Hi
Hey! How can I help you today?
Conjoint tendon
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a complete overview of the conjoint tendon:
Conjoint Tendon (Inguinal Falx / Falx Inguinalis)
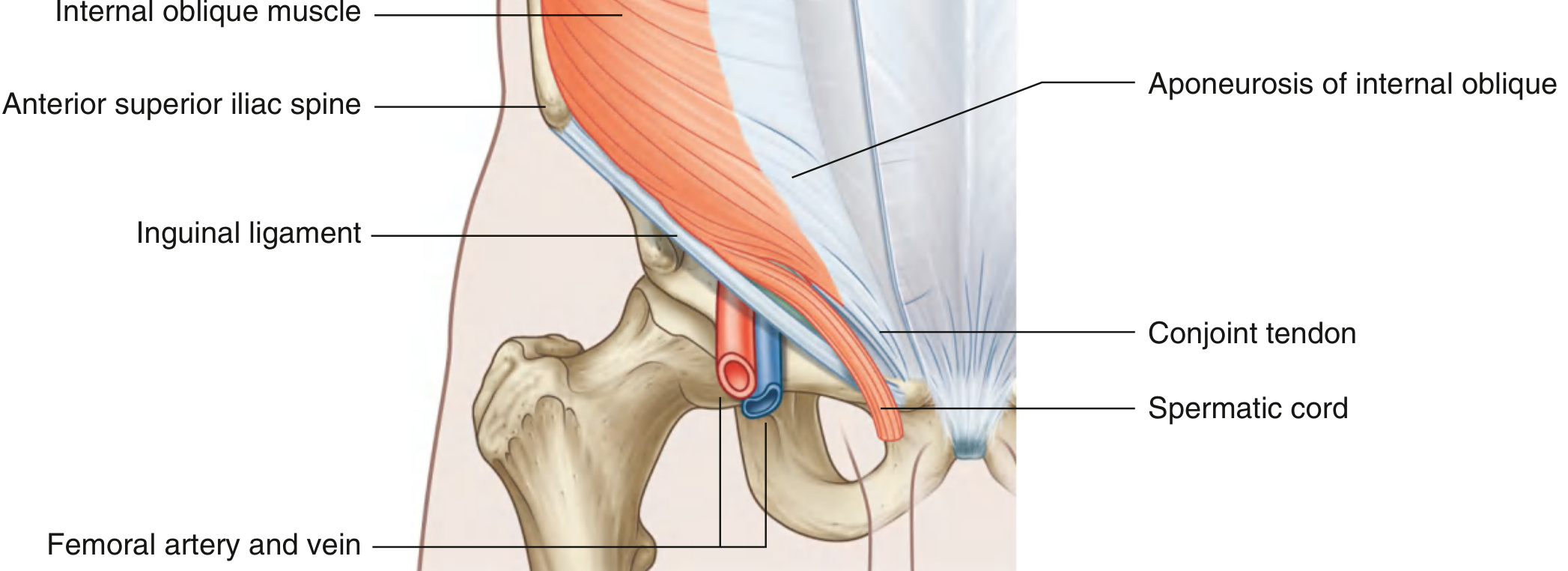
Formation
The conjoint tendon is formed by the fusion of the aponeuroses of two muscles:
- Internal oblique (IO) muscle
- Transversus abdominis (TA) muscle
Their medial aponeurotic fibers join together, most prominently near the pubic tubercle.
Important note: According to Sabiston Textbook of Surgery, a true fused conjoint tendon is actually present in only about 5% of patients. In most people, the IO and TA aponeuroses remain separate or are only loosely approximated. The term is used loosely in clinical and surgical contexts.
Insertion
- Pubic crest and pectineal line of the pubis
Location / Relations
- Lies medially in the groin
- Sits posterior to the superficial (external) inguinal ring, reinforcing it from behind
- The arching fibers of the IO and TA form the roof of the inguinal canal, converging medially as they descend to become the conjoint tendon
Role in Inguinal Canal Walls
| Wall | Structure |
|---|---|
| Anterior | Aponeurosis of external oblique (+ IO laterally) |
| Posterior | Transversalis fascia (+ conjoint tendon reinforces the medial 1/3) |
| Roof | Arching fibers of IO and TA (become conjoint tendon medially) |
| Floor | Inguinal ligament (medial half) |
Clinical Significance
- Direct inguinal hernia: Occurs through Hesselbach's triangle, medial to the inferior epigastric vessels. Weakness or thinning of the posterior wall (where the conjoint tendon should reinforce) predisposes to this hernia type.
- Hernia repair: In open inguinal hernia repair (e.g., Bassini, Shouldice), the conjoint tendon (or the IO-TA aponeurotic arch) is sutured to the inguinal or Cooper's ligament to reconstruct the posterior inguinal wall.
- Shoulder surgery: The term "conjoint tendon" is also used in the shoulder for the combined tendon of coracobrachialis and the short head of biceps brachii, which arise together from the coracoid process - this is a completely different structure relevant in deltopectoral approaches.
Also Called
- Inguinal falx
- Falx inguinalis
- (In surgery texts) - the "triple layer" of IO + TA + cremasteric fascia
- Gray's Anatomy for Students, p. 354
- Sabiston Textbook of Surgery, p. 1680
What is fascia transversalis
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a detailed account of the transversalis fascia:
Transversalis Fascia (Endoabdominal Fascia)
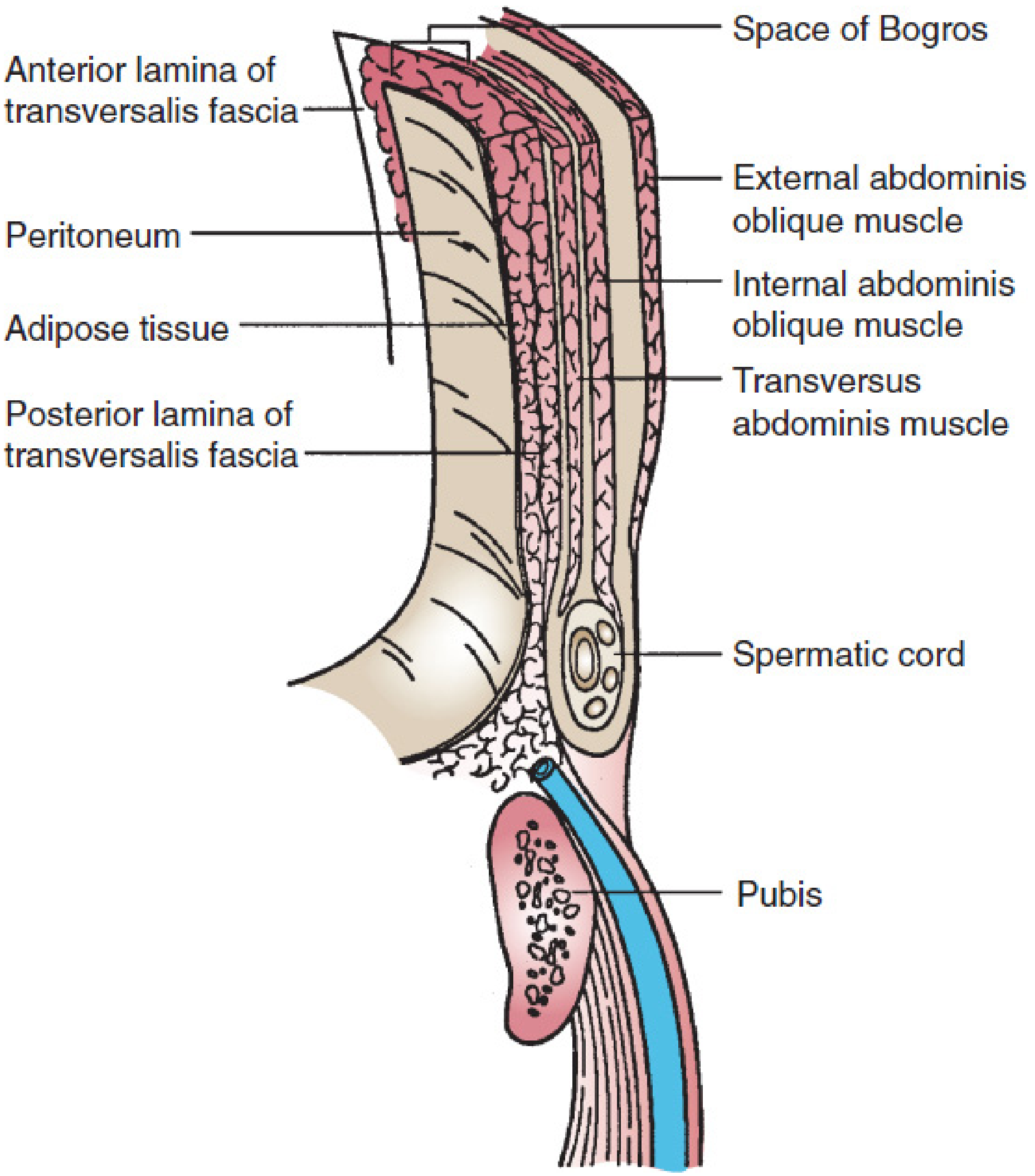
Definition
The transversalis fascia is a continuous sheet of connective tissue that lines the inner (deep) surface of the transversus abdominis muscle and extends throughout the entire extraperitoneal space. It is also called the endoabdominal fascia. Where it overlies specific muscles, it takes regional names (e.g., iliac fascia over the iliacus, psoas fascia over the psoas).
According to Mulholland & Greenfield's Surgery, it is "perhaps the most commonly misunderstood structure in the literature devoted to groin hernia," because different surgeons may be referring to very different structures when they use the term.
Layers - Is it One or Two?
There is debate:
- Most authors: a single layer
- Others: two laminae (the bilaminar view)
- Anterior lamina: more uniform; adherent to the deep surface of the transversus abdominis and rectus abdominis
- Posterior lamina: variable in density; interspersed with adipose tissue; lies within the preperitoneal space (between peritoneum and the anterior lamina); the inferior epigastric vessels run within this layer
The preperitoneal (Space of Bogros) is defined as the space between the peritoneum and the anterior lamina of the transversalis fascia.
Role in the Inguinal Region
| Structure | Contribution |
|---|---|
| Posterior wall of inguinal canal | Formed entirely by transversalis fascia |
| Deep inguinal ring | An oval defect/outpouching in the transversalis fascia where the spermatic cord (or round ligament) exits |
| Internal spermatic fascia | Derived from the transversalis fascia as it evaginates around the spermatic cord at the deep ring |
| Final common denominator of all groin hernias | Failure of the transversalis fascia to contain intra-abdominal contents |
Derivatives / Analogs
The transversalis fascia condenses or thickens at several locations to form important structures:
-
Iliopubic tract - the thickened band of transversalis fascia at the zone of transition between iliacus and transversus abdominis; runs parallel to (but posterior to) the inguinal ligament; extends from the iliac crest to the pubic tubercle. Critical landmark in laparoscopic hernia repair - nerves of the lumbar plexus run below it, so tacks/staples must not be placed inferior to it.
-
Iliopectineal arch - condenses where it overlies the iliopsoas; separates the vascular compartment (femoral vessels) from the neuromuscular compartment (iliopsoas, femoral nerve, lateral femoral cutaneous nerve). Contributes to the femoral sheath.
-
Crura of the deep inguinal ring - the superior and inferior crura form a transversalis fascia sling shaped like a "monk's hood" around the deep inguinal ring. When the transversus abdominis contracts, the crura are pulled upward and laterally, producing a valvular action that actively prevents indirect herniation.
Clinical Significance
- Hernia formation: All groin hernias ultimately represent failure of the transversalis fascia. Direct hernias arise through a weakened posterior wall; indirect hernias pass through the deep inguinal ring.
- Bassini / Shouldice repair: Both operations rely on tightening the internal ring and suturing the transversalis fascia (together with the transversus abdominis aponeurosis) to the inguinal ligament as the primary repair step.
- Laparoscopic hernia repair (TEP/TAPP): The surgeon works in the preperitoneal space, posterior to the transversalis fascia, making a thorough understanding of its layers and derivatives essential for safe dissection.
- Robustness: It tends to be thicker and stronger in the lower abdomen (inguinal region) compared to elsewhere.
- Mulholland & Greenfield's Surgery, p. 3647-3650
- Sabiston Textbook of Surgery, p. 1680
- Gray's Anatomy for Students, p. 352
Show fasica transversalis and conjoint tendon in same picture
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Reading File
Loading Image
This is the image you need. Here are both diagrams showing the conjoint tendon and transversalis fascia together:
Diagram 1 - Bassini's Original Inguinal Canal Anatomy (Bailey & Love's Surgery)
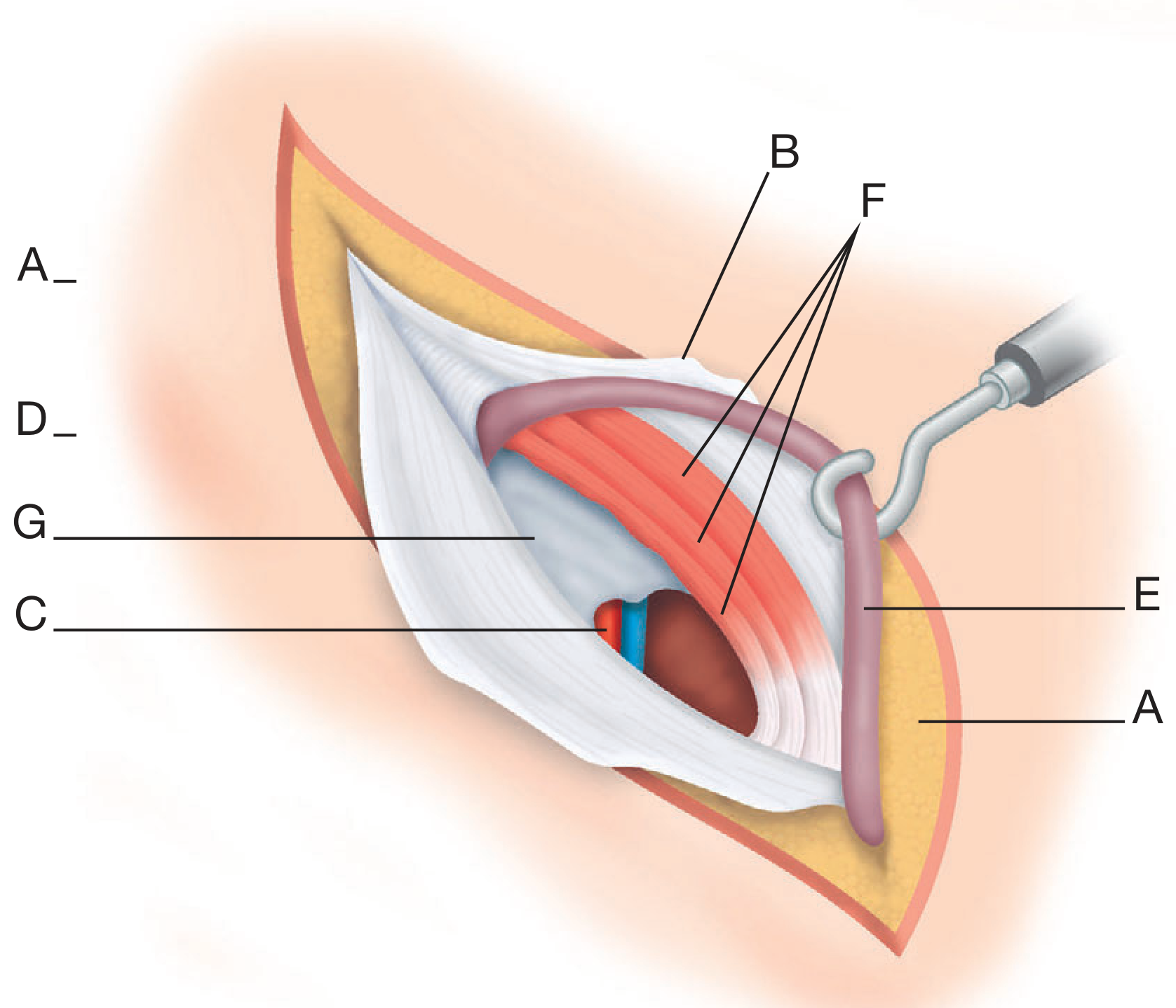
Key labels:
- A - Subcutaneous fat (skin edges)
- B - External oblique aponeurosis (opened and retracted)
- C - Inferior epigastric vessels
- D - Poupart's (inguinal) ligament
- E - Spermatic cord (retracted)
- F - Conjoint tendon (the red/salmon-coloured muscle layer = triple layer of internal oblique + transversus abdominis + cremasteric fascia)
- G - Transversalis fascia (the white shiny layer forming the posterior wall, visible below the conjoint tendon)
Diagram 2 - Sabiston's 3D Inguinal Region
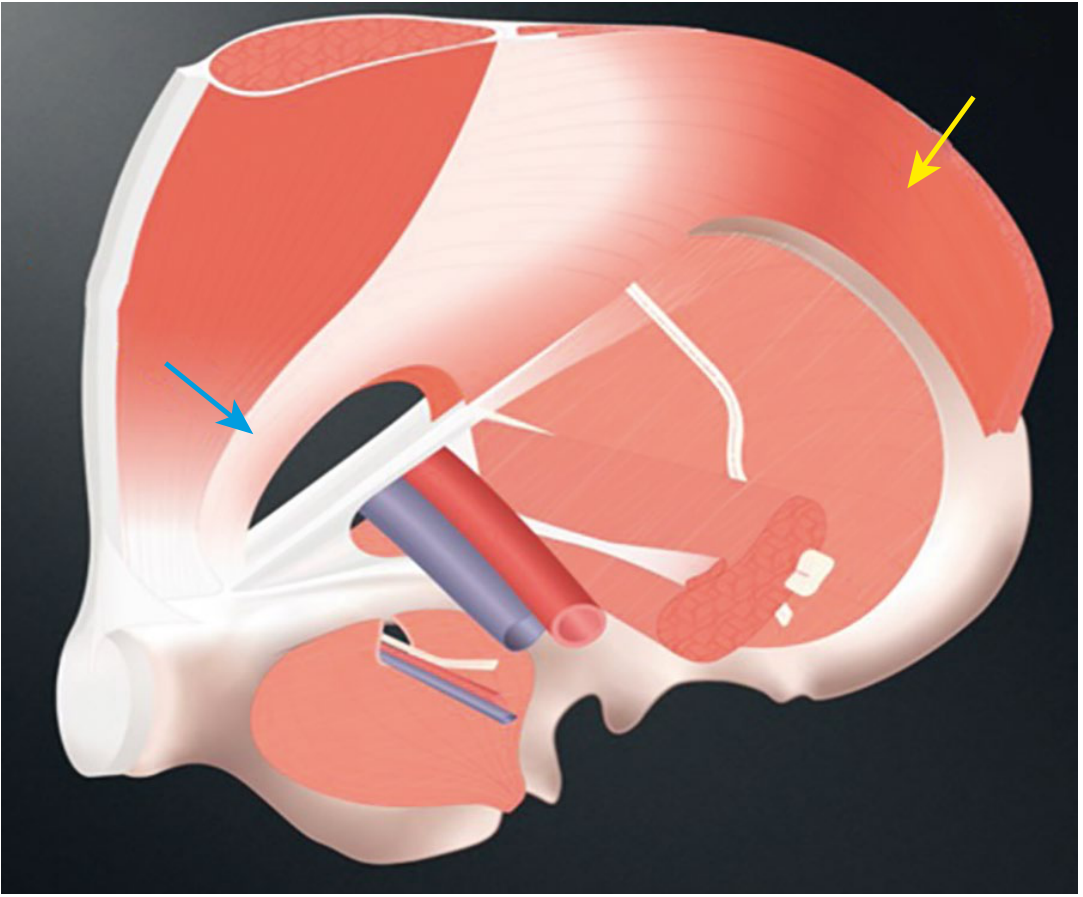
Key arrows:
- Yellow arrow - Transversus abdominis muscle / posterior wall (transversalis fascia)
- Blue arrow - Conjoint tendon inserting medially at the pubic crest
How they relate in these images:
The transversalis fascia (G) is the deep white glistening sheet forming the entire posterior wall of the inguinal canal. The conjoint tendon (F) is the muscular-aponeurotic arch of IO + TA that reinforces only the medial third of this posterior wall, sitting anterior/superior to the transversalis fascia at the medial end.
- Bailey & Love's Short Practice of Surgery, Fig. 64.14, p. 1089
- Sabiston Textbook of Surgery, Fig. 82.9, p. 1683
This is a shared conversation. Sign in to Orris to start your own chat.