Lap cholecystectomy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative surgical textbooks. Let me compile the full structured answer.
Laparoscopic Cholecystectomy
Overview
Laparoscopic cholecystectomy (LC) is the gold-standard surgical treatment for symptomatic gallstone disease. It was first performed by Muhe in 1985 (using a direct scope) and then popularized by Mouret in 1987. It is now one of the most commonly performed general surgery operations worldwide, with a reported mortality of 0.1–0.5% and morbidity of 2–3%. - Sabiston Textbook of Surgery, p. 1838
Indications
- Biliary colic (symptomatic cholelithiasis) - the most common indication
- Acute cholecystitis (early LC is the gold standard; higher conversion rate but safe in experienced hands)
- Biliary pancreatitis (mild-moderate; LC should be performed during the same admission or within 2 weeks)
- Chronic cholecystitis
- Gallbladder polyps (>1 cm or symptomatic)
- Biliary dyskinesia
Contraindications
Absolute (Maingot's Abdominal Operations)
| Contraindication | Notes |
|---|---|
| Unable to tolerate general anesthesia | GA with muscle relaxation is mandatory |
| Refractory coagulopathy | Cannot achieve hemostasis |
| Suspicion of gallbladder carcinoma | Mandates open resection; gallbladder perforation (20-30% of LC) risks intraperitoneal dissemination |
Relative
| Contraindication | Notes |
|---|---|
| Previous upper abdominal surgery | Higher adhesions, higher conversion rate |
| Cirrhosis / portal hypertension | Risk of bleeding from portal collaterals |
| Cholangitis / diffuse peritonitis | Higher conversion rate; emergency laparotomy often needed |
| COPD | Impaired CO₂ exchange from pneumoperitoneum |
| Morbid obesity | Technical difficulty; higher conversion |
| Pregnancy | 2nd trimester preferred; insufflation <12 mmHg; use laparoscopic ultrasound instead of cholangiogram to limit fetal radiation; fetal heart monitoring perioperatively |
Preoperative Preparation
- General anesthesia with full muscle relaxation
- Supine positioning, one arm tucked (to allow intraoperative cholangiogram if needed)
- Orogastric tube to decompress stomach
- Foley catheter if prolonged surgery anticipated
- Prep abdomen and lower chest to allow for open conversion if needed
- Patient secured in steep reverse Trendelenburg position
Port Placement (Standard 4-Port Technique)
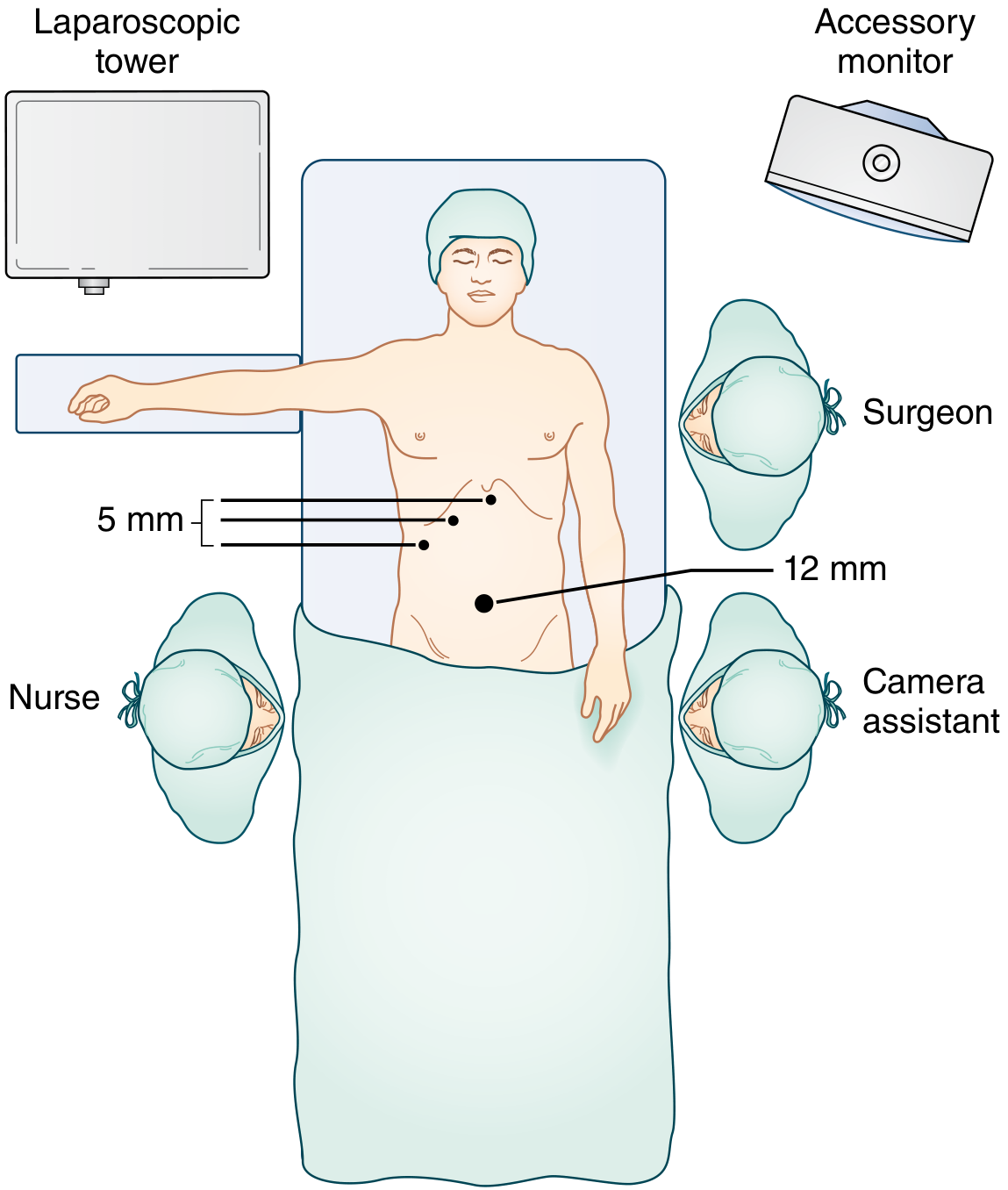
Port placement for laparoscopic cholecystectomy. The 12-mm umbilical port serves for camera and specimen extraction; three 5-mm ports are placed in the right anterior axillary line, right midclavicular line, and subxiphoid position. - Sabiston Textbook of Surgery, p. 1839
| Port | Size | Purpose |
|---|---|---|
| Umbilical (periumbilical) | 12 mm | Camera port; specimen extraction |
| Right anterior axillary line | 5 mm | Fundus retraction (cephalad toward right shoulder) |
| Right midclavicular line | 5 mm | Infundibulum retraction (inferolateral) |
| Subxiphoid | 5 mm | Dissection and clip application |
Alternative: Modified French position - patient in split-leg position; subxiphoid port for fundus retraction; working ports in both upper quadrants.
Operative Steps
1. Fundus Retraction and Exposure
- The gallbladder fundus is grasped and retracted cephalad (toward right shoulder)
- The infundibulum/Hartmann's pouch is retracted inferolaterally to open the hepatocystic triangle (Triangle of Calot)
- Adjacent adherent structures (omentum, duodenum, colon) are bluntly peeled down
2. Critical View of Safety (CVS)
The critical view of safety (Strasberg's CVS) is the key safety measure to prevent bile duct injury:
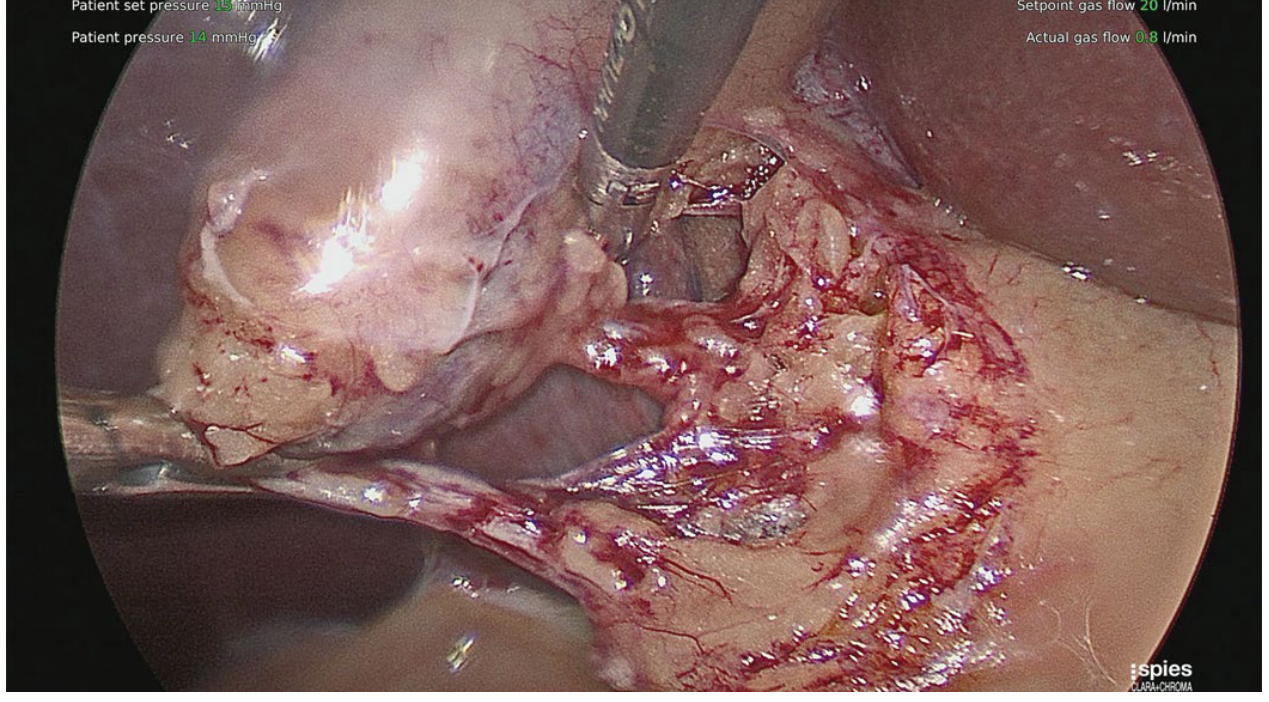
Critical view of safety: exactly two and only two structures entering the gallbladder (cystic duct and cystic artery). - Sabiston Textbook of Surgery, p. 1839
CVS requires all three of the following:
- Two and only two structures entering the gallbladder (cystic duct + cystic artery)
- Lower one-third of the gallbladder dissected off the liver (cystic plate visible)
- Hepatocystic triangle completely cleared of fat and fibrous tissue
Calot's node (lymph node of Calot): A lymph node overlying the cystic artery is a useful landmark. Limiting peritoneal division to the gallbladder side of this node helps minimize CBD injury risk.
3. Clipping and Division
- Clips applied to the cystic duct and cystic artery
- Both structures transected between clips
- Gallbladder dissected off the liver bed using electrocautery
- Venous drainage from gallbladder is directly into the liver bed - excellent hemostasis required
4. Specimen Extraction
- Gallbladder brought out through the umbilical port via a specimen retrieval bag
- Any spilled stones must be retrieved to prevent late perihepatic abscess formation
Intraoperative Cholangiography (IOC)
Not routinely recommended by the Tokyo Guidelines, but selectively indicated when:
- Anatomy is unclear or anomalous
- Suspected choledocholithiasis
- Gallstone pancreatitis (to confirm CBD clearance before ERCP)
Technique: A catheter is passed into the cystic duct via ductotomy; water-soluble contrast injected to opacify the biliary tree. Identifies CBD stones, anomalous anatomy, and guides biliary reconstruction.
Fluorescence Cholangiography (ICG): Indocyanine green (ICG) given IV 2-4 hours before surgery (peak biliary excretion). ICG binds plasma proteins, is taken up by hepatocytes, and excreted into bile. Under near-infrared (NIR) light, it fluoresces green and provides real-time dynamic mapping of extrahepatic biliary anatomy. No radiation required. Safe in pregnancy. Anaphylaxis rate: 0.003%. Early data suggest reduced operative time and conversion to open surgery. - Sabiston Textbook of Surgery, p. 1840
Advantages vs. Open Cholecystectomy
| Advantages of LC | Disadvantages of LC |
|---|---|
| Less postoperative pain | No 3D depth perception (2D monocular view) |
| Smaller incisions | Reduced haptic (tactile) feedback |
| Better cosmesis | Adhesions/inflammation limit use |
| Shorter hospitalization (same-day or 1-day) | More difficult hemorrhage control |
| Earlier return to full activity | CO₂ insufflation complications |
| Lower total cost | Slightly higher bile duct injury rate |
- Maingot's Abdominal Operations, p. 1016
Special Considerations
Acute Cholecystitis
- LC is preferred; higher conversion rate but safe when performed by experienced surgeons
- Inflamed, distended gallbladder: decompress with laparoscopic needle-aspirator or 14G angiocatheter before grasping
- Claw/rat-tooth graspers useful when routine graspers fail
- Dome-down (fundus-first) approach may be needed when infundibular dissection is too dangerous
- ICG fluorescence cholangiography helps when tissue thickness is a concern, though penetration may be limited by inflammation
Conversion to Open
- Not a complication - it is sound surgical judgment
- Indications: unclear anatomy, massive hemorrhage, major bile duct injury, failure to progress
- Rate: approximately 5% overall; higher in acute cholecystitis
Pregnancy (2nd trimester preferred)
- Insufflation pressure limited to <12 mmHg (prevent fetal hypoxia and reduced venous return)
- Maternal hyperventilation with end-tidal CO₂ monitoring to prevent fetal acidosis
- Fetal heart monitoring perioperatively
- Use laparoscopic ultrasound instead of cholangiogram (limit radiation)
- Open port insertion to avoid uterine injury
Laparoscopic Common Bile Duct Exploration (LCBDE)
- Two approaches: transcystic and choledochotomy
- One-stage management (LCBDE + LC) vs. two-stage (ERCP + LC): equivalent stone clearance but one-stage has lower LOS, cost, and pancreatitis rates
- ERCP utilization has risen dramatically, with declining CBDE experience among trainees
Complications
Procedure-Specific
| Complication | Notes |
|---|---|
| Bile duct injury | Most significant; rate ~0.4% (vs. ~0.2% open). Classic mechanism: CBD mistaken for cystic duct due to infundibular traction aligning them. Misidentification risk factors: short cystic duct, large Hartmann's pouch stone, dense inflammation. If recognized intraoperatively: primary repair ± T-tube; complete transection: end-to-end rarely advised - hepaticojejunostomy preferred |
| Bile leak | From cystic duct stump or aberrant duct of Luschka; managed with ERCP and stenting |
| Hemorrhage | Cystic artery, liver bed; trocar-related abdominal wall bleeding |
| Retained CBD stones | Detected on postoperative cholangiogram; managed with ERCP |
| Wound infection / incisional hernia | Port sites |
| Dropped stones | Must retrieve intraoperatively; late perihepatic abscess risk |
Most serious complications occur early in the surgeon's experience. In one multivariate analysis of 8,839 LCs with 15 bile duct injuries, the predicted risk was 1.7% at case 1 vs. 0.17% at case 50 - highlighting the steep learning curve. - Maingot's Abdominal Operations
Pneumoperitoneum-Related
| Complication | Mechanism |
|---|---|
| CO₂ embolism | Intravascular CO₂ entry |
| Vasovagal reflex | Peritoneal stretch |
| Cardiac arrhythmias | Hypercarbia, vagal stimulation |
| Hypercarbic acidosis | Impaired CO₂ exchange (especially in COPD) |
| Reduced venous return | Elevated intra-abdominal pressure compressing IVC |
Trocar-Related
- Abdominal wall hematoma (visualize each trocar site before removal)
- Visceral injury (bowel, bladder - especially in closed insertion near adhesions)
- Major vascular injury (aorta, IVC, iliac vessels - leave trocar in situ if major vessel injury suspected, do NOT remove before open control)
Outcomes
- Mortality: 0.1-0.5%
- Morbidity: 2-3%
- Conversion rate: ~5% elective; higher in acute cholecystitis, previous upper abdominal surgery
- Hospital stay: Same-day or 1-day for elective cases
- Return to full activity: Within a few days
Sources: Sabiston Textbook of Surgery (21st/22nd ed.); Maingot's Abdominal Operations; Current Surgical Therapy 14e; Bailey and Love's Short Practice of Surgery 28th ed.
This is a shared conversation. Sign in to Orris to start your own chat.