Puberty physiology
Reading File
Finding Sources
Searching PubMed
puberty physiology hormones
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks and excellent diagrams. Let me compile the full response.
Puberty Physiology
Puberty is the transition from a juvenile to an adult reproductive state, encompassing the physical, hormonal, and psychological changes that confer the capacity to reproduce. It involves two overlapping processes: gonadarche (maturation of the gonads) and adrenarche (increased adrenal androgen secretion).
1. Overview and Definitions
- Gonadarche: Activation of the gonads by pituitary gonadotropins (FSH and LH), leading to sex steroid and gamete production.
- Adrenarche: Increased secretion of DHEA, DHEAS, and androstenedione from the adrenal cortex, unique to humans and great apes. It occurs at ages 6-8 years in both sexes - before gonadarche. Triggers pubarche (pubic hair growth). Its absence does not prevent gonadarche or reproductive competence.
- Puberty (strictly defined): The point at which endocrine and gametogenic gonadal function has first developed to the point where reproduction is possible.
2. Gonadotropin Secretion Across the Lifespan
The hypothalamic-pituitary axis drives puberty, and its activity changes dramatically across life:
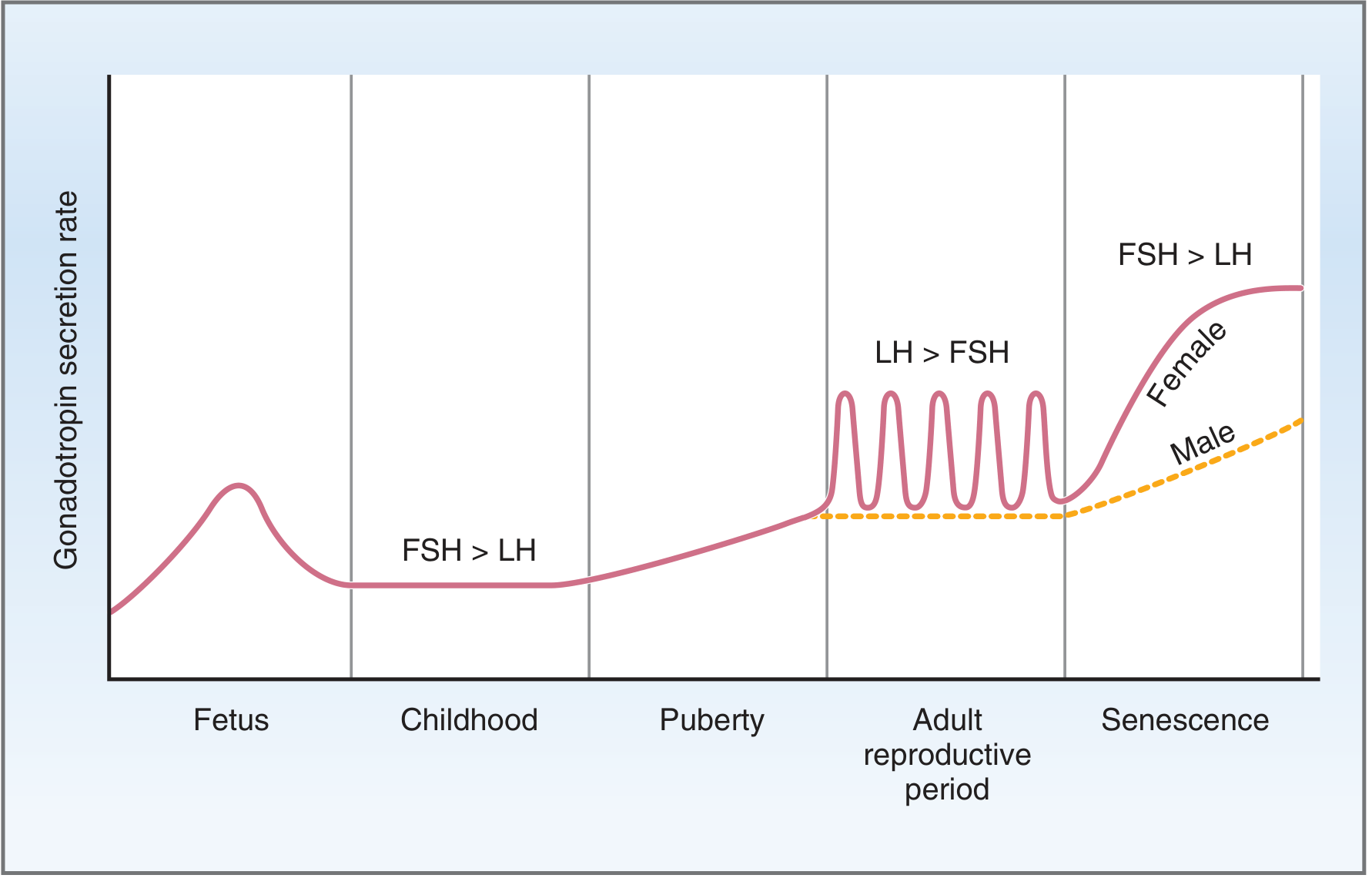
Gonadotropin secretion over the life span (Costanzo Physiology, 7th Ed.)
Key phases:
| Phase | FSH/LH pattern |
|---|---|
| Fetal | GnRH secretion begins at gestational week 4; FSH/LH secretion starts weeks 10-12; peak in 2nd trimester |
| Infancy (mini-puberty) | Second gonadotropin peak at ~2-3 months postnatally |
| Childhood | FSH > LH; both fall to low levels |
| Puberty | Pulsatile GnRH; LH > FSH begins; pulsatility starts nocturnally (REM sleep) |
| Reproductive adult | Cyclic LH surges in females; tonic pattern in males |
| Senescence | FSH > LH again; markedly elevated |
The detailed pattern across a lifetime:
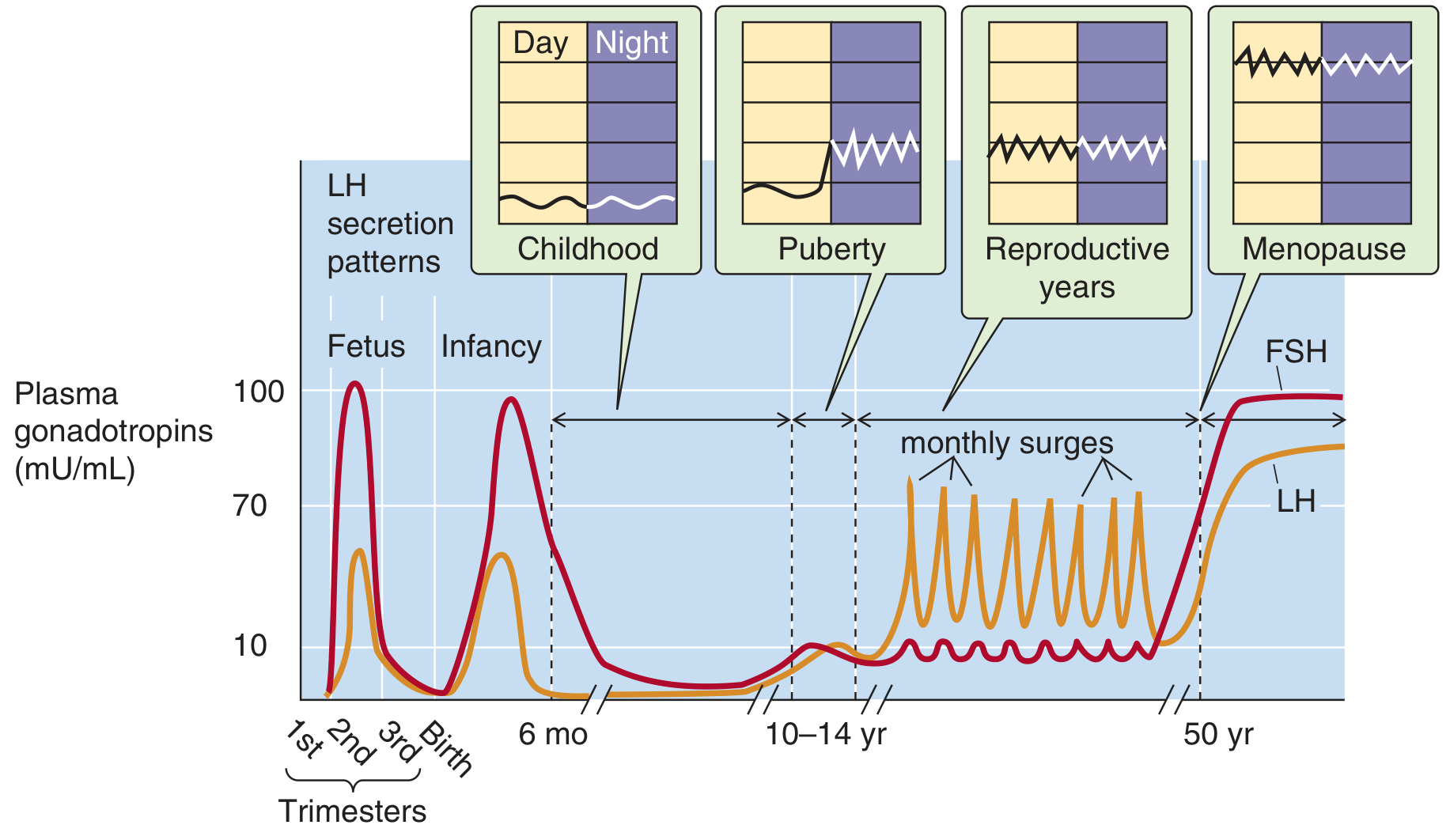
Gonadotropin function during life - Medical Physiology (Boron & Boulpaep)
3. Neuroendocrine Control: The GnRH Pulse Generator
The central event triggering puberty is the onset of pulsatile GnRH secretion from hypothalamic neurons.
Why is GnRH low during childhood?
Before puberty, the hypothalamic-pituitary axis is exquisitely sensitive to negative feedback - even very low circulating sex steroid levels completely suppress gonadotropin release. At puberty, this sensitivity decreases, so progressively higher steroid levels are required to suppress GnRH/LH/FSH. This shift is the permissive event for puberty.
Sequence of events at puberty onset:
- Pulsatile GnRH release begins - initially only during REM sleep at night
- GnRH up-regulates its own receptor (GnRH-R) in the anterior pituitary, amplifying the FSH/LH response
- Nocturnal LH pulses are the earliest measurable hormonal change of puberty
- Pulses gradually become 24-hour, not just nocturnal
- Rising FSH and LH stimulate gonadal steroid secretion
- Sex steroids drive physical pubertal changes
Kisspeptin: Neurons in the arcuate nucleus and anteroventral periventricular nucleus (AVPV) of the hypothalamus secrete kisspeptin (encoded by the KISS1 gene), which acts on GnRH neurons via kisspeptin receptor (GPR54). Kisspeptin signaling is now understood to be a major driver of GnRH pulsatility at puberty onset - mutations in GPR54 cause hypogonadotropic hypogonadism with failure of puberty.
Other regulators of puberty timing:
- Melatonin (pineal gland): Natural inhibitor of GnRH release; levels are highest in childhood and decline at puberty - pinealectomy precipitates early puberty
- Leptin: Adipokine reflecting fat mass; required permissively for puberty onset. Leptin-deficient children fail to enter puberty until treated with leptin
- Genetics: Familial patterns are strong (e.g., age at menarche is similar between mothers and daughters)
- Nutrition: Severe caloric restriction, malnutrition, or heavy exercise delay puberty; obesity can accelerate it
- Geography: Proximity to the equator and lower altitude are associated with earlier puberty
- Secular trend: In the US and Europe, the age of menarche has declined by 1-3 months per decade over the past 175 years
4. Hormone Changes During Puberty
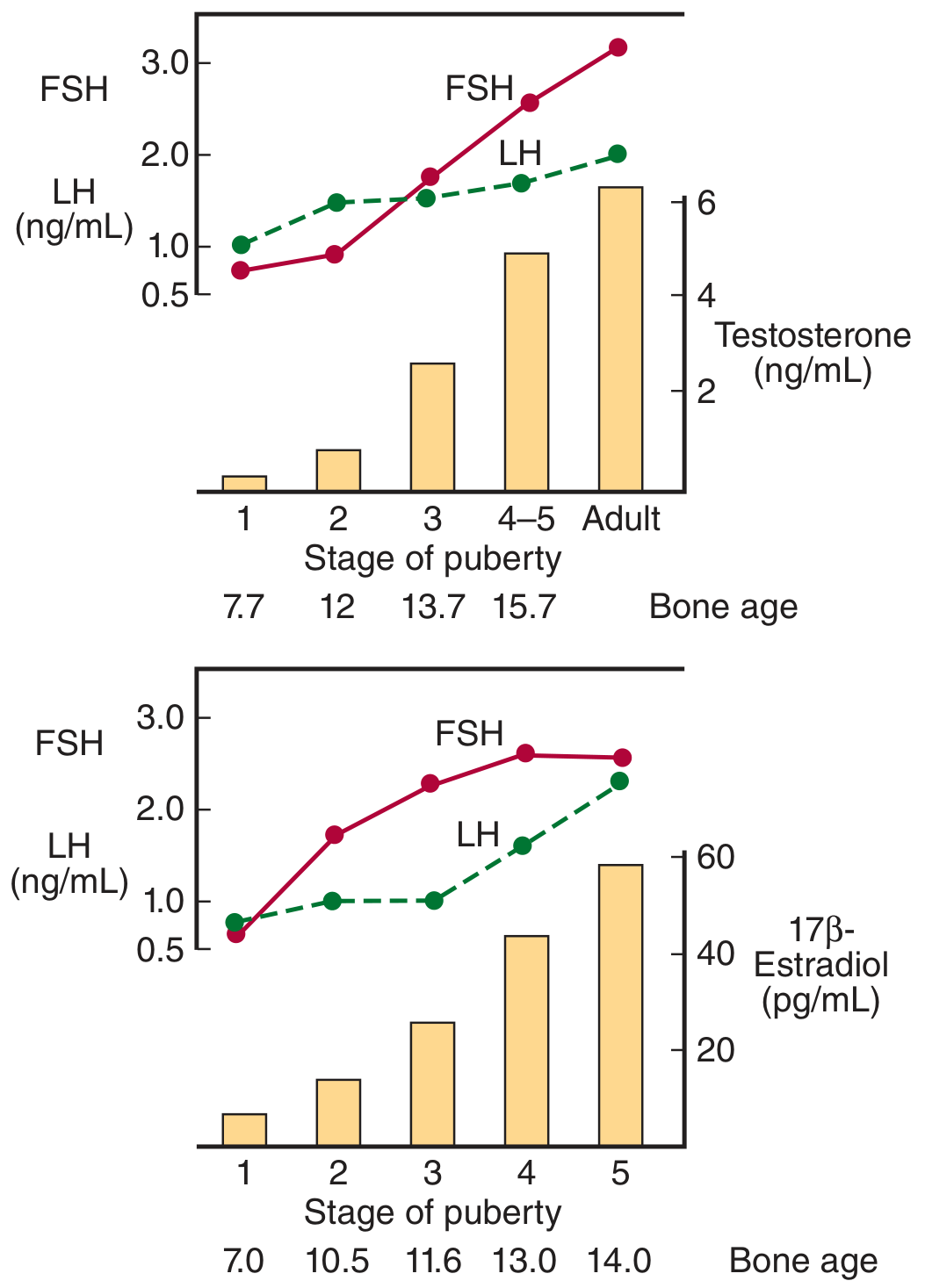
Hormone changes across Tanner stages in boys (top) and girls (bottom) - Ganong's Review of Medical Physiology, 26th Ed.
Males: FSH and LH rise progressively across puberty stages. Testosterone rises dramatically from stage 2 onward, reaching adult levels by stage 4-5. Bone age correlates: ~12 years at stage 2, ~15.7 years by stage 4-5.
Females: FSH rises early and remains higher than LH until ovulatory cycles are established. Estradiol rises progressively, reaching adult levels (~55-65 pg/mL) by stage 5. In girls, in childhood FSH > LH; at puberty and adult reproductive period LH > FSH.
5. Timeline of Pubertal Events
Events of Puberty
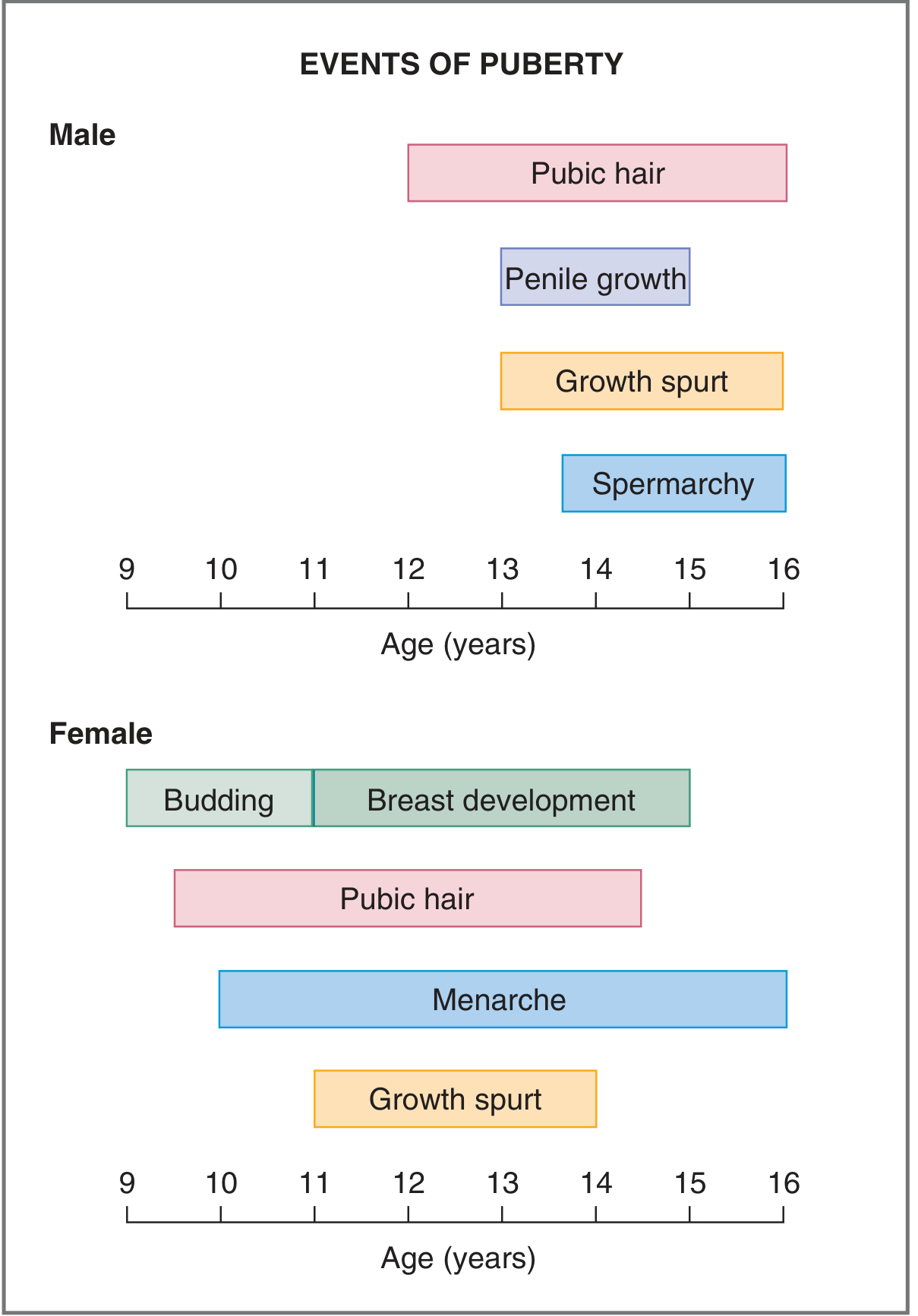
Major events of puberty in males and females (Costanzo Physiology, 7th Ed.)
Males (normal range: 9-14 years onset, complete within 2-4.5 years):
- First sign: Testicular enlargement >2.5 cm (Tanner stage 2) - mainly due to seminiferous tubule growth
- Pubic hair development (1-1.5 years after genital development)
- Penile enlargement (length, then girth)
- Spermarche (initiation of sperm production), usually ~age 14
- Linear growth spurt (peaks later than females, ~age 13-14)
- Deepening of voice (laryngeal growth; vocal cord length increases ~50%)
- Facial and body hair
- Increased muscle mass and nitrogen retention
- Epiphyseal closure when adult height attained
Females (normal range: 8-13 years onset):
- First sign: Thelarche (breast budding, Tanner stage 2), ~age 10-11
- Adrenarche/pubarche (pubic and axillary hair)
- Growth spurt (begins and ends earlier than males)
- Menarche (first menstrual period), ~ages 12-14; initially often anovulatory
- Regular ovulation appears ~1 year after menarche
- Epiphyseal closure
6. Tanner Stages
The Tanner staging system provides standardized assessment of pubertal development in both sexes across 5 stages:
| Stage | Pubic Hair (Both Sexes) | Male Genitalia | Female Breast/Genitalia |
|---|---|---|---|
| 1 | None (only vellus hair) | Preadolescent - same relative size as young child | Only papillae elevated |
| 2 | Sparse, at base of penis or along labia majora | Scrotum and testes enlarged | Breast buds begin; areolar diameter increases |
| 3 | Darker, coarser, curlier; spreads above pubis | Penis enlarged (length); testes further enlarged | Breasts and areolae enlarge; vagina enlarges, begins producing discharge; menses may begin |
| 4 | Adult type, smaller area than adults | Penis enlarged in length and diameter; testes further enlarged | Areolae/papillae project beyond breast tissue; ovulation and menstruation begin (often irregular) |
| 5 | Adult pattern | Adult pattern | Areolae on same level as breast; only papillae project - Adult |
7. Effects of Sex Steroids
Testosterone (Males)
Testosterone acts directly or via metabolites - dihydrotestosterone (DHT) (5α-reduction, more potent at androgen receptor, acts on external genitalia, prostate, skin) and estradiol (aromatization, acts on bone, brain):
- External genitalia: enlargement of penis and scrotum
- Accessory organs: prostate, seminal vesicles begin secreting
- Skin: coarser, oilier (sebum → acne); facial/axillary/pubic hair
- Musculoskeletal: linear growth spurt, muscle mass/strength (especially shoulder girdle), increased bone mineral density, epiphyseal maturation
- Erythropoiesis: higher hematocrit and hemoglobin than females
- Voice: laryngeal thickening, lower voice
- CNS: libido development; spatial cognition
- Spermatogenesis: Leydig cell testosterone + FSH on Sertoli cells → seminiferous tubule maturation
Estrogen (Females)
- Breast development (thelarche)
- Uterine growth and endometrial proliferation
- Vaginal epithelial maturation
- Fat deposition (hips, thighs)
- Skeletal growth spurt; epiphyseal closure (earlier than males due to earlier estrogen rise)
- Bone mineral deposition
- Positive feedback at high concentrations → LH surge → ovulation (established after 1-2 years of anovulatory cycles)
8. The Growth Spurt
Growth hormone (GH) secretion increases at puberty, acting synergistically with sex steroids to produce the growth spurt. Sex steroids stimulate GH secretion and increase hepatic IGF-1 production. The growth spurt in girls precedes that in boys by ~2 years, explaining the shorter average adult height in females. Epiphyseal fusion terminates growth, and the estrogen-mediated acceleration of bone maturation is why girls stop growing earlier.
9. Key Points Summary
| Feature | Males | Females |
|---|---|---|
| Normal onset | 9-14 years | 8-13 years |
| First sign | Testicular enlargement | Thelarche (breast budding) |
| Adrenarche | Age 10-12 yrs | Age 8-10 yrs |
| Key hormone | Testosterone | Estradiol |
| Initiator | GnRH → LH/FSH | GnRH → LH/FSH |
| Gametogenesis | Spermarche | Menarche (then ovulation ~1 yr later) |
| Growth spurt peak | ~Age 13-14 | ~Age 11-12 |
Sources: Medical Physiology (Boron & Boulpaep) | Costanzo Physiology, 7th Ed. | Ganong's Review of Medical Physiology, 26th Ed. | Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.