*mm))
col_w = [44, 30, 30, 36, 30, 30, 30, 37] # mm
col_w_pts = [x*mm for x in col_w]
ci_header = [
p("Condition", cell_center_bold),
p("Diuretic\n(Thiazide)", cell_center_bold),
p("Beta-\nBlocker", cell_center_bold),
p("ACE\nInhibitor", cell_center_bold),
p("ARB", cell_center_bold),
p("CCB", cell_center_bold),
p("MRA\n(Spiro)", cell_center_bold),
p("Notes", cell_center_bold),
]
ci_data = [
ci_header,
[p("Heart Failure (HFrEF)", cell_bold), tick(), tick(), tick(), tick(), tick(False),
tick(), p("Avoid verapamil/diltiazem", cell_body)],
[p("Post-MI", cell_bold), tick(False), tick(), tick(), tick(False), tick(False),
tick(), p("Beta-blocker within 24h", cell_body)],
[p("High CAD Risk / Angina", cell_bold), tick(), tick(), tick(), tick(False), tick(),
tick(False), p("CCB: prefer amlodipine", cell_body)],
[p("Diabetes Mellitus", cell_bold), tick(), tick(), tick(), tick(), tick(),
tick(False), p("ACEi/ARB renoprotective", cell_body)],
[p("CKD / Proteinuria", cell_bold), tick(False), tick(False), tick(), tick(),
tick(False), tick(False), p("ACEi or ARB first-line", cell_body)],
[p("Stroke Prevention\n(Recurrent)", cell_bold), tick(), tick(False), tick(),
tick(False), tick(False), tick(False), p("Thiazide + ACEi combo", cell_body)],
[p("Atrial Fibrillation\n(Rate control)", cell_bold), tick(False), tick(), tick(False),
tick(False), p("✔ non-DHP\n(diltiazem)", cell_center), tick(False),
p("Avoid DHP CCBs alone", cell_body)],
[p("Pregnancy", cell_bold), tick(False), p("✔ Labetalol\nonly", cell_center),
tick(False), tick(False), p("✔ Nifedipine\n(long-acting)", cell_center),
tick(False), p("Methyldopa also safe", cell_body)],
[p("BPH", cell_bold), tick(False), tick(False), tick(False), tick(False), tick(False),
tick(False), p("Alpha-blocker (doxazosin)", cell_body)],
[p("Phaeochromocytoma", cell_bold), tick(False), p("✔ After\nalpha-block", cell_center),
tick(False), tick(False), tick(False), tick(False),
p("Alpha-blocker (phentolamine) FIRST", cell_body)],
]
ci_tbl = Table(ci_data, colWidths=col_w_pts, repeatRows=1)
ci_style = [
# Header row
("BACKGROUND", (0,0), (-1,0), NAVY),
("TEXTCOLOR", (0,0), (-1,0), WHITE),
("FONTNAME", (0,0), (-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,0), 8),
("ALIGN", (0,0), (-1,0), "CENTER"),
("VALIGN", (0,0), (-1,-1),"MIDDLE"),
("TOPPADDING", (0,0), (-1,-1), 4),
("BOTTOMPADDING",(0,0), (-1,-1), 4),
("LEFTPADDING", (0,0), (-1,-1), 4),
("RIGHTPADDING", (0,0), (-1,-1), 4),
("GRID", (0,0), (-1,-1), 0.4, GREY2),
("ROWBACKGROUNDS",(0,1),(-1,-1),[WHITE, GREY1]),
# Condition column highlight
("BACKGROUND", (0,1), (0,-1), LTBLUE),
("FONTNAME", (0,1), (0,-1), "Helvetica-Bold"),
]
ci_tbl.setStyle(TableStyle(ci_style))
elems.append(ci_tbl)
elems.append(Spacer(1, 4*mm))
# ── SECTION 2: Drug Class Summary ─────────────────────────────────────
sec2_hdr = Table([[p("DRUG CLASS SUMMARY – Mechanisms, Side Effects & Key Indications", section_style)]],
colWidths=[267*mm])
sec2_hdr.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), colors.HexColor("#1e5e3e")),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING",(0,0),(-1,-1), 5),
("ROUNDEDCORNERS",(0,0),(-1,-1), 4),
]))
elems.append(sec2_hdr)
elems.append(Spacer(1, 2*mm))
dc_col_w = [45, 38, 55, 55, 74] # mm
dc_col_w_pts = [x*mm for x in dc_col_w]
dc_header = [
p("Drug Class", cell_center_bold),
p("Examples", cell_center_bold),
p("Mechanism", cell_center_bold),
p("Side Effects", cell_center_bold),
p("Key Indications / Notes", cell_center_bold),
]
dc_rows = [
["Thiazide/Thiazide-like\nDiuretics",
"HCTZ, Chlorthalidone\nIndapamide",
"Inhibit Na-Cl cotransporter\n(distal convoluted tubule)",
"Hypokalemia, hyponatremia,\nhyperuricemia, hyperglycemia,\ndyslipidemia",
"First-line uncomplicated HTN;\nheart failure; CAD risk;\nstroke prevention.\nChlorothalidone preferred over HCTZ"],
["Loop Diuretics",
"Furosemide\nBumetanide",
"Inhibit Na-K-2Cl cotransporter\n(thick ascending limb)",
"Hypokalemia, ototoxicity,\ndehydration",
"HTN + volume overload;\nheart failure;\nCKD with GFR <30 (thiazides lose efficacy)"],
["ACE Inhibitors",
"Ramipril, Lisinopril\nEnalapril, Perindopril",
"Block Ang I → Ang II conversion\n(bradykinin accumulation)",
"Dry cough (10-15%),\nhyperkalemia, ↑creatinine,\nangioedema (rare)",
"Heart failure, post-MI, CKD with\nproteinuria, diabetes, stroke.\nAVOID: pregnancy, bilateral RAS"],
["Angiotensin Receptor\nBlockers (ARBs)",
"Losartan, Valsartan\nTelmisartan, Irbesartan",
"Block Ang II at AT1 receptor\n(no bradykinin accumulation)",
"Similar to ACEi;\nNO cough; rare angioedema",
"Same as ACEi — preferred when\nACEi cough intolerable.\nAVOID: pregnancy, bilateral RAS"],
["Dihydropyridine\nCCBs (DHP)",
"Amlodipine\nNifedipine (SR)\nFelodipine",
"Block L-type Ca²⁺ channels\n→ vasodilation",
"Peripheral edema, flushing,\ngingival hyperplasia",
"Uncomplicated HTN, elderly,\nisolated systolic HTN, angina,\nCKD, black patients, diabetes"],
["Non-DHP CCBs",
"Diltiazem\nVerapamil",
"Block L-type Ca²⁺ channels\n+ AV nodal depression",
"Bradycardia, AV block;\nverapamil: constipation",
"HTN + angina + AF (rate control).\nAVOID: HFrEF, AV block,\nwith beta-blockers"],
["Beta-Blockers",
"Metoprolol, Atenolol\nCarvedilol, Bisoprolol\nLabetalol (IV/oral)",
"Block β1 (and β2 if non-selective)\nadrenergic receptors",
"Fatigue, bradycardia,\nbronchospasm, masks hypoglycemia,\nlipid changes",
"HFrEF, post-MI, angina, AF rate\ncontrol, pregnancy (labetalol).\nAVOID: asthma, severe bradycardia"],
["MRA / K-sparing",
"Spironolactone\nEplerenone",
"Block aldosterone receptor\n→ Na excretion, K retention",
"Hyperkalemia, gynecomastia\n(spironolactone), menstrual changes",
"Resistant HTN (4th-line add-on);\nHFrEF, post-MI with HF;\nprimary hyperaldosteronism"],
["Alpha-1 Blockers",
"Doxazosin\nPrazosin\nPhentolamine (IV)",
"Block α1 receptors\n→ vasodilation",
"First-dose orthostatic\nhypotension, reflex tachycardia",
"HTN + BPH; phaeochromocytoma\n(phentolamine FIRST before β-blocker).\nNot first-line alone"],
["Central α2-Agonists",
"Methyldopa\nClonidine",
"Stimulate α2 receptors in CNS\n→ reduce sympathetic outflow",
"Sedation, dry mouth;\nrebound HTN on withdrawal\n(clonidine)",
"Methyldopa: drug of choice in\npregnancy. Clonidine: resistant HTN.\nNot 1st-line otherwise"],
]
dc_data = [dc_header] + [[p(r[0], cell_bold)] + [p(x, cell_body) for x in r[1:]] for r in dc_rows]
row_colors_dc = [LTBLUE, LTTEAL, LTBLUE, LTTEAL, LTBLUE, LTTEAL,
LTBLUE, LTTEAL, LTBLUE, LTTEAL]
dc_tbl = Table(dc_data, colWidths=dc_col_w_pts, repeatRows=1)
dc_style = [
("BACKGROUND", (0,0), (-1,0), colors.HexColor("#1e5e3e")),
("TEXTCOLOR", (0,0), (-1,0), WHITE),
("FONTNAME", (0,0), (-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,0), 8),
("ALIGN", (0,0), (-1,0), "CENTER"),
("VALIGN", (0,0), (-1,-1),"MIDDLE"),
("TOPPADDING", (0,0), (-1,-1), 3),
("BOTTOMPADDING",(0,0), (-1,-1), 3),
("LEFTPADDING", (0,0), (-1,-1), 4),
("RIGHTPADDING", (0,0), (-1,-1), 4),
("GRID", (0,0), (-1,-1), 0.4, GREY2),
("FONTNAME", (0,1), (0,-1), "Helvetica-Bold"),
]
for i, bg in enumerate(row_colors_dc, start=1):
dc_style.append(("BACKGROUND", (0,i), (-1,i), bg))
dc_tbl.setStyle(TableStyle(dc_style))
elems.append(dc_tbl)
elems.append(Spacer(1, 4*mm))
return elems
# ─────────────────────────────────────────────────────────────────────────────
# PAGE 2 – Special Situations + Hypertensive Emergency + Avoid table
# ─────────────────────────────────────────────────────────────────────────────
def build_page2():
elems = []
elems.append(PageBreak())
# Header (repeat)
header_data = [[p("BP MEDICATIONS | QUICK REFERENCE CHART (Page 2)", title_style)]]
header_tbl = Table(header_data, colWidths=[267*mm])
header_tbl.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), NAVY),
("TOPPADDING", (0,0), (-1,-1), 8),
("BOTTOMPADDING",(0,0),(-1,-1), 6),
("ROUNDEDCORNERS",(0,0),(-1,-1), 6),
]))
elems.append(header_tbl)
elems.append(Spacer(1, 4*mm))
# ── Algorithm box ─────────────────────────────────────────────────────
algo_hdr = Table([[p("STEP-UP TREATMENT ALGORITHM (Uncomplicated HTN)", section_style)]],
colWidths=[267*mm])
algo_hdr.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), AMBER),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING",(0,0),(-1,-1), 5),
("ROUNDEDCORNERS",(0,0),(-1,-1), 4),
]))
elems.append(algo_hdr)
elems.append(Spacer(1, 2*mm))
algo_col_w = [25, 55, 110, 77]
algo_data = [
[p("Step", cell_center_bold), p("Regimen", cell_center_bold),
p("Detail", cell_center_bold), p("When to use", cell_center_bold)],
[p("1", cell_center_bold),
p("Dual combination", cell_bold),
p("ACEi or ARB + CCB or Thiazide diuretic", cell_body),
p("All patients BP ≥140/90 mmHg\n(monotherapy if BP just >140/90 or very elderly)", cell_body)],
[p("2", cell_center_bold),
p("Triple combination", cell_bold),
p("ACEi or ARB + CCB + Thiazide diuretic", cell_body),
p("Dual combo insufficient to reach target", cell_body)],
[p("3", cell_center_bold),
p("Resistant HTN", cell_bold),
p("Triple combo + Spironolactone 25-50 mg OD\n(or alpha-blocker or beta-blocker)", cell_body),
p("BP still uncontrolled on 3 drugs;\nrefer to specialist", cell_body)],
[p("★", cell_center_bold),
p("Beta-blockers", cell_bold),
p("Add at ANY step if specific indication present", cell_body),
p("HFrEF, angina, AF, post-MI,\npregnancy (labetalol)", cell_body)],
]
algo_tbl = Table(algo_data, colWidths=[x*mm for x in algo_col_w], repeatRows=1)
algo_tbl.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), colors.HexColor("#9b5e04")),
("TEXTCOLOR", (0,0), (-1,0), WHITE),
("FONTNAME", (0,0), (-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,0), 8),
("ALIGN", (0,0), (-1,0), "CENTER"),
("VALIGN", (0,0), (-1,-1),"MIDDLE"),
("TOPPADDING", (0,0), (-1,-1), 4),
("BOTTOMPADDING",(0,0), (-1,-1), 4),
("LEFTPADDING", (0,0), (-1,-1), 5),
("RIGHTPADDING", (0,0), (-1,-1), 5),
("GRID", (0,0), (-1,-1), 0.4, GREY2),
("ROWBACKGROUNDS",(0,1),(-1,-1),[LTAMBER, WHITE, LTAMBER, WHITE]),
("FONTNAME", (0,1), (1,-1), "Helvetica-Bold"),
("BACKGROUND", (0,4), (-1,4), colors.HexColor("#fff0d0")),
]))
elems.append(algo_tbl)
elems.append(Spacer(1, 4*mm))
# ── Two-column section: Special Situations | Hypertensive Emergency ──
# Special situations table
sp_hdr_data = [[p("SPECIAL CLINICAL SITUATIONS", section_style)]]
sp_hdr_tbl = Table(sp_hdr_data, colWidths=[130*mm])
sp_hdr_tbl.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), colors.HexColor("#5b2d8e")),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING",(0,0),(-1,-1), 5),
("ROUNDEDCORNERS",(0,0),(-1,-1), 4),
]))
sp_rows = [
[p("Situation", cell_center_bold), p("Preferred Drug(s)", cell_center_bold)],
[p("Pregnancy", cell_bold), p("Methyldopa | Labetalol | Nifedipine SR", cell_body)],
[p("Elderly / Isolated systolic HTN", cell_bold), p("Amlodipine | Chlorthalidone", cell_body)],
[p("Black / African-descent patients", cell_bold), p("CCB or Thiazide (RAS blockers less\neffective as monotherapy)", cell_body)],
[p("CKD + Proteinuria", cell_bold), p("ACEi or ARB (renoprotective)", cell_body)],
[p("Metabolic syndrome / Pre-diabetes", cell_bold), p("ACEi or ARB or CCB\n(avoid thiazide+BB combo)", cell_body)],
[p("Post-renal transplant", cell_bold), p("CCB (amlodipine) — first-line", cell_body)],
[p("Bilateral renal artery stenosis", cell_bold), p("CCB or diuretic\n(AVOID ACEi / ARBs)", cell_body)],
[p("Aortic aneurysm / Marfan syndrome", cell_bold), p("Beta-blocker (atenolol/metoprolol)\nor ARB (losartan)", cell_body)],
[p("Migraines", cell_bold), p("Beta-blocker (propranolol, metoprolol)\nor verapamil", cell_body)],
[p("Raynaud's phenomenon", cell_bold), p("Amlodipine (vasodilatory CCB)\nAVOID non-selective beta-blockers", cell_body)],
[p("Hyperthyroidism / Thyroid storm", cell_bold), p("Beta-blocker (propranolol)", cell_body)],
]
sp_tbl = Table(sp_rows, colWidths=[50*mm, 78*mm])
sp_tbl.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), colors.HexColor("#5b2d8e")),
("TEXTCOLOR", (0,0), (-1,0), WHITE),
("FONTNAME", (0,0), (-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,0), 7.5),
("ALIGN", (0,0), (-1,0), "CENTER"),
("VALIGN", (0,0), (-1,-1),"MIDDLE"),
("TOPPADDING", (0,0), (-1,-1), 3),
("BOTTOMPADDING",(0,0), (-1,-1), 3),
("LEFTPADDING", (0,0), (-1,-1), 4),
("RIGHTPADDING", (0,0), (-1,-1), 4),
("GRID", (0,0), (-1,-1), 0.4, GREY2),
("ROWBACKGROUNDS",(0,1),(-1,-1),[colors.HexColor("#f3eeff"), WHITE]),
("FONTNAME", (0,1), (0,-1), "Helvetica-Bold"),
]))
# Hypertensive emergency table
em_hdr_data = [[p("HYPERTENSIVE EMERGENCY – IV Agents", section_style)]]
em_hdr_tbl = Table(em_hdr_data, colWidths=[131*mm])
em_hdr_tbl.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), RED),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING",(0,0),(-1,-1), 5),
("ROUNDEDCORNERS",(0,0),(-1,-1), 4),
]))
em_rows = [
[p("Emergency Type", cell_center_bold), p("Preferred Agent(s)", cell_center_bold), p("Avoid", cell_center_bold)],
[p("Hypertensive\nEncephalopathy", cell_bold), p("Nicardipine, Labetalol,\nClevidipine", cell_body),
p("Nitroprusside", cell_body)],
[p("Acute Ischemic\nStroke", cell_bold), p("Nicardipine, Labetalol,\nClevidipine", cell_body),
p("Nitroprusside, Nimodipine", cell_body)],
[p("Haemorrhagic\nStroke", cell_bold), p("Nicardipine, Labetalol", cell_body),
p("Nitroprusside", cell_body)],
[p("Aortic Dissection", cell_bold), p("Esmolol (IV) + Nitroprusside\nor Labetalol", cell_body),
p("Hydralazine\n(reflex tachycardia)", cell_body)],
[p("Acute Pulmonary\nOedema", cell_bold), p("IV Nitroglycerine +\nFurosemide + Nicardipine", cell_body),
p("Beta-blockers", cell_body)],
[p("Acute MI + HTN", cell_bold), p("Beta-blocker +\nNitroglycerine + ACEi", cell_body),
p("Hydralazine", cell_body)],
[p("Eclampsia /\nSevere pre-eclampsia", cell_bold), p("IV Hydralazine, IV Labetalol,\nIV MgSO4 (seizures)", cell_body),
p("ACEi, ARBs", cell_body)],
[p("Phaeochromocytoma\nCrisis", cell_bold), p("Phentolamine (alpha-blocker)\nTHEN beta-blocker", cell_body),
p("Beta-blocker FIRST\n(paradoxical HTN!)", cell_body)],
[p("Renal Crisis\n(Scleroderma)", cell_bold), p("ACE Inhibitor\n(captopril)", cell_body),
p("ARB (less evidence)", cell_body)],
]
em_tbl = Table(em_rows, colWidths=[38*mm, 54*mm, 39*mm])
em_tbl.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), RED),
("TEXTCOLOR", (0,0), (-1,0), WHITE),
("FONTNAME", (0,0), (-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,0), 7.5),
("ALIGN", (0,0), (-1,0), "CENTER"),
("VALIGN", (0,0), (-1,-1),"MIDDLE"),
("TOPPADDING", (0,0), (-1,-1), 3),
("BOTTOMPADDING",(0,0), (-1,-1), 3),
("LEFTPADDING", (0,0), (-1,-1), 4),
("RIGHTPADDING", (0,0), (-1,-1), 4),
("GRID", (0,0), (-1,-1), 0.4, GREY2),
("ROWBACKGROUNDS",(0,1),(-1,-1),[LTRED, WHITE]),
("FONTNAME", (0,1), (0,-1), "Helvetica-Bold"),
]))
# Side-by-side layout
two_col_header = Table(
[[sp_hdr_tbl, Spacer(6*mm, 1), em_hdr_tbl]],
colWidths=[130*mm, 6*mm, 131*mm]
)
two_col_header.setStyle(TableStyle([
("VALIGN", (0,0), (-1,-1), "TOP"),
("TOPPADDING", (0,0), (-1,-1), 0),
("BOTTOMPADDING", (0,0), (-1,-1), 0),
("LEFTPADDING", (0,0), (-1,-1), 0),
("RIGHTPADDING", (0,0), (-1,-1), 0),
]))
elems.append(two_col_header)
elems.append(Spacer(1, 2*mm))
two_col = Table(
[[sp_tbl, Spacer(6*mm, 1), em_tbl]],
colWidths=[130*mm, 6*mm, 131*mm]
)
two_col.setStyle(TableStyle([
("VALIGN", (0,0), (-1,-1), "TOP"),
("TOPPADDING", (0,0), (-1,-1), 0),
("BOTTOMPADDING", (0,0), (-1,-1), 0),
("LEFTPADDING", (0,0), (-1,-1), 0),
("RIGHTPADDING", (0,0), (-1,-1), 0),
]))
elems.append(two_col)
elems.append(Spacer(1, 4*mm))
# ── AVOID table ───────────────────────────────────────────────────────
av_hdr = Table([[p("DRUGS TO AVOID IN SPECIFIC CONDITIONS", section_style)]],
colWidths=[267*mm])
av_hdr.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), RED),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING",(0,0),(-1,-1), 5),
("ROUNDEDCORNERS",(0,0),(-1,-1), 4),
]))
elems.append(av_hdr)
elems.append(Spacer(1, 2*mm))
av_col_w = [65, 202]
av_rows = [
[p("Condition", cell_center_bold), p("Drug(s) to Avoid (with reason)", cell_center_bold)],
[p("Pregnancy", cell_bold), p("ACEi, ARBs, Direct Renin Inhibitors (aliskiren) – all TERATOGENIC", cell_body)],
[p("Bilateral renal artery stenosis", cell_bold), p("ACEi / ARBs – can precipitate acute renal failure", cell_body)],
[p("Hyperkalaemia", cell_bold), p("ACEi, ARBs, MRA (spironolactone), K-sparing diuretics – worsen hyperkalaemia", cell_body)],
[p("Asthma / COPD", cell_bold), p("Non-selective beta-blockers (propranolol) – bronchospasm; use cardioselective (bisoprolol) with caution only if essential", cell_body)],
[p("AV block (2nd / 3rd degree)", cell_bold), p("Verapamil, Diltiazem, Beta-blockers – worsen AV conduction block; risk of asystole", cell_body)],
[p("Gout", cell_bold), p("Thiazide diuretics – raise serum uric acid; worsen gout attacks", cell_body)],
[p("Decompensated / acute HF", cell_bold), p("Verapamil, Non-DHP CCBs – negative inotropy worsens acute failure", cell_body)],
[p("Phaeochromocytoma", cell_bold), p("Beta-blockers FIRST without alpha-blockade – causes paradoxical severe HTN (unopposed alpha stimulation)", cell_body)],
[p("Metabolic syndrome / Diabetes risk", cell_bold), p("Thiazide + Beta-blocker combination – synergistically worsen insulin resistance and glucose tolerance", cell_body)],
]
av_tbl = Table(av_rows, colWidths=[x*mm for x in av_col_w])
av_tbl.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), RED),
("TEXTCOLOR", (0,0), (-1,0), WHITE),
("FONTNAME", (0,0), (-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,0), 8),
("ALIGN", (0,0), (-1,0), "CENTER"),
("VALIGN", (0,0), (-1,-1),"MIDDLE"),
("TOPPADDING", (0,0), (-1,-1), 3),
("BOTTOMPADDING",(0,0), (-1,-1), 3),
("LEFTPADDING", (0,0), (-1,-1), 5),
("RIGHTPADDING", (0,0), (-1,-1), 5),
("GRID", (0,0), (-1,-1), 0.4, GREY2),
("ROWBACKGROUNDS",(0,1),(-1,-1),[LTRED, WHITE]),
("FONTNAME", (0,1), (0,-1), "Helvetica-Bold"),
]))
elems.append(av_tbl)
elems.append(Spacer(1, 4*mm))
# ── Footer note ───────────────────────────────────────────────────────
elems.append(HRFlowable(width="100%", thickness=0.5, color=GREY2))
elems.append(Spacer(1, 2*mm))
elems.append(p(
"Sources: JNC 7 Guidelines | ACC/AHA 2018 | Comprehensive Clinical Nephrology 7e | "
"NKF Primer 8e | Textbook of Family Medicine 9e | Goldman-Cecil Medicine | Lippincott Pharmacology | "
"For clinical decisions, always verify against current local guidelines.",
small_note
))
return elems
# ── BUILD PDF ─────────────────────────────────────────────────────────────────
doc = SimpleDocTemplate(
OUTPUT,
pagesize=landscape(A4),
leftMargin=12*mm, rightMargin=12*mm,
topMargin=10*mm, bottomMargin=10*mm
)
story = build_page1() + build_page2()
doc.build(story)
print(f"PDF created: {OUTPUT}")
cd /home/daytona/workspace/bp-chart && python3 generate_bp_chart.py 2>&1
ls -lh /home/daytona/workspace/bp-chart/BP_Medications_QuickRef.pdf
BP Medications QuickRef
PDF Document · PDF
- Compelling Indications table (JNC 7 / ACC-AHA 2018) - checkmark grid across all 11 conditions vs 6 drug classes
- Full Drug Class Summary - mechanism, examples, side effects, and key indications for all 10 drug classes (thiazides through central agonists)
- Step-up Treatment Algorithm (dual → triple → resistant HTN)
- Special Clinical Situations (pregnancy, elderly, black patients, CKD, Raynaud's, etc.)
- Hypertensive Emergency IV agents by emergency type (with "Avoid" column)
- Drugs to Avoid table with reasons
Unable to download
ls -lh /home/daytona/workspace/bp-chart/ && file /home/daytona/workspace/bp-chart/BP_Medications_QuickRef.pdf
cp /home/daytona/workspace/bp-chart/BP_Medications_QuickRef.pdf /home/daytona/workspace/BP_Medications_QuickRef.pdf && ls -lh /home/daytona/workspace/BP_Medications_QuickRef.pdf
python3 -c " import base64 with open('/home/daytona/workspace/BP_Medications_QuickRef.pdf','rb') as f: data = base64.b64encode(f.read()).decode() html = f'''<!DOCTYPE html> <html> <head><title>BP Medications Quick Reference</title></head> <body style=\"font-family:Arial;text-align:center;padding:40px\"> <h2>BP Medications Quick Reference Chart</h2> <p>Click the button below to download your PDF:</p> <a href=\"data:application/pdf;base64,{data}\" download=\"BP_Medications_QuickRef.pdf\"> <button style=\"padding:16px 32px;font-size:18px;background:#1a3a5c;color:white;border:none;border-radius:8px;cursor:pointer\"> Download PDF </button> </a> <p style=\"margin-top:20px;color:#666;font-size:13px\">Print at A4 landscape for best results</p> </body> </html>''' with open('/home/daytona/workspace/bp-chart/download.html','w') as f: f.write(html) print('HTML created, size:', len(html), 'chars') "
BP Medications QuickRef
PDF Document · PDF
download
HTML File · HTML

Still showing this
~/bp-chart/BP_Medications_Chart.html
<!DOCTYPE html>
<html lang="en">
<head>
<meta charset="UTF-8">
<meta name="viewport" content="width=device-width, initial-scale=1.0">
<title>BP Medications Quick Reference</title>
<style>
* { box-sizing: border-box; margin: 0; padding: 0; }
body { font-family: Arial, sans-serif; font-size: 12px; background: #f5f7fa; color: #1a1a1a; }
.page { max-width: 1100px; margin: 0 auto; padding: 16px; }
.header {
background: linear-gradient(135deg, #1a3a5c, #2a6090);
color: white; text-align: center;
padding: 14px 10px 10px; border-radius: 8px; margin-bottom: 12px;
}
.header h1 { font-size: 22px; letter-spacing: 1px; margin-bottom: 4px; }
.header p { font-size: 11px; color: #b0d0e8; }
.section-title {
color: white; font-size: 13px; font-weight: bold;
padding: 7px 12px; border-radius: 6px; margin-bottom: 6px;
text-align: center; letter-spacing: 0.5px;
}
.teal { background: #1a7a8a; }
.green { background: #1e5e3e; }
.amber { background: #d4830a; }
.purple { background: #5b2d8e; }
.red { background: #c0392b; }
.navy { background: #1a3a5c; }
table { width: 100%; border-collapse: collapse; margin-bottom: 14px; font-size: 11.5px; }
th { padding: 7px 8px; text-align: center; font-size: 12px; }
td { padding: 6px 8px; vertical-align: middle; border: 1px solid #dce0e5; }
tr:nth-child(even) td { background: #f2f4f6; }
tr:nth-child(odd) td { background: #ffffff; }
.td-label { font-weight: bold; }
/* Compelling indications */
#ci th { background: #1a3a5c; color: white; border: 1px solid #2a5c8a; }
#ci .td-label { background: #dceef5 !important; }
#ci td { text-align: center; }
#ci td:first-child { text-align: left; }
.tick { color: #1e7d44; font-size: 15px; font-weight: bold; }
.dash { color: #aaa; }
/* Drug class table */
#dc th { background: #1e5e3e; color: white; border: 1px solid #2a8a5e; }
#dc .td-label { background: #dceef5 !important; }
#dc tr:nth-child(even) td { background: #d4f0f0; }
#dc tr:nth-child(odd) td { background: #ffffff; }
/* Algorithm */
#algo th { background: #9b5e04; color: white; border: 1px solid #d4830a; }
#algo tr:nth-child(even) td { background: #fdf3dc; }
#algo tr:nth-child(odd) td { background: #ffffff; }
#algo .td-label { font-weight: bold; }
.algo-star td { background: #fff0d0 !important; }
/* Two-col layout */
.two-col { display: flex; gap: 14px; margin-bottom: 14px; }
.two-col > div { flex: 1; }
/* Special situations */
#sp th { background: #5b2d8e; color: white; border: 1px solid #7b4dae; }
#sp .td-label { background: #f3eeff !important; }
#sp tr:nth-child(even) td { background: #f3eeff; }
#sp tr:nth-child(odd) td { background: #ffffff; }
/* Emergency */
#em th { background: #c0392b; color: white; border: 1px solid #e05040; }
#em .td-label { background: #fde8e6 !important; }
#em tr:nth-child(even) td { background: #fde8e6; }
#em tr:nth-child(odd) td { background: #ffffff; }
/* Avoid */
#av th { background: #c0392b; color: white; border: 1px solid #e05040; }
#av .td-label { background: #fde8e6 !important; }
#av tr:nth-child(even) td { background: #fde8e6; }
#av tr:nth-child(odd) td { background: #ffffff; }
.page-break { border: none; border-top: 3px dashed #ccc; margin: 20px 0; }
.footer { text-align: center; font-size: 10px; color: #777; margin-top: 8px; padding: 8px; border-top: 1px solid #dce0e5; }
.print-btn {
display: block; margin: 0 auto 16px; padding: 12px 30px;
background: #1a3a5c; color: white; font-size: 15px; font-weight: bold;
border: none; border-radius: 8px; cursor: pointer; letter-spacing: 0.5px;
}
.print-btn:hover { background: #2a6090; }
@media print {
.print-btn { display: none !important; }
body { background: white; font-size: 10px; }
.page { padding: 8px; max-width: 100%; }
.header h1 { font-size: 16px; }
.two-col { gap: 8px; }
td, th { padding: 4px 5px; font-size: 9.5px; }
.section-title { font-size: 11px; padding: 5px 8px; }
@page { size: A4 landscape; margin: 8mm; }
}
</style>
</head>
<body>
<div class="page">
<button class="print-btn" onclick="window.print()">🖨️ Print / Save as PDF</button>
<!-- HEADER -->
<div class="header">
<h1>BP MEDICATIONS — QUICK REFERENCE CHART</h1>
<p>JNC 7 · ACC/AHA 2018 · Comprehensive Clinical Nephrology 7e · NKF Primer 8e</p>
</div>
<!-- SECTION 1: Compelling Indications -->
<div class="section-title teal">COMPELLING INDICATIONS (JNC 7 / ACC-AHA 2018)</div>
<table id="ci">
<thead><tr>
<th style="text-align:left">Condition</th>
<th>Diuretic<br>(Thiazide)</th>
<th>Beta-<br>Blocker</th>
<th>ACE<br>Inhibitor</th>
<th>ARB</th>
<th>CCB</th>
<th>MRA<br>(Spiro)</th>
<th>Notes</th>
</tr></thead>
<tbody>
<tr><td class="td-label">Heart Failure (HFrEF)</td><td><span class="tick">✔</span></td><td><span class="tick">✔</span></td><td><span class="tick">✔</span></td><td><span class="tick">✔</span></td><td><span class="dash">—</span></td><td><span class="tick">✔</span></td><td>Avoid verapamil / diltiazem</td></tr>
<tr><td class="td-label">Post-MI</td><td><span class="dash">—</span></td><td><span class="tick">✔</span></td><td><span class="tick">✔</span></td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td><span class="tick">✔</span></td><td>Beta-blocker within 24 h</td></tr>
<tr><td class="td-label">High CAD Risk / Angina</td><td><span class="tick">✔</span></td><td><span class="tick">✔</span></td><td><span class="tick">✔</span></td><td><span class="dash">—</span></td><td><span class="tick">✔</span></td><td><span class="dash">—</span></td><td>CCB: prefer amlodipine</td></tr>
<tr><td class="td-label">Diabetes Mellitus</td><td><span class="tick">✔</span></td><td><span class="tick">✔</span></td><td><span class="tick">✔</span></td><td><span class="tick">✔</span></td><td><span class="tick">✔</span></td><td><span class="dash">—</span></td><td>ACEi/ARB renoprotective</td></tr>
<tr><td class="td-label">CKD / Proteinuria</td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td><span class="tick">✔</span></td><td><span class="tick">✔</span></td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td>ACEi or ARB first-line</td></tr>
<tr><td class="td-label">Stroke Prevention (Recurrent)</td><td><span class="tick">✔</span></td><td><span class="dash">—</span></td><td><span class="tick">✔</span></td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td>Thiazide + ACEi combo</td></tr>
<tr><td class="td-label">Atrial Fibrillation (Rate control)</td><td><span class="dash">—</span></td><td><span class="tick">✔</span></td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td>✔ non-DHP<br>(diltiazem)</td><td><span class="dash">—</span></td><td>Avoid DHP CCBs alone</td></tr>
<tr><td class="td-label">Pregnancy</td><td><span class="dash">—</span></td><td>✔ Labetalol only</td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td>✔ Nifedipine SR</td><td><span class="dash">—</span></td><td>Methyldopa also safe</td></tr>
<tr><td class="td-label">BPH</td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td>Alpha-blocker (doxazosin)</td></tr>
<tr><td class="td-label">Phaeochromocytoma</td><td><span class="dash">—</span></td><td>✔ After alpha-block</td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td>Phentolamine FIRST, then BB</td></tr>
</tbody>
</table>
<!-- SECTION 2: Drug Classes -->
<div class="section-title green">DRUG CLASS SUMMARY — Mechanisms, Side Effects & Key Indications</div>
<table id="dc">
<thead><tr>
<th style="text-align:left">Drug Class</th>
<th>Examples</th>
<th>Mechanism</th>
<th>Side Effects</th>
<th style="text-align:left">Key Indications / Notes</th>
</tr></thead>
<tbody>
<tr><td class="td-label">Thiazide / Thiazide-like Diuretics</td><td>HCTZ, Chlorthalidone, Indapamide</td><td>Inhibit Na-Cl cotransporter (DCT)</td><td>Hypokalemia, hyperuricemia, hyperglycemia, dyslipidemia</td><td>First-line uncomplicated HTN; HF; CAD; stroke. Chlorthalidone preferred over HCTZ.</td></tr>
<tr><td class="td-label">Loop Diuretics</td><td>Furosemide, Bumetanide</td><td>Inhibit Na-K-2Cl cotransporter (thick ascending limb)</td><td>Hypokalemia, ototoxicity, dehydration</td><td>HTN + volume overload; HF; CKD with GFR <30 (thiazides lose efficacy)</td></tr>
<tr><td class="td-label">ACE Inhibitors</td><td>Ramipril, Lisinopril, Enalapril, Perindopril</td><td>Block Ang I → Ang II conversion; bradykinin accumulation</td><td>Dry cough (10-15%), hyperkalemia, ↑creatinine, angioedema (rare)</td><td>HF, post-MI, CKD with proteinuria, diabetes, stroke. AVOID: pregnancy, bilateral RAS.</td></tr>
<tr><td class="td-label">ARBs (Angiotensin Receptor Blockers)</td><td>Losartan, Valsartan, Telmisartan, Irbesartan</td><td>Block Ang II at AT1 receptor (no bradykinin)</td><td>Similar to ACEi — NO cough; rare angioedema</td><td>Same as ACEi. Preferred when ACEi cough intolerable. AVOID: pregnancy, bilateral RAS.</td></tr>
<tr><td class="td-label">Dihydropyridine CCBs (DHP)</td><td>Amlodipine, Nifedipine SR, Felodipine</td><td>Block L-type Ca²⁺ channels → vasodilation</td><td>Peripheral edema, flushing, gingival hyperplasia</td><td>Uncomplicated HTN, elderly, isolated systolic HTN, angina, CKD, black patients, diabetes</td></tr>
<tr><td class="td-label">Non-DHP CCBs</td><td>Diltiazem, Verapamil</td><td>Block L-type Ca²⁺ channels + AV nodal depression</td><td>Bradycardia, AV block; verapamil: constipation</td><td>HTN + angina + AF rate control. AVOID: HFrEF, AV block, combined with beta-blockers.</td></tr>
<tr><td class="td-label">Beta-Blockers</td><td>Metoprolol, Atenolol, Carvedilol, Bisoprolol, Labetalol (IV/oral)</td><td>Block β1 (and β2 if non-selective) adrenergic receptors</td><td>Fatigue, bradycardia, bronchospasm, masks hypoglycemia</td><td>HFrEF, post-MI, angina, AF rate control, pregnancy (labetalol). AVOID: asthma, severe bradycardia.</td></tr>
<tr><td class="td-label">MRA / K-sparing (Spironolactone)</td><td>Spironolactone, Eplerenone</td><td>Block aldosterone receptor → Na excretion, K retention</td><td>Hyperkalemia, gynecomastia (spironolactone), menstrual changes</td><td>Resistant HTN (4th-line add-on); HFrEF; post-MI with HF; primary hyperaldosteronism</td></tr>
<tr><td class="td-label">Alpha-1 Blockers</td><td>Doxazosin, Prazosin, Phentolamine (IV)</td><td>Block α1 receptors → vasodilation</td><td>First-dose orthostatic hypotension, reflex tachycardia</td><td>HTN + BPH; phaeochromocytoma (phentolamine FIRST before β-blocker). Not first-line alone.</td></tr>
<tr><td class="td-label">Central α2-Agonists</td><td>Methyldopa, Clonidine</td><td>Stimulate α2 in CNS → reduce sympathetic outflow</td><td>Sedation, dry mouth; rebound HTN on withdrawal (clonidine)</td><td>Methyldopa: drug of choice in pregnancy. Clonidine: resistant HTN. Not 1st-line otherwise.</td></tr>
</tbody>
</table>
<hr class="page-break">
<!-- SECTION 3: Algorithm -->
<div class="section-title amber">STEP-UP TREATMENT ALGORITHM (Uncomplicated HTN)</div>
<table id="algo">
<thead><tr>
<th>Step</th><th>Regimen</th><th>Detail</th><th>When to Use</th>
</tr></thead>
<tbody>
<tr><td style="text-align:center;font-weight:bold">1</td><td class="td-label">Dual combination</td><td><strong>ACEi or ARB + CCB</strong> or <strong>Thiazide diuretic</strong></td><td>All patients BP ≥140/90 mmHg (monotherapy if BP just >140/90 or very elderly/frail)</td></tr>
<tr><td style="text-align:center;font-weight:bold">2</td><td class="td-label">Triple combination</td><td><strong>ACEi or ARB + CCB + Thiazide diuretic</strong></td><td>Dual combo insufficient to reach BP target</td></tr>
<tr><td style="text-align:center;font-weight:bold">3</td><td class="td-label">Resistant HTN</td><td>Triple combo + <strong>Spironolactone 25–50 mg OD</strong> (or alpha-blocker or beta-blocker)</td><td>BP uncontrolled on 3 drugs; refer to specialist</td></tr>
<tr class="algo-star"><td style="text-align:center;font-weight:bold">★</td><td class="td-label">Beta-blockers</td><td>Add at <strong>ANY step</strong> when specific indication present</td><td>HFrEF, angina, AF, post-MI, pregnancy (labetalol)</td></tr>
</tbody>
</table>
<!-- SECTION 4: Two-col -->
<div class="two-col">
<div>
<div class="section-title purple">SPECIAL CLINICAL SITUATIONS</div>
<table id="sp">
<thead><tr><th style="text-align:left">Situation</th><th style="text-align:left">Preferred Drug(s)</th></tr></thead>
<tbody>
<tr><td class="td-label">Pregnancy</td><td>Methyldopa | Labetalol | Nifedipine SR</td></tr>
<tr><td class="td-label">Elderly / Isolated systolic HTN</td><td>Amlodipine | Chlorthalidone</td></tr>
<tr><td class="td-label">Black / African-descent patients</td><td>CCB or Thiazide (RAS blockers less effective as monotherapy)</td></tr>
<tr><td class="td-label">CKD + Proteinuria</td><td>ACEi or ARB (renoprotective)</td></tr>
<tr><td class="td-label">Metabolic syndrome / Pre-diabetes</td><td>ACEi or ARB or CCB (avoid thiazide+BB combo)</td></tr>
<tr><td class="td-label">Post-renal transplant</td><td>CCB (amlodipine) — first-line</td></tr>
<tr><td class="td-label">Bilateral renal artery stenosis</td><td>CCB or diuretic (AVOID ACEi / ARBs)</td></tr>
<tr><td class="td-label">Aortic aneurysm / Marfan</td><td>Beta-blocker (atenolol) or ARB (losartan)</td></tr>
<tr><td class="td-label">Migraines</td><td>Beta-blocker (propranolol, metoprolol) or verapamil</td></tr>
<tr><td class="td-label">Raynaud's phenomenon</td><td>Amlodipine. AVOID non-selective beta-blockers.</td></tr>
<tr><td class="td-label">Hyperthyroidism / Thyroid storm</td><td>Beta-blocker (propranolol)</td></tr>
</tbody>
</table>
</div>
<div>
<div class="section-title red">HYPERTENSIVE EMERGENCY — IV Agents</div>
<table id="em">
<thead><tr><th style="text-align:left">Emergency Type</th><th>Preferred Agent(s)</th><th>Avoid</th></tr></thead>
<tbody>
<tr><td class="td-label">HTN Encephalopathy</td><td>Nicardipine, Labetalol, Clevidipine</td><td>Nitroprusside</td></tr>
<tr><td class="td-label">Acute Ischaemic Stroke</td><td>Nicardipine, Labetalol, Clevidipine</td><td>Nitroprusside, Nimodipine</td></tr>
<tr><td class="td-label">Haemorrhagic Stroke</td><td>Nicardipine, Labetalol</td><td>Nitroprusside</td></tr>
<tr><td class="td-label">Aortic Dissection</td><td>Esmolol IV + Nitroprusside or Labetalol</td><td>Hydralazine (reflex tachycardia)</td></tr>
<tr><td class="td-label">Acute Pulmonary Oedema</td><td>IV Nitroglycerine + Furosemide + Nicardipine</td><td>Beta-blockers</td></tr>
<tr><td class="td-label">Acute MI + HTN</td><td>Beta-blocker + Nitroglycerine + ACEi</td><td>Hydralazine</td></tr>
<tr><td class="td-label">Eclampsia / Severe Pre-eclampsia</td><td>IV Hydralazine, IV Labetalol, IV MgSO4 (seizures)</td><td>ACEi, ARBs</td></tr>
<tr><td class="td-label">Phaeochromocytoma Crisis</td><td>Phentolamine (alpha-blocker) THEN beta-blocker</td><td>Beta-blocker FIRST (paradoxical HTN!)</td></tr>
<tr><td class="td-label">Scleroderma Renal Crisis</td><td>ACE Inhibitor (captopril)</td><td>ARB (less evidence)</td></tr>
</tbody>
</table>
<p style="font-size:10.5px;color:#c0392b;font-weight:bold;margin-top:4px;">⚠ Reduce BP by max 25% in first hour. Never drop too fast — risk of ischaemia.</p>
</div>
</div>
<!-- SECTION 5: Avoid -->
<div class="section-title red">DRUGS TO AVOID IN SPECIFIC CONDITIONS</div>
<table id="av">
<thead><tr>
<th style="text-align:left">Condition</th>
<th style="text-align:left">Drug(s) to Avoid & Reason</th>
</tr></thead>
<tbody>
<tr><td class="td-label">Pregnancy</td><td>ACEi, ARBs, Direct Renin Inhibitors (aliskiren) — all TERATOGENIC</td></tr>
<tr><td class="td-label">Bilateral renal artery stenosis</td><td>ACEi / ARBs — can precipitate acute renal failure</td></tr>
<tr><td class="td-label">Hyperkalaemia</td><td>ACEi, ARBs, MRA (spironolactone), K-sparing diuretics — worsen hyperkalaemia</td></tr>
<tr><td class="td-label">Asthma / COPD</td><td>Non-selective beta-blockers (propranolol) — bronchospasm. Use cardioselective (bisoprolol) with caution if essential.</td></tr>
<tr><td class="td-label">AV block (2nd / 3rd degree)</td><td>Verapamil, Diltiazem, Beta-blockers — worsen conduction block; risk of asystole</td></tr>
<tr><td class="td-label">Gout</td><td>Thiazide diuretics — raise serum uric acid; worsen gout attacks</td></tr>
<tr><td class="td-label">Decompensated / acute HF</td><td>Verapamil, Non-DHP CCBs — negative inotropy worsens acute failure</td></tr>
<tr><td class="td-label">Phaeochromocytoma</td><td>Beta-blockers FIRST (without alpha-blockade) — paradoxical severe HTN from unopposed alpha stimulation</td></tr>
<tr><td class="td-label">Metabolic syndrome / Diabetes risk</td><td>Thiazide + Beta-blocker combination — synergistically worsen insulin resistance and glucose tolerance</td></tr>
</tbody>
</table>
<div class="footer">
Sources: JNC 7 Guidelines · ACC/AHA 2018 · Comprehensive Clinical Nephrology 7e · NKF Primer 8e · Textbook of Family Medicine 9e · Goldman-Cecil Medicine · Lippincott Pharmacology<br>
For clinical decisions, always verify against current local guidelines.
</div>
<button class="print-btn" onclick="window.print()" style="margin-top:14px">🖨️ Print / Save as PDF</button>
</div>
</body>
</html>
python3 -c " import base64 with open('/home/daytona/workspace/bp-chart/BP_Medications_Chart.html', 'rb') as f: content = f.read() b64 = base64.b64encode(content).decode() data_uri = 'data:text/html;base64,' + b64 # Write a tiny launcher HTML with the data URI as an href launcher = '''<!DOCTYPE html> <html> <head><meta charset=\"UTF-8\"><title>BP Chart Launcher</title> <style>body{font-family:Arial;text-align:center;padding:50px;background:#f0f4f8;} .btn{display:inline-block;padding:18px 36px;background:#1a3a5c;color:white;font-size:18px;font-weight:bold;border-radius:10px;text-decoration:none;margin:10px;} p{color:#555;margin:10px 0;} </style></head> <body> <h2 style=\"color:#1a3a5c\">BP Medications Quick Reference</h2> <p>Tap the button to open the chart, then use your browser menu to print or save as PDF.</p> <a class=\"btn\" href=\"''' + data_uri + '''\" target=\"_blank\">Open Chart</a> <p style=\"font-size:12px;color:#888;margin-top:20px\">After opening: tap ⋮ menu → Print → Save as PDF</p> </body></html>''' with open('/home/daytona/workspace/bp-chart/open_chart.html', 'w') as f: f.write(launcher) print('Launcher created, size:', len(launcher), 'bytes') print('Data URI length:', len(data_uri)) "
How to get your printable PDF (2 easy options):
Option A - Use an online HTML-to-PDF converter (easiest on mobile)
- Go to htmltomd.com or sejda.com/html-to-pdf
- Paste the HTML code below into the text box
- Download the PDF
Option B - Save as HTML and print
- Copy all the HTML code below
- Paste it into a new file called
bp_chart.htmlon your computer - Open in Chrome → Press Ctrl+P (or ⌘+P) → Save as PDF → Set paper to A4 Landscape
<!DOCTYPE html>
<html lang="en">
<head>
<meta charset="UTF-8">
<meta name="viewport" content="width=device-width, initial-scale=1.0">
<title>BP Medications Quick Reference</title>
<style>
*{box-sizing:border-box;margin:0;padding:0}body{font-family:Arial,sans-serif;font-size:12px;background:#f5f7fa;color:#1a1a1a}.page{max-width:1100px;margin:0 auto;padding:16px}.header{background:linear-gradient(135deg,#1a3a5c,#2a6090);color:white;text-align:center;padding:14px 10px 10px;border-radius:8px;margin-bottom:12px}.header h1{font-size:22px;letter-spacing:1px;margin-bottom:4px}.header p{font-size:11px;color:#b0d0e8}.section-title{color:white;font-size:13px;font-weight:bold;padding:7px 12px;border-radius:6px;margin-bottom:6px;text-align:center;letter-spacing:.5px}.teal{background:#1a7a8a}.green{background:#1e5e3e}.amber{background:#d4830a}.purple{background:#5b2d8e}.red{background:#c0392b}.navy{background:#1a3a5c}table{width:100%;border-collapse:collapse;margin-bottom:14px;font-size:11.5px}th{padding:7px 8px;text-align:center;font-size:12px}td{padding:6px 8px;vertical-align:middle;border:1px solid #dce0e5}tr:nth-child(even) td{background:#f2f4f6}tr:nth-child(odd) td{background:#fff}.td-label{font-weight:bold}#ci th{background:#1a3a5c;color:white;border:1px solid #2a5c8a}#ci .td-label{background:#dceef5!important}#ci td{text-align:center}#ci td:first-child{text-align:left}.tick{color:#1e7d44;font-size:15px;font-weight:bold}.dash{color:#aaa}#dc th{background:#1e5e3e;color:white;border:1px solid #2a8a5e}#dc .td-label{background:#dceef5!important}#dc tr:nth-child(even) td{background:#d4f0f0}#dc tr:nth-child(odd) td{background:#fff}#algo th{background:#9b5e04;color:white;border:1px solid #d4830a}#algo tr:nth-child(even) td{background:#fdf3dc}#algo tr:nth-child(odd) td{background:#fff}#algo .td-label{font-weight:bold}.algo-star td{background:#fff0d0!important}.two-col{display:flex;gap:14px;margin-bottom:14px}.two-col>div{flex:1}#sp th{background:#5b2d8e;color:white;border:1px solid #7b4dae}#sp .td-label{background:#f3eeff!important}#sp tr:nth-child(even) td{background:#f3eeff}#sp tr:nth-child(odd) td{background:#fff}#em th{background:#c0392b;color:white;border:1px solid #e05040}#em .td-label{background:#fde8e6!important}#em tr:nth-child(even) td{background:#fde8e6}#em tr:nth-child(odd) td{background:#fff}#av th{background:#c0392b;color:white;border:1px solid #e05040}#av .td-label{background:#fde8e6!important}#av tr:nth-child(even) td{background:#fde8e6}#av tr:nth-child(odd) td{background:#fff}.page-break{border:none;border-top:3px dashed #ccc;margin:20px 0}.footer{text-align:center;font-size:10px;color:#777;margin-top:8px;padding:8px;border-top:1px solid #dce0e5}.print-btn{display:block;margin:0 auto 16px;padding:12px 30px;background:#1a3a5c;color:white;font-size:15px;font-weight:bold;border:none;border-radius:8px;cursor:pointer;letter-spacing:.5px}@media print{.print-btn{display:none!important}body{background:white;font-size:10px}.page{padding:8px;max-width:100%}.header h1{font-size:16px}.two-col{gap:8px}td,th{padding:4px 5px;font-size:9.5px}.section-title{font-size:11px;padding:5px 8px}@page{size:A4 landscape;margin:8mm}}
</style>
</head>
<body>
<div class="page">
<button class="print-btn" onclick="window.print()">🖨️ Print / Save as PDF</button>
<div class="header"><h1>BP MEDICATIONS — QUICK REFERENCE CHART</h1><p>JNC 7 · ACC/AHA 2018 · Comprehensive Clinical Nephrology 7e · NKF Primer 8e</p></div>
<div class="section-title teal">COMPELLING INDICATIONS (JNC 7 / ACC-AHA 2018)</div>
<table id="ci"><thead><tr><th style="text-align:left">Condition</th><th>Diuretic<br>(Thiazide)</th><th>Beta-Blocker</th><th>ACE Inhibitor</th><th>ARB</th><th>CCB</th><th>MRA (Spiro)</th><th>Notes</th></tr></thead><tbody>
<tr><td class="td-label">Heart Failure (HFrEF)</td><td><span class="tick">✔</span></td><td><span class="tick">✔</span></td><td><span class="tick">✔</span></td><td><span class="tick">✔</span></td><td><span class="dash">—</span></td><td><span class="tick">✔</span></td><td>Avoid verapamil / diltiazem</td></tr>
<tr><td class="td-label">Post-MI</td><td><span class="dash">—</span></td><td><span class="tick">✔</span></td><td><span class="tick">✔</span></td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td><span class="tick">✔</span></td><td>Beta-blocker within 24 h</td></tr>
<tr><td class="td-label">High CAD Risk / Angina</td><td><span class="tick">✔</span></td><td><span class="tick">✔</span></td><td><span class="tick">✔</span></td><td><span class="dash">—</span></td><td><span class="tick">✔</span></td><td><span class="dash">—</span></td><td>CCB: prefer amlodipine</td></tr>
<tr><td class="td-label">Diabetes Mellitus</td><td><span class="tick">✔</span></td><td><span class="tick">✔</span></td><td><span class="tick">✔</span></td><td><span class="tick">✔</span></td><td><span class="tick">✔</span></td><td><span class="dash">—</span></td><td>ACEi/ARB renoprotective</td></tr>
<tr><td class="td-label">CKD / Proteinuria</td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td><span class="tick">✔</span></td><td><span class="tick">✔</span></td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td>ACEi or ARB first-line</td></tr>
<tr><td class="td-label">Stroke Prevention (Recurrent)</td><td><span class="tick">✔</span></td><td><span class="dash">—</span></td><td><span class="tick">✔</span></td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td>Thiazide + ACEi combo</td></tr>
<tr><td class="td-label">Atrial Fibrillation (Rate control)</td><td><span class="dash">—</span></td><td><span class="tick">✔</span></td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td>✔ non-DHP (diltiazem)</td><td><span class="dash">—</span></td><td>Avoid DHP CCBs alone</td></tr>
<tr><td class="td-label">Pregnancy</td><td><span class="dash">—</span></td><td>✔ Labetalol only</td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td>✔ Nifedipine SR</td><td><span class="dash">—</span></td><td>Methyldopa also safe</td></tr>
<tr><td class="td-label">BPH</td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td>Alpha-blocker (doxazosin)</td></tr>
<tr><td class="td-label">Phaeochromocytoma</td><td><span class="dash">—</span></td><td>✔ After alpha-block</td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td><span class="dash">—</span></td><td>Phentolamine FIRST, then BB</td></tr>
</tbody></table>
<div class="section-title green">DRUG CLASS SUMMARY — Mechanisms, Side Effects & Key Indications</div>
<table id="dc"><thead><tr><th style="text-align:left">Drug Class</th><th>Examples</th><th>Mechanism</th><th>Side Effects</th><th style="text-align:left">Key Indications / Notes</th></tr></thead><tbody>
<tr><td class="td-label">Thiazide / Thiazide-like Diuretics</td><td>HCTZ, Chlorthalidone, Indapamide</td><td>Inhibit Na-Cl cotransporter (DCT)</td><td>Hypokalemia, hyperuricemia, hyperglycemia, dyslipidemia</td><td>First-line uncomplicated HTN; HF; CAD; stroke. Chlorthalidone preferred over HCTZ.</td></tr>
<tr><td class="td-label">Loop Diuretics</td><td>Furosemide, Bumetanide</td><td>Inhibit Na-K-2Cl cotransporter (thick ascending limb)</td><td>Hypokalemia, ototoxicity, dehydration</td><td>HTN + volume overload; HF; CKD with GFR <30</td></tr>
<tr><td class="td-label">ACE Inhibitors</td><td>Ramipril, Lisinopril, Enalapril</td><td>Block Ang I→Ang II; bradykinin accumulation</td><td>Dry cough (10-15%), hyperkalemia, angioedema</td><td>HF, post-MI, CKD+proteinuria, diabetes, stroke. AVOID: pregnancy, bilateral RAS.</td></tr>
<tr><td class="td-label">ARBs</td><td>Losartan, Valsartan, Telmisartan</td><td>Block Ang II at AT1 receptor (no bradykinin)</td><td>Similar to ACEi — NO cough</td><td>Same as ACEi. Preferred when ACEi cough intolerable. AVOID: pregnancy, bilateral RAS.</td></tr>
<tr><td class="td-label">Dihydropyridine CCBs (DHP)</td><td>Amlodipine, Nifedipine SR, Felodipine</td><td>Block L-type Ca²⁺ → vasodilation</td><td>Peripheral edema, flushing, gingival hyperplasia</td><td>Uncomplicated HTN, elderly, angina, CKD, black patients, diabetes</td></tr>
<tr><td class="td-label">Non-DHP CCBs</td><td>Diltiazem, Verapamil</td><td>Block L-type Ca²⁺ + AV nodal depression</td><td>Bradycardia, AV block; verapamil: constipation</td><td>HTN + angina + AF rate control. AVOID: HFrEF, AV block, with beta-blockers.</td></tr>
<tr><td class="td-label">Beta-Blockers</td><td>Metoprolol, Carvedilol, Bisoprolol, Labetalol</td><td>Block β1 (±β2) adrenergic receptors</td><td>Fatigue, bradycardia, bronchospasm, masks hypoglycemia</td><td>HFrEF, post-MI, angina, AF, pregnancy (labetalol). AVOID: asthma, severe bradycardia.</td></tr>
<tr><td class="td-label">MRA / Spironolactone</td><td>Spironolactone, Eplerenone</td><td>Block aldosterone receptor</td><td>Hyperkalemia, gynecomastia, menstrual changes</td><td>Resistant HTN (4th-line); HFrEF; post-MI with HF; primary hyperaldosteronism</td></tr>
<tr><td class="td-label">Alpha-1 Blockers</td><td>Doxazosin, Prazosin, Phentolamine IV</td><td>Block α1 receptors → vasodilation</td><td>First-dose orthostatic hypotension</td><td>HTN + BPH; phaeochromocytoma (phentolamine FIRST). Not first-line alone.</td></tr>
<tr><td class="td-label">Central α2-Agonists</td><td>Methyldopa, Clonidine</td><td>Stimulate α2 in CNS → reduce sympathetic outflow</td><td>Sedation, dry mouth; rebound HTN (clonidine)</td><td>Methyldopa: drug of choice in pregnancy. Not 1st-line otherwise.</td></tr>
</tbody></table>
<hr class="page-break">
<div class="section-title amber">STEP-UP TREATMENT ALGORITHM (Uncomplicated HTN)</div>
<table id="algo"><thead><tr><th>Step</th><th>Regimen</th><th>Detail</th><th>When to Use</th></tr></thead><tbody>
<tr><td style="text-align:center;font-weight:bold">1</td><td class="td-label">Dual combination</td><td><strong>ACEi or ARB + CCB</strong> or <strong>Thiazide diuretic</strong></td><td>BP ≥140/90 mmHg (monotherapy if just above 140/90 or frail elderly)</td></tr>
<tr><td style="text-align:center;font-weight:bold">2</td><td class="td-label">Triple combination</td><td><strong>ACEi or ARB + CCB + Thiazide diuretic</strong></td><td>Dual combo insufficient to reach BP target</td></tr>
<tr><td style="text-align:center;font-weight:bold">3</td><td class="td-label">Resistant HTN</td><td>Triple combo + Spironolactone 25–50 mg OD (or alpha-blocker or beta-blocker)</td><td>BP uncontrolled on 3 drugs; refer to specialist</td></tr>
<tr class="algo-star"><td style="text-align:center;font-weight:bold">★</td><td class="td-label">Beta-blockers</td><td>Add at ANY step when specific indication present</td><td>HFrEF, angina, AF, post-MI, pregnancy (labetalol)</td></tr>
</tbody></table>
<div class="two-col">
<div>
<div class="section-title purple">SPECIAL CLINICAL SITUATIONS</div>
<table id="sp"><thead><tr><th style="text-align:left">Situation</th><th style="text-align:left">Preferred Drug(s)</th></tr></thead><tbody>
<tr><td class="td-label">Pregnancy</td><td>Methyldopa | Labetalol | Nifedipine SR</td></tr>
<tr><td class="td-label">Elderly / Isolated systolic HTN</td><td>Amlodipine | Chlorthalidone</td></tr>
<tr><td class="td-label">Black / African-descent patients</td><td>CCB or Thiazide (RAS blockers less effective as monotherapy)</td></tr>
<tr><td class="td-label">CKD + Proteinuria</td><td>ACEi or ARB (renoprotective)</td></tr>
<tr><td class="td-label">Metabolic syndrome / Pre-diabetes</td><td>ACEi or ARB or CCB (avoid thiazide+BB combo)</td></tr>
<tr><td class="td-label">Post-renal transplant</td><td>CCB (amlodipine) — first-line</td></tr>
<tr><td class="td-label">Bilateral renal artery stenosis</td><td>CCB or diuretic (AVOID ACEi / ARBs)</td></tr>
<tr><td class="td-label">Aortic aneurysm / Marfan</td><td>Beta-blocker (atenolol) or ARB (losartan)</td></tr>
<tr><td class="td-label">Migraines</td><td>Beta-blocker (propranolol, metoprolol) or verapamil</td></tr>
<tr><td class="td-label">Raynaud's phenomenon</td><td>Amlodipine. AVOID non-selective beta-blockers.</td></tr>
<tr><td class="td-label">Hyperthyroidism / Thyroid storm</td><td>Beta-blocker (propranolol)</td></tr>
</tbody></table>
</div>
<div>
<div class="section-title red">HYPERTENSIVE EMERGENCY — IV Agents</div>
<table id="em"><thead><tr><th style="text-align:left">Emergency Type</th><th>Preferred Agents</th><th>Avoid</th></tr></thead><tbody>
<tr><td class="td-label">HTN Encephalopathy</td><td>Nicardipine, Labetalol, Clevidipine</td><td>Nitroprusside</td></tr>
<tr><td class="td-label">Acute Ischaemic Stroke</td><td>Nicardipine, Labetalol, Clevidipine</td><td>Nitroprusside, Nimodipine</td></tr>
<tr><td class="td-label">Haemorrhagic Stroke</td><td>Nicardipine, Labetalol</td><td>Nitroprusside</td></tr>
<tr><td class="td-label">Aortic Dissection</td><td>Esmolol IV + Nitroprusside or Labetalol</td><td>Hydralazine</td></tr>
<tr><td class="td-label">Acute Pulmonary Oedema</td><td>IV Nitroglycerine + Furosemide + Nicardipine</td><td>Beta-blockers</td></tr>
<tr><td class="td-label">Acute MI + HTN</td><td>Beta-blocker + Nitroglycerine + ACEi</td><td>Hydralazine</td></tr>
<tr><td class="td-label">Eclampsia / Pre-eclampsia</td><td>IV Hydralazine, IV Labetalol, IV MgSO4</td><td>ACEi, ARBs</td></tr>
<tr><td class="td-label">Phaeochromocytoma Crisis</td><td>Phentolamine THEN beta-blocker</td><td>Beta-blocker FIRST!</td></tr>
<tr><td class="td-label">Scleroderma Renal Crisis</td><td>ACE Inhibitor (captopril)</td><td>ARB (less evidence)</td></tr>
</tbody></table>
<p style="font-size:10.5px;color:#c0392b;font-weight:bold;margin-top:4px;">⚠ Reduce BP max 25% in first hour. Avoid rapid drops — risk of ischaemia.</p>
</div></div>
<div class="section-title red">DRUGS TO AVOID IN SPECIFIC CONDITIONS</div>
<table id="av"><thead><tr><th style="text-align:left">Condition</th><th style="text-align:left">Drug(s) to Avoid & Reason</th></tr></thead><tbody>
<tr><td class="td-label">Pregnancy</td><td>ACEi, ARBs, Direct Renin Inhibitors — all TERATOGENIC</td></tr>
<tr><td class="td-label">Bilateral renal artery stenosis</td><td>ACEi / ARBs — can precipitate acute renal failure</td></tr>
<tr><td class="td-label">Hyperkalaemia</td><td>ACEi, ARBs, MRA (spironolactone), K-sparing diuretics</td></tr>
<tr><td class="td-label">Asthma / COPD</td><td>Non-selective beta-blockers (propranolol) — bronchospasm</td></tr>
<tr><td class="td-label">AV block (2nd / 3rd degree)</td><td>Verapamil, Diltiazem, Beta-blockers — risk of asystole</td></tr>
<tr><td class="td-label">Gout</td><td>Thiazide diuretics — raise serum uric acid</td></tr>
<tr><td class="td-label">Decompensated / acute HF</td><td>Verapamil, Non-DHP CCBs — negative inotropy worsens acute failure</td></tr>
<tr><td class="td-label">Phaeochromocytoma</td><td>Beta-blockers FIRST (without alpha-blockade) — paradoxical severe HTN</td></tr>
<tr><td class="td-label">Metabolic syndrome / Diabetes risk</td><td>Thiazide + Beta-blocker combination — worsen insulin resistance</td></tr>
</tbody></table>
<div class="footer">Sources: JNC 7 · ACC/AHA 2018 · Comprehensive Clinical Nephrology 7e · NKF Primer 8e · Textbook of Family Medicine 9e · Goldman-Cecil Medicine · Lippincott Pharmacology<br>For clinical decisions, always verify against current local guidelines.</div>
<button class="print-btn" onclick="window.print()" style="margin-top:14px">🖨️ Print / Save as PDF</button>
</div></body></html>
- Copy the code above
- Open a new Chrome tab → type
data:text/html,in the address bar → paste the code after the comma → tap Go - Tap the Print / Save as PDF button that appears on the page
- Select Save as PDF from the print menu