Examination of Haemorrhoids
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content from the textbooks and all the key images. Here is the full structured answer:
Examination of Haemorrhoids
Background
Haemorrhoids (piles) are symptomatic enlargements of the internal haemorrhoidal venous plexus (from the Greek: haima = blood, rhos = flowing). They characteristically occur at the 3, 7, and 11 o'clock positions (with the patient in the lithotomy position). Secondary haemorrhoids may develop between these primary positions. External haemorrhoids relate to venous channels of the inferior haemorrhoidal plexus deep in the skin surrounding the anal verge, and are frequently confused with anal skin tags (which are not true haemorrhoids).
Grading (Degrees) of Internal Haemorrhoids
| Degree | Description |
|---|---|
| 1st degree | Bleed only - no prolapse. Hypertrophied plexus remains entirely within the anal canal |
| 2nd degree | Prolapse during defaecation but reduce spontaneously |
| 3rd degree | Prolapse but must be manually reduced |
| 4th degree | Permanently prolapsed, cannot be reduced |
"Mixed" haemorrhoids (3rd/4th degree) have a significant cutaneous component with repeated congestion and oedema.
Clinical Symptoms
- Bleeding - the earliest symptom; bright red, painless, separate from the stool; seen on toilet paper or as a fresh "splash in the pan"
- Prolapse - lump appearing at the anal orifice (2nd-4th degree)
- Pruritus - from mucous discharge
- Mucous discharge - common with prolapsed haemorrhoids
- Pain - NOT typical of uncomplicated haemorrhoids; pain should alert to another diagnosis such as anal fissure or thrombosis
- Anaemia - with chronic significant bleeding (3rd-4th degree)
Examination Setup
Careful clinical examination will be diagnostic in the vast majority of patients, but requires:
- A relaxed, informed patient
- A private environment with a chaperone
- Good light
- Personal protective equipment
Positions for Examination
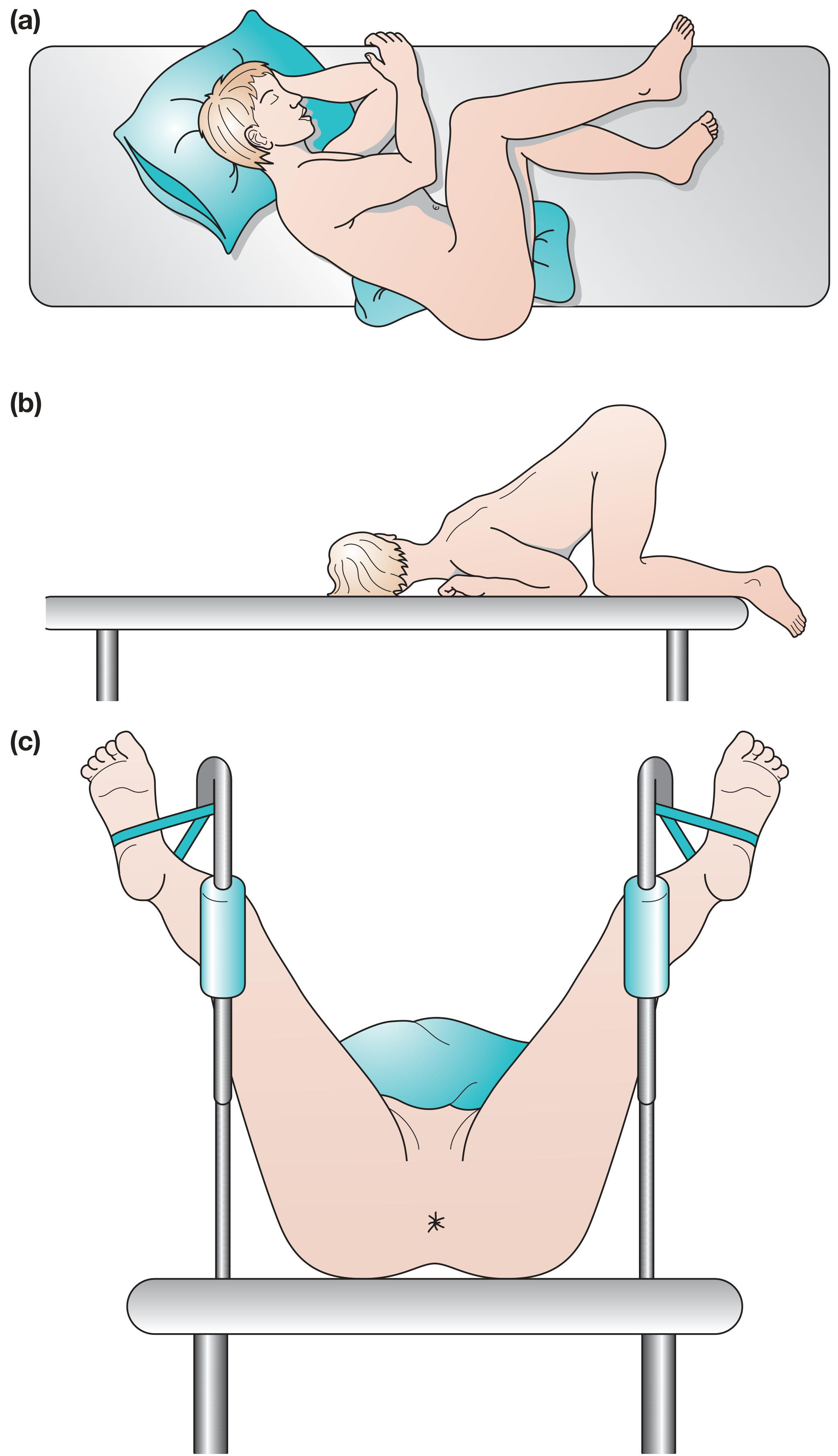
Figure: (a) Left lateral (Sims) position - most common; (b) knee-elbow position; (c) lithotomy position with legs in stirrups.
The left lateral (Sims) position is most commonly used, with the patient's buttocks overlying the edge of the couch. In younger patients, the prone jack-knife or knee-elbow positions may be used.
Step 1: General Examination
Before the local examination, general examination aims to identify predisposing causes of raised intra-abdominal pressure:
- Constipation
- Pregnancy (venous compression + excess progesterone relaxing vessel walls)
- Urethral stricture, enlarged prostate, pelvic tumours (pressing on superior rectal veins)
- Evidence of anaemia (with prolonged bleeding)
Step 2: Local Inspection
The buttocks are gently parted to inspect the anus and perineum, looking for:
| Finding | Significance |
|---|---|
| Skin lesions (e.g. psoriasis, lichen planus, warts, HSV vesicles) | May be confined to perineum or suggest systemic condition |
| Evidence of anal leakage / soiling | Suggests sphincter weakness or prolapse |
| Patulous anus vs. closed anus | Tone assessment |
| Bearing down / straining | May reveal prolapsing haemorrhoids or even rectal prolapse |
| Sentinel tag + pain on parting buttocks | Suggests underlying anal fissure |
| Protruding haemorrhoids at rest | 4th degree |

Figure 80.20 from Bailey & Love: 'Mixed' haemorrhoids; third-degree internal haemorrhoids become visible when the patient strains.
Step 3: Digital Rectal Examination (DRE)
Important point: Uncomplicated internal haemorrhoids cannot be felt on DRE because they are soft and compressible. Digital examination is NOT diagnostic for haemorrhoids unless they are thrombosed or fibrosed.
What DRE does assess:
- Soft tissue induration and tenderness around the anus
- Perianal subcutaneous lesions
- Intrarectal or intra-anal mass
- Sphincter length, resting tone, and voluntary squeeze
- In males: posterior surface of the prostate (anterior wall)
- In females: uterine cervix (anterior wall)
- Puborectalis sling felt posteriorly at the apex of the canal
- Stool colour, blood, mucus, or pus on the withdrawing finger
Step 4: Proctoscopy - The Key Investigation
Haemorrhoids are primarily diagnosed by proctoscopy. This is the essential tool.
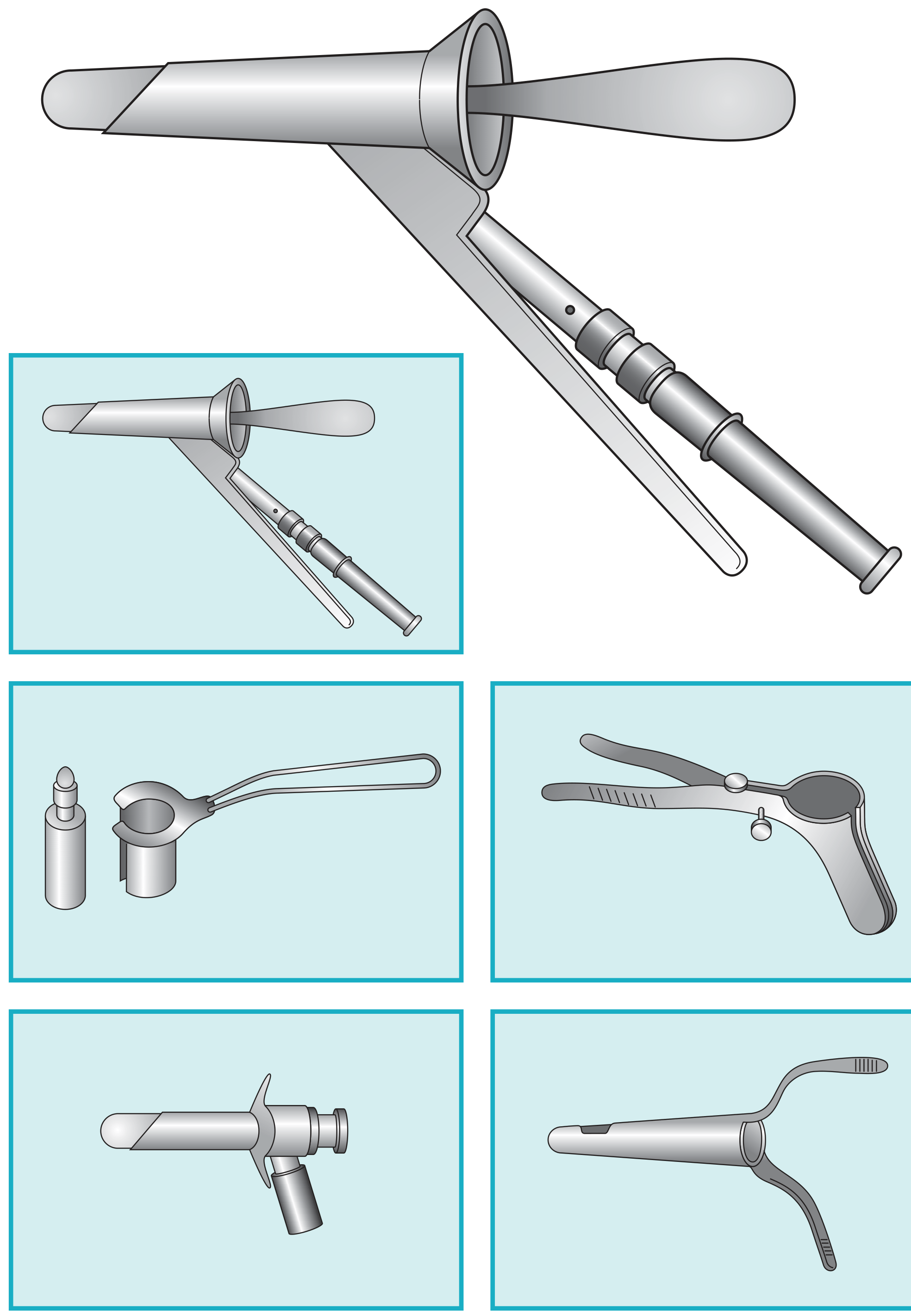
Figure 80.4 from Bailey & Love: Various types of proctoscope.
Technique:
- Fully introduce the proctoscope with the obturator in place
- Remove the obturator under good light
- Slowly withdraw the proctoscope
- The red-brown mucosa with the haemorrhoids will bulge into the proctoscope as it is withdrawn
- The three primary piles are visible at 3, 7, and 11 o'clock (lithotomy position)
- Ask the patient to bear down on slow withdrawal - may reveal a descending intussusception
Proctoscopy also allows minor procedures through the instrument: injection sclerotherapy, rubber band ligation, and biopsy.
Step 5: Sigmoidoscopy
Sigmoidoscopy (rigid or flexible) should always be performed alongside proctoscopy because:
- Rectal pathology is frequently associated with anal lesions
- It is mandatory to exclude serious proximal pathology - particularly carcinoma of the rectum
- Any doubt about the origin of rectal bleeding warrants further investigation (colonoscopy or barium enema)
If there is any doubt about the diagnosis of haemorrhoids, examination under anaesthesia and/or endoscopic visualisation are necessary.
Summary of Examination Steps
- General examination - identify predisposing causes (constipation, pregnancy, prostate, pelvic mass)
- Position the patient - left lateral (Sims) position most commonly
- Inspection - buttocks parted; look for prolapse, skin tags, skin lesions, fistulae, sentinel pile
- Digital rectal examination - assess tone, masses, tenderness; note that uncomplicated piles are impalpable
- Proctoscopy - definitive diagnosis; haemorrhoids bulge into scope on withdrawal at 3, 7, 11 o'clock
- Sigmoidoscopy - mandatory to exclude rectal carcinoma and other proximal pathology
Key Clinical Reminders
- "If you don't put your finger in, you might put your foot in it" - DRE is essential for any patient with anorectal/bowel symptoms (Bailey & Love)
- Bright-red painless bleeding is characteristic; pain should always raise suspicion of a concurrent diagnosis (fissure, thrombosis, carcinoma)
- Symptomless haemorrhoids should not be treated
- Symptoms spontaneously come and go; reassure the patient after full examination and address constipation
- Always exclude colorectal malignancy before attributing bleeding to haemorrhoids
Sources: Bailey and Love's Short Practice of Surgery, 28th Edition, Ch. 80; S. Das - A Manual on Clinical Surgery, 13th Edition, Ch. 4; 22nd Edition Pye's Surgical Handicraft
Examination of liposarcoma
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full answer.
Examination of Liposarcoma
What is Liposarcoma?
Liposarcoma is a malignant tumour with adipocytic differentiation and is the most common soft tissue sarcoma of adulthood (second most common in some orthopaedic series). It occurs predominantly in people in their 50s-60s, arising in the deep soft tissues and retroperitoneum. Three distinct histological subtypes exist, each with different genetics, behaviour, and prognosis.
Subtypes at a Glance
| Subtype | Location | Genetics | Behaviour |
|---|---|---|---|
| Well-differentiated (ALT/WDL) | Deep extremity, retroperitoneum | MDM2 amplification (12q13-q15) | Indolent; excellent prognosis if resected; retroperitoneal WDL frequently recurs |
| Myxoid liposarcoma | Thigh, lower extremity | t(12;16) fusion gene | Intermediate; metastasises to soft tissue (retroperitoneum, extremities) |
| Pleomorphic liposarcoma | Extremities | Complex karyotype | Aggressive; frequent metastases |
| Dedifferentiated liposarcoma | Retroperitoneum | MDM2 amplification + high-grade component | High-grade; risk of dedifferentiation highest in retroperitoneum |
(ALT = Atypical Lipomatous Tumour; WDL = Well-Differentiated Liposarcoma - histologically identical but differ by anatomic location and clinical outcome)
Clinical Presentation
The classic presentation is a large, painless, deep-seated mass located proximally in the extremities (most commonly the thigh) in a patient over 50 years old. Key features:
- Asymptomatic mass - the most common presentation; often noticed incidentally or after minor trauma draws attention to a pre-existing lesion
- Size: tumours in distal extremities tend to be smaller at presentation; proximal extremity and retroperitoneal tumours can grow very large before becoming apparent
- Retroperitoneal liposarcoma: typically presents as a mass >10 cm; symptoms arise late when the tumour compresses surrounding structures - pain, early satiety, obstructive GI symptoms, or neurological symptoms from lumbar/pelvic nerve compression
- Pain: occurs with impingement on bone or neurovascular bundles; more typical of high-grade or large tumours
- Tumour growth: centrifugal - compresses but initially does not invade surrounding normal structures
- Lower extremity DVT may occasionally be the presenting feature (tumour compressing venous outflow)
History Taking
A thorough history should document:
| Parameter | Detail |
|---|---|
| Location | Extremity vs. truncal vs. retroperitoneal |
| Time frame | How long the mass has been present; rate of growth |
| Size change | Enlarging masses are more concerning |
| Pain | Noncyclical pain raises suspicion for malignancy |
| Bowel/urinary symptoms | Compression effects in retroperitoneal disease |
| Family history | Li-Fraumeni syndrome (p53 mutation), Neurofibromatosis Type 1 (3-15% lifetime risk of malignant tumours including MPNST) |
| Previous cancer | Prior history raises concern for metastasis to abdominal wall |
| Prior surgery/radiation | Radiation-induced sarcoma; port-site recurrence after laparoscopy (<1% risk) |
Physical Examination
General Examination
- Overall appearance: look for signs of anaemia (chronic bleeding retroperitoneally), weight loss, cachexia
- Lymph nodes: a complete nodal examination of all nodal basins is mandatory - though lymph node metastasis is rare in liposarcoma (<5% of soft tissue sarcomas overall), it must be excluded
- Testicular examination in men: retroperitoneal mass differential includes testicular primaries (germ cell tumours) - elevated AFP/beta-HCG should be checked
Local Examination of the Mass
The physical examination should systematically document:
| Parameter | Findings and Significance |
|---|---|
| Location | Anatomic site; superficial vs. deep to fascia |
| Size | Measured in three dimensions; >5 cm is high-risk |
| Depth | Superficial (above investing fascia) vs. deep (below fascia) - deep lesions are higher grade |
| Consistency | Soft and fluctuant (lipomatous) vs. firm/hard (dedifferentiated or pleomorphic) |
| Mobility | Mobile vs. fixed - fixation to underlying bone, neurovascular bundles, or overlying skin suggests invasion |
| Surface | Smooth vs. lobulated |
| Tenderness | Pain on palpation - suggests high-grade or rapidly enlarging tumour |
| Skin involvement | Overlying skin changes, induration, ulceration (rare) |
| Transillumination | Liposarcoma does NOT transilluminate (unlike lipoma which may partially do so) |
| Regional neurovascular status | Assess distal pulses, sensation, and motor function for neurovascular compromise |
A key clinical rule: any soft tissue mass that is >5 cm, deep to the fascia, or enlarging must be evaluated with imaging and biopsy - it should NOT be assumed benign.
"Enlarging masses and masses larger than 5 cm or deep to the fascia should be evaluated with a history, imaging, and biopsy." - Schwartz's Principles of Surgery, 11th Ed.
Distinguishing Features from Lipoma (Differential)
Lipoma is 100 times more common than sarcoma. Clinical features that raise suspicion for liposarcoma over lipoma:
- Deep location (beneath investing fascia)
- Size >5-10 cm
- Firmness or heterogeneity on palpation
- Fixed or non-mobile
- Rapid growth
- Pain (lipomas are typically painless)
- Age >50 years with retroperitoneal location
Investigations
Imaging
MRI is the preferred modality for extremity soft tissue sarcomas:
- Shows fat signal in well-differentiated subtypes
- Features favouring malignancy over a benign lipoma:
- Size >10 cm
- Thick, nodular septa
- Globular or nodular non-adipose areas
- Fat content <75%
- Septal enhancement on contrast
- Incomplete fat suppression
CT is preferred for retroperitoneal, intra-abdominal, and truncal sarcomas; can often distinguish WDL from dedifferentiated liposarcoma.
Chest CT for lung metastasis staging in:
- High-grade tumours >5 cm
- Myxoid liposarcoma (also CT abdomen/pelvis - metastasises to soft tissues)
Well-differentiated liposarcoma can be diagnosed by CT imaging alone - negative biopsy should not delay operative intervention if CT is diagnostic.
Histopathology
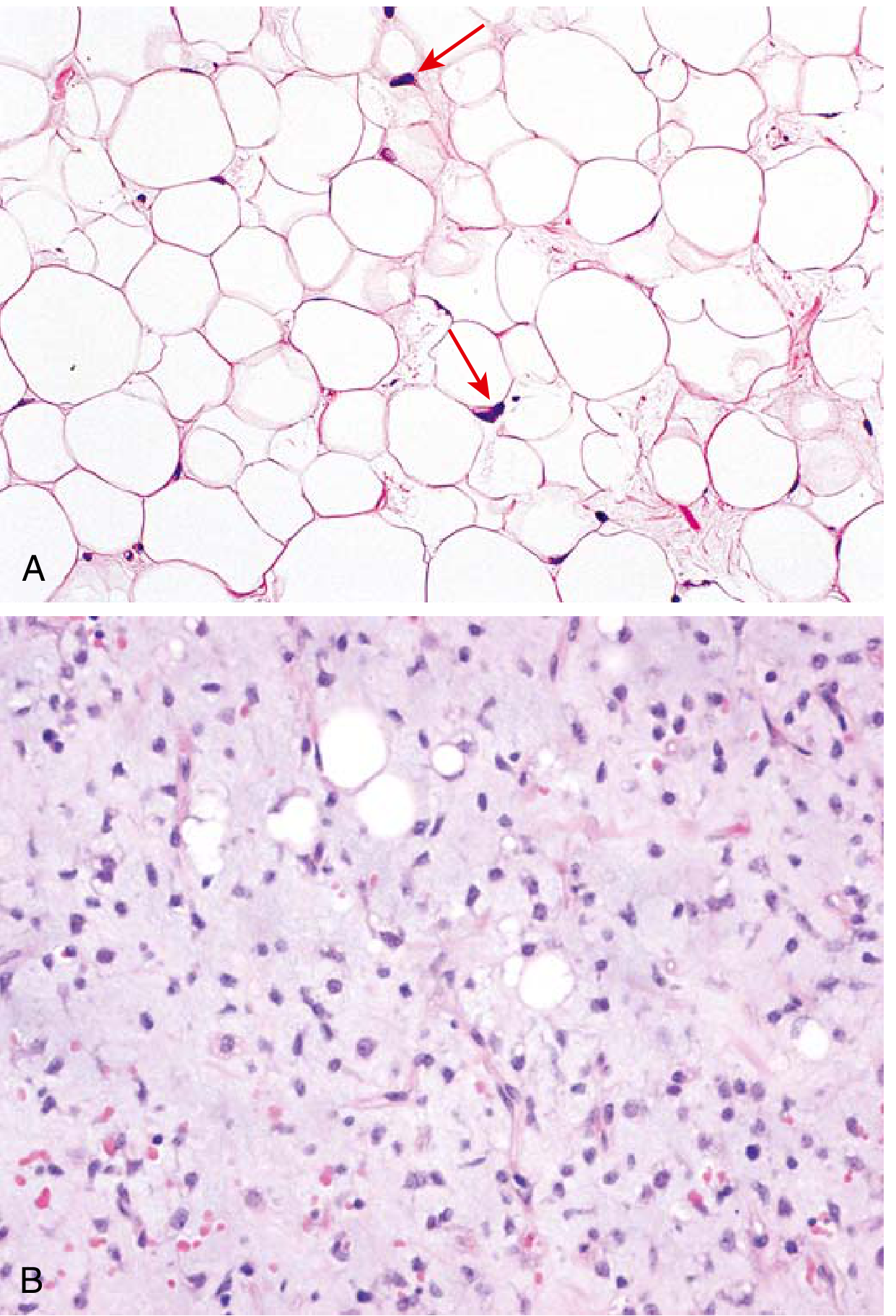
Fig. 19.43 - Robbins & Kumar Basic Pathology: (A) Well-differentiated liposarcoma - mature adipocytes with rare atypical stromal cells; (B) Myxoid liposarcoma - myxoid matrix, arborising "chicken wire" capillaries, and scattered lipoblasts.
Sarcoma is diagnosed by morphologic assessment of histologic sections by an experienced sarcoma pathologist. Even expert pathologists disagree on subtype and grade in 25-40% of cases, highlighting the need for a specialist sarcoma centre.
Ancillary techniques:
- Immunohistochemistry (MDM2, CDK4 for WDL/dedifferentiated)
- Conventional cytogenetics
- FISH for MDM2 amplification (12q13-q15)
- PCR for t(12;16) in myxoid liposarcoma
Biopsy
- Core needle biopsy - preferred for extremity and truncal lesions; performed by the operating surgeon at a sarcoma centre; incision oriented longitudinally along the extremity
- Incisional biopsy - for lesions where core needle is inadequate
- Excisional biopsy - only for superficial lesions <3 cm
- FNA - generally inadequate; only at institutions with specialist cytopathology expertise
- Important: diagnostic imaging should be performed before biopsy to avoid swelling/haemorrhage artefact
Pathological Staging (AJCC)
Soft tissue sarcoma staging includes:
- Histologic grade (most important prognostic factor)
- Tumour size (≤5 cm vs. >5 cm; retroperitoneal: most are >10 cm at diagnosis)
- Depth (superficial vs. deep)
- Nodal/distant metastasis
Poor prognostic indicators: high grade, large size (>5 cm), deep/proximal location, presence of metastasis.
Complications of Liposarcoma
| Complication | Notes |
|---|---|
| Local recurrence | Most common cause of treatment failure, especially retroperitoneal WDL |
| Lung metastases | Primary haematogenous spread (especially high-grade) |
| Soft tissue metastases | Unique to myxoid liposarcoma (retroperitoneum, contralateral extremity) |
| Dedifferentiation | WDL in the retroperitoneum may transform to high-grade dedifferentiated liposarcoma (up to 10%) |
| Portal pyaemia | Rare |
Summary: Examination Checklist
- History - duration, growth rate, pain, systemic symptoms, family/cancer history
- General - anaemia, weight loss, lymphadenopathy, testicular exam (in men with retroperitoneal mass)
- Local mass - site, size, depth, consistency, mobility, skin involvement, neurovascular status
- Imaging before biopsy - MRI for extremity; CT for retroperitoneal
- Core needle biopsy at a sarcoma centre, longitudinal incision
- Chest CT for staging (high-grade or >5 cm)
- Staging workup - CT chest/abdomen/pelvis for myxoid liposarcoma specifically
- Multidisciplinary team - radiologist, pathologist, surgical oncologist, medical and radiation oncologist
Sources: Schwartz's Principles of Surgery 11th Edition, Ch. 36; Campbell's Operative Orthopaedics 15th Ed 2026, Ch. 30; Robbins & Kumar Basic Pathology; Grainger & Allison's Diagnostic Radiology; Fischer's Mastery of Surgery 8th Ed
Examination of Abdomen
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from all three textbooks. Let me compile the full, structured answer.
Examination of the Abdomen
Setup and Patient Position
Before any local examination, perform a detailed general examination of the patient as a whole. The sequence is: Inspection → Palpation → Percussion → Auscultation - followed by examination of hernial orifices, digital rectal examination (DRE), and vaginal examination in females.
Patient position:
- Lie flat on the back, hips and knees extended (or slightly flexed to relax abdominal muscles during palpation)
- Expose the abdomen from the nipples above to the saphenous openings below (including inguinal and femoral rings)
- Examine in good light (preferably daylight)
- Warm hands before examining; gain the patient's confidence
General Examination (Before Local Exam)
The abdomen is examined in the context of the whole patient. Look for:
| System | Findings |
|---|---|
| Hands | Leukonychia, palmar erythema, clubbing, asterixis - signs of chronic liver disease; koilonychia / pallor - anaemia |
| Face / sclera | Jaundice, anaemia, xanthelasma, parotid enlargement |
| Neck | Left supraclavicular lymphadenopathy (Virchow's node / Troisier's sign) - secondary involvement in carcinoma of stomach, pancreas, colon, testis, or breast |
| Vital signs | Heart rate, blood pressure, respiratory rate, temperature, weight, BMI |
| General | Weight loss, dehydration, pedal oedema, abnormal pigmentation, cachexia |
Regions of the Abdomen
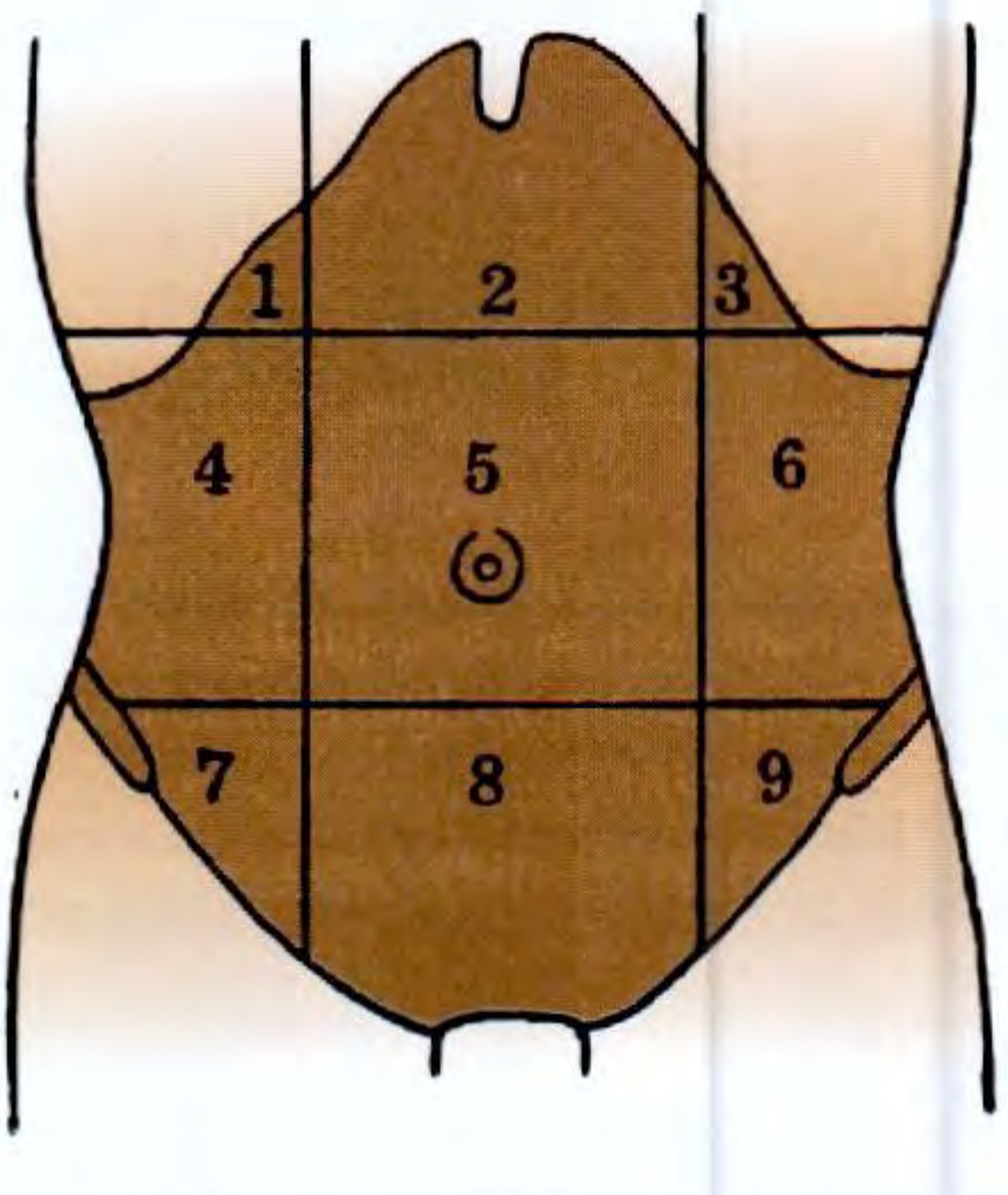
Fig. 35.1 - S. Das: The abdomen divided into nine regions. (1) Right hypochondrium, (2) Epigastrium, (3) Left hypochondrium, (4) Right lumbar, (5) Umbilical region, (6) Left lumbar, (7) Right iliac fossa, (8) Hypogastrium, (9) Left iliac fossa.
Alternatively, a simpler 4-quadrant system (right/left upper and lower quadrants) may be used clinically.
1. INSPECTION
The examiner's eye should be at the level of the patient's abdominal wall (crouch or sit) to detect subtle masses, pulsations, and peristalsis.
A. Hernial Orifices
- Inspect first - inguinal, femoral, umbilical, and incisional hernia sites
- Ask the patient to cough to detect an impulse (positive = hernia)
- "If this examination be left for the last it may be missed and actual cause of acute abdomen may thus remain in the dark" - S. Das
B. Contour of the Abdomen
| Contour | Significance |
|---|---|
| Central distension | Small bowel obstruction |
| Peripheral distension | Large bowel obstruction |
| Scaphoid (sunken) | Diffuse peritonitis (protective rectus contraction), dehydration, cachexia |
| Uniform generalized distension | Ascites, obesity, gaseous distension, late peritonitis |
| Localised bulge | Organomegaly, abdominal wall hernia or abscess |
| Volvulus | Rapid central distension (sigmoid or caecal volvulus) |
5 F's of abdominal distension: Fat, Fluid (ascites), Flatus (gas), Faeces, Fetus (pregnancy)
C. Respiratory Movement
- Normal: abdomen rises and falls freely with respiration
- Absent or sluggish: widespread peritoneal irritation - diffuse peritonitis (peptic perforation, haemorrhage from ruptured ectopic gestation)
- Localised limitation: localized peritonitis (acute cholecystitis, appendicitis)
D. Visible Peristalsis
- Watch patiently for a few moments
- "Ladder pattern" - small bowel obstruction
- Left-to-right wave from left hypochondrium - pyloric obstruction / gastric carcinoma
- Right-to-left wave - transverse colon carcinoma
E. Pulsating Swelling
- Visible pulsation in epigastrium - abdominal aortic aneurysm (leaking or intact)
F. Skin
| Sign | Location | Cause |
|---|---|---|
| Grey Turner's sign | Flanks (bluish-grey discolouration) | Retroperitoneal haemorrhage - severe acute pancreatitis, leaking AAA |
| Cullen's sign | Periumbilical bluish discolouration | Severe acute haemorrhagic pancreatitis, ruptured ectopic gestation, liver trauma (blood tracks along ligamentum teres) |
| Redness / blisters | Site of pain | Hot application; suggests localised inflammation |

Figure 63.3 - Bailey & Love: Cullen's sign of periumbilical skin discolouration (and Grey Turner's sign of flank discolouration) in severe acute pancreatitis.
G. Scars
- Previous surgical scars indicate prior operations; their size and location suggest the nature of previous surgery
- Striae (stretch marks) - pregnancy, obesity, Cushing's syndrome
H. Dilated Veins
- Caput medusae (periumbilical radiating veins) - portal hypertension with recanalization of umbilical vein
- Flow direction: in portal hypertension, flow is away from umbilicus; in IVC obstruction, flow is upward above umbilicus and downward below
- Scrotum inspection - always inspect; testicular malignancy metastasizes to para-aortic nodes (swelling here may be the first presentation)
2. PALPATION
Technique
- Use the volar surfaces (flexor surfaces) of the fingers - never poke with fingertips held vertical
- Forearm kept horizontal at the level of the abdomen
- Hand movement at metacarpophalangeal joints only; not at interphalangeal joints
- Begin superficial palpation, then deep palpation (if tenderness allows)
- Start furthest from the site of pain and work towards it
- Watch the patient's face throughout for signs of discomfort
- For palpation: hips and knees flexed to relax abdominal muscles
- Ask patient to breathe through the mouth slowly to reduce voluntary guarding
A. Tenderness
- Note: site, severity, and radiation of tenderness
- McBurney's point (1/3 of the way from ASIS to umbilicus) - appendicitis
- Murphy's sign: palpate under the right costal margin during deep inspiration; the patient catches their breath or winces due to the inflamed gallbladder descending onto the examining fingers - indicates acute cholecystitis
- Rovsing's sign: pressure on the left iliac fossa produces pain in the right iliac fossa - acute appendicitis (coils of ileum shift slightly to the right, pressing on the inflamed appendix)
- Cope's Psoas test: a retrocaecal appendix lies on psoas major; passive extension of the hip (with patient in left lateral position) stretches psoas and causes pain - retrocaecal appendicitis
- Obturator test: internal rotation of a flexed hip causes pain in RIF - pelvic appendicitis
B. Guarding and Rigidity
Voluntary guarding - patient tenses muscles consciously to avoid pain; disappears during expiration; present throughout the abdomenInvoluntary guarding (muscle guard) - reflex spasm of overlying abdominal wall when inflamed viscus touches parietal peritoneum; remains during expiration; localized to the area of pathology
| Pattern | Significance |
|---|---|
| Involuntary guarding (upper right rectus) | Peptic ulcer perforation |
| Involuntary guarding (right iliac fossa) | Paracaecal appendicitis |
| Involuntary guarding (loin) | Retrocaecal appendicitis |
| No abdominal guarding | Pelvic appendicitis, all colics, obstruction without strangulation |
| Board-like rigidity (whole abdomen) | Generalized peritonitis (late sign - must not let patient reach this stage) |
Differentiation from thoracic disease: In diaphragmatic pleurisy / basal pneumonia, skin may be hyperaesthetic but deep palpation does not elicit true tenderness; Rovsing's sign is negative; rigidity diminishes on expiration.
C. Rebound Tenderness (Blumberg's/Release sign)
- Press gradually with each expiration → then suddenly and completely withdraw the hand
- Patient cries out or winces - sign of parietal peritoneal inflammation (peritonitis)
- A gentler method: percussion tenderness (patient winces when the abdomen is percussed) - equally sensitive, less painful for the patient
- Pain on coughing also indicates rebound tenderness
- In acute intestinal obstruction, the presence of rebound tenderness suggests strangulation
D. Examining an Abdominal Mass
For any abdominal lump, assess systematically:
| Feature | Details |
|---|---|
| Position | Describe in relation to the nine regions |
| Size | Measured in three dimensions |
| Shape and surface | Regular/irregular; smooth or nodular |
| Margin | Well-defined (neoplasm) vs. ill-defined (inflammatory/traumatic) |
| Consistency | Soft, cystic, firm, hard; variable consistency; fluctuation; fluid thrill in large cysts |
| Tenderness | Indicates inflammatory aetiology |
| Local temperature | Rise = inflammatory swelling |
| Movement with respiration | Liver, gallbladder, spleen, stomach move well; kidney/suprarenal move very little; retroperitoneal masses are fixed |
| Parietal vs. intraperitoneal | Rising test (patient raises shoulders with arms crossed): parietal lumps become more prominent; intraperitoneal lumps disappear. Carnett's test / Leg-lifting test: tense abdominal muscles by lifting straight legs - parietal swellings become more prominent; intraperitoneal ones become impalpable |
| Mobility | Intraperitoneal contact with diaphragm = moves with respiration; retroperitoneal = fixed; enlarged kidney = ballotable and bimanually palpable |
| Expansile pulsation | Characteristic of abdominal aortic aneurysm (normal aorta transmits a non-expansile impulse) |
| Uterine/ovarian mass | Moves transversely |
| Mesenteric cyst | Moves perpendicular to root of mesentery (obliquely - from right iliac fossa to left hypochondrium) |
E. Liver Palpation
- Start in the right lower quadrant and move upward toward the rib cage, so the liver edge is felt on the way up
- Patient takes deep breath - normal liver edge may be felt up to 2 cm below the right costal margin
- Normal edge: smooth, slightly tender on deep inspiration in thin subjects
- Hard, irregular: cirrhosis
- Tender, enlarged, smooth: acute hepatitis (viral, alcoholic), hepatic congestion (right heart failure)
- Scratch test: bell of stethoscope over right upper quadrant; scratch from mid-abdomen upward - sound is amplified over the liver; useful when liver edge is unclear
F. Spleen Palpation
- Healthy spleen is NOT normally palpable
- Enlarged spleen descends downwards, forwards and medially
- Start in right lower abdomen with fingertips pointing upward; move gradually toward the left hypochondrium with each breath
- If not palpable supine, repeat in right lateral position
- Characteristic notch on the medial border distinguishes it from other masses
- Percussion: dullness between 9th and 11th ribs in the left midaxillary line = splenomegaly
G. Kidneys
- Bimanual palpation (ballottement): one hand behind the loin, one hand on anterior abdomen
- Enlarged kidney is ballotable - can be bounced between the two hands
- Moves very little with respiration (unlike spleen/liver)
- Renal angle tenderness: tap over the costovertebral angle (renal angle) - tenderness indicates pyelonephritis or renal pathology
3. PERCUSSION
- Moves from resonant to dull areas
- Liver span: normally 6-12 cm in the midclavicular line; diminished in cirrhosis; increased in hepatomegaly (right heart failure, NAFLD, cholestatic cirrhosis)
- Liver: dull to percussion
- Gas under diaphragm: loss of liver dullness / hyperresonance in right hypochondrium = pneumoperitoneum (perforated viscus)
- Splenomegaly: dullness between 9th-11th ribs in left midaxillary line
- Tympany: normal bowel/gaseous distension
- Dullness in flanks → Shifting dullness → confirmed by patient rolling to one side; dullness shifts = ascites
- Fluid thrill: tap one flank, feel vibrations transmitted to the other flank (hand of assistant placed on midline to prevent abdominal wall transmission) - large-volume ascites
- Percussion rebound: patient winces when abdomen is gently percussed = underlying peritonitis (more humane than the classical release sign)
4. AUSCULTATION
| Finding | Significance |
|---|---|
| Absent / silent abdomen | Diffuse peritonitis, paralytic ileus - pathognomonic of peritonitis |
| Reduced or absent locally | Localized inflammation of underlying organ |
| High-pitched tinkling / metallic sounds / borborygmi | Mechanical intestinal obstruction |
| Normal clicks and gurgles | Normal peristalsis |
| Succussion splash | Gastric stasis / pyloric obstruction - "shaking a half-filled bottle of water" |
| Aortic bruit | Aortic stenosis / AAA |
| Iliac bruit | Iliac artery stenosis |
| Cardiac / respiratory sounds audible | Complete absence of bowel sounds in peritonitis or paralytic ileus |
A "silent abdomen" is the pathognomonic feature of diffuse peritonitis. A "noisy abdomen" (metallic tinkles) is a feature of mechanical intestinal obstruction.
5. COMPLETION OF ABDOMINAL EXAMINATION
Abdominal examination is not complete until:
- All hernial orifices examined (inguinal, femoral, umbilical, incisional) - with cough impulse
- Digital Rectal Examination (DRE) - mandatory in all acute abdominal cases
- Tenderness in the right wall of rectum = pelvic appendicitis
- Tenderness in rectovesical pouch = perforated peptic ulcer
- Bulging anterior wall of rectum = pelvic abscess
- "Red currant jelly" on gloved finger (blood + mucus, no faecal odour) = intussusception
- Vaginal examination in females (if indicated)
- Tenderness in both fornices + purulent discharge = acute salpingitis
- Soft cervix + cervical excitation pain = ruptured ectopic gestation
- Renal angles - tap for tenderness
- External genitalia - inspect the scrotum routinely (testicular malignancy → para-aortic lymphadenopathy)
- Thoracic and lumbar spine examination
- Vital signs and measurement - note abdominal girth in obstruction/ascites for serial comparison
Key Clinical Reminders
| Sign | Condition |
|---|---|
| Grey Turner's sign | Retroperitoneal haemorrhage (pancreatitis, AAA) |
| Cullen's sign | Periumbilical haemorrhage (haemorrhagic pancreatitis, ruptured ectopic) |
| Murphy's sign | Acute cholecystitis |
| Rovsing's sign | Acute appendicitis |
| Blumberg's (rebound) sign | Peritonitis |
| Troisier's sign | Left supraclavicular node = intra-abdominal malignancy |
| Caput medusae | Portal hypertension |
| Board-like rigidity | Generalized peritonitis (late) |
| Shifting dullness / fluid thrill | Ascites |
| Succussion splash | Gastric outlet obstruction |
| Expansile pulsation | Abdominal aortic aneurysm |
| Ballottement | Enlarged kidney |
Sources: S. Das - A Manual on Clinical Surgery, 13th Edition; Bailey and Love's Short Practice of Surgery, 28th Edition, Ch. 63; Goldman-Cecil Medicine International Edition, Ch. 132
This is a shared conversation. Sign in to Orris to start your own chat.