Intra aortic balloon pump: principles, indications, advantages and disadvantages
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative textbooks with excellent images. Here is the full answer:
Intra-Aortic Balloon Pump (IABP)
Overview
The IABP is the most commonly used mechanical circulatory support (MCS) device. First described by Harken in 1958, it is a percutaneously placed device that sits in the descending thoracic aorta, just distal to the left subclavian artery and proximal to the renal arteries. The catheter is a double-lumen, 7.5- to 8.0-French polyethylene balloon typically inserted via the left femoral artery under fluoroscopic or ultrasound guidance.
Helium gas is used to inflate the balloon because its low viscosity allows rapid transfer in and out, and it absorbs very quickly into blood in the event of balloon rupture.
Principles (Mechanism of Action - Counterpulsation)
The IABP operates on the principle of counterpulsation - it acts opposite to the cardiac cycle:
1. Inflation during diastole (triggered at aortic valve closure / dicrotic notch on the arterial trace, or mid-T-wave on ECG)
- Rapid balloon inflation displaces blood proximally and distally
- Increases diastolic aortic pressure ("diastolic augmentation")
- Increases coronary artery perfusion pressure (since coronary filling occurs in diastole)
- Augments cerebral perfusion
2. Deflation just before systole (triggered at peak R wave on ECG)
- Rapid deflation creates a sudden drop in aortic end-diastolic pressure
- Reduces left ventricular afterload (the LV ejects against less resistance)
- Lowers myocardial oxygen demand (MVO2)
- Modestly augments cardiac output by ~0.5-1.0 L/min
The net effect is a favourable shift in the myocardial oxygen supply-demand balance: more oxygen delivered (via enhanced coronary perfusion) and less consumed (via afterload reduction).
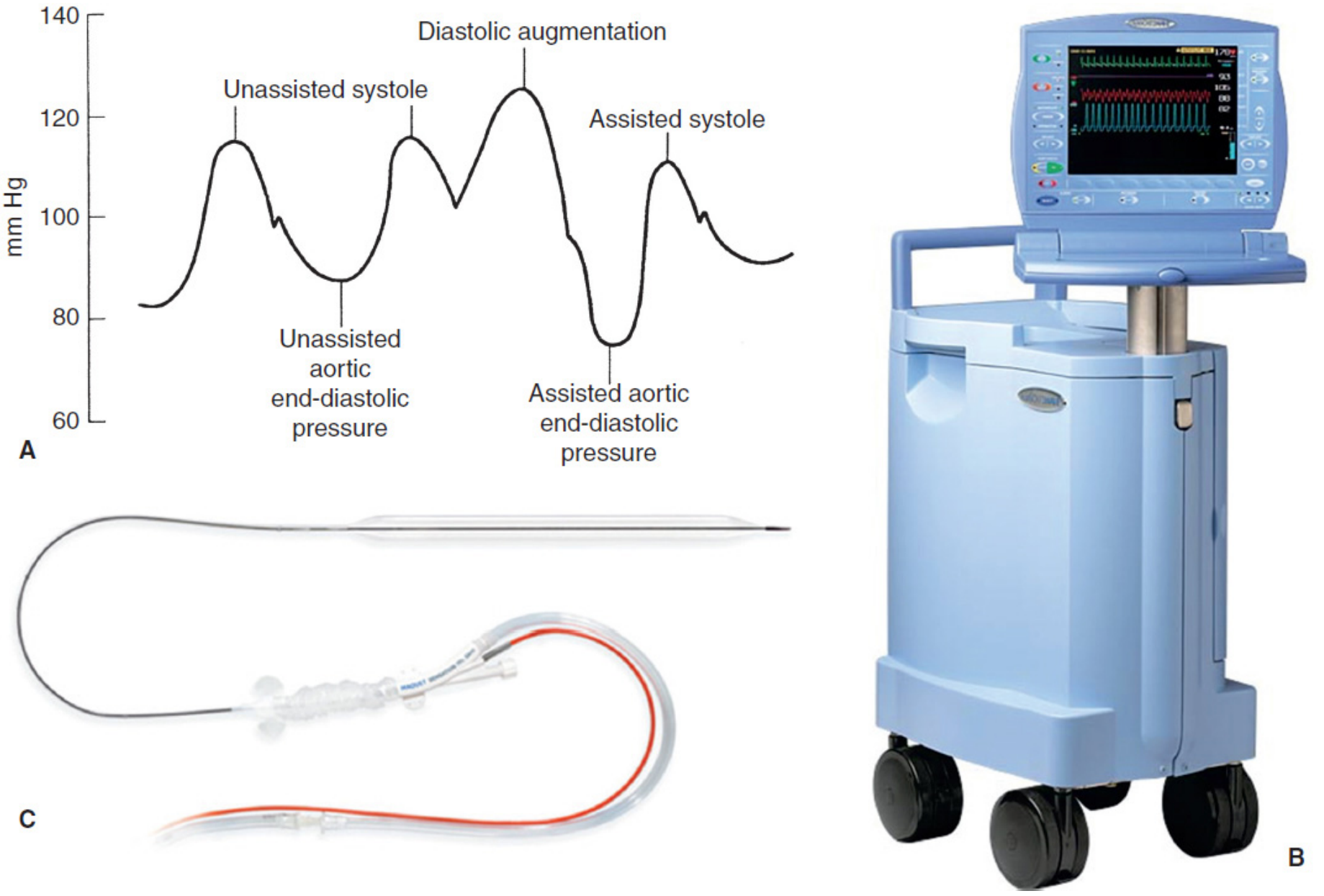
IABP Waveform
The arterial waveform with IABP in place shows the characteristic features of:
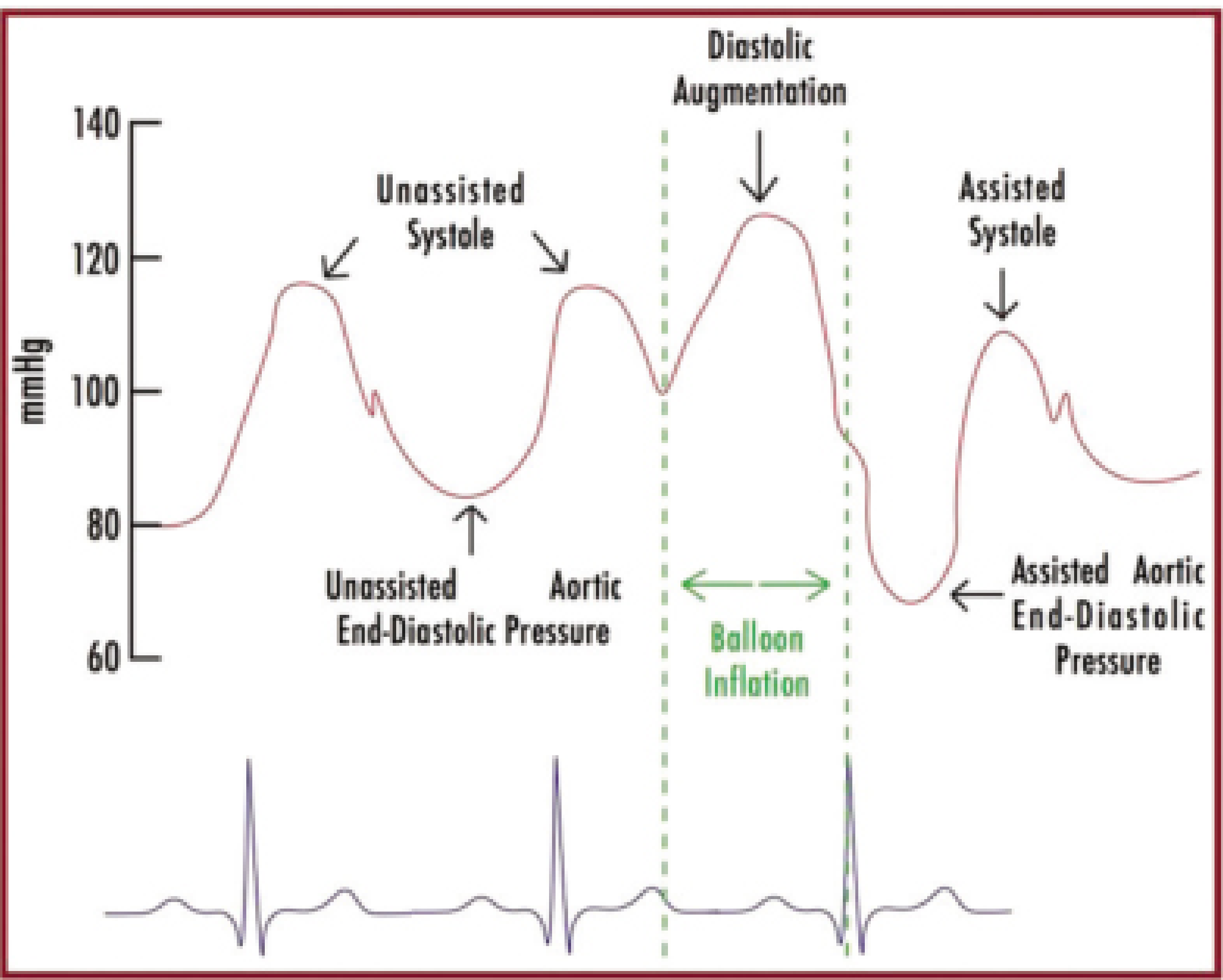
- Unassisted systole - normal peak pressure
- Diastolic augmentation - a prominent spike during the assisted diastole, often exceeding the previous systolic peak
- Assisted aortic end-diastolic pressure - lower than the unassisted end-diastolic pressure (reflects afterload reduction)
- Assisted systole - reduced systolic peak (less work required from LV)
MCS Device Comparison
Hemodynamic Requirements
For the IABP to be effective, the patient must have:
- Some residual LV function - any increase in cardiac output still depends on the work of the heart itself
- Electrical stability - the device is triggered by ECG (R wave) or arterial pressure tracing (dicrotic notch)
Optimal effect also depends on: balloon position, blood displacement volume, balloon-to-aorta diameter ratio, timing precision, and the patient's heart rate, blood pressure, and vascular resistance.
Indications
| Clinical Setting | Details |
|---|---|
| Cardiogenic shock | Post-MI or acute decompensated HF with hypotension; stabilization bridge |
| Acute MI complications | Papillary muscle rupture (acute MR), ventricular septal rupture |
| Pre/post cardiac surgery | Bridge before or support after coronary artery bypass grafting (CABG) |
| High-risk PCI | Prophylactic support during percutaneous coronary intervention |
| Bridge to therapy | Bridge to LVAD, transplant, or recovery |
| Refractory unstable angina | When medical therapy fails, prior to definitive revascularization |
| Thrombolysis in cardiogenic shock | Augments thrombolysis benefit; particularly when PCI is unavailable, used with thrombolytics then transfer |
Contraindications
Absolute:
- Severe aortic regurgitation - balloon inflation in diastole would worsen regurgitant volume back into the LV
- Aortic dissection - balloon inflation could propagate or worsen the dissection
Relative:
- Aortic aneurysm
- Significant coagulopathy
- Severe peripheral arterial disease (especially at the insertion site)
- Severe aortoiliac occlusive disease
- Uncontrolled sepsis
Advantages
| Advantage | Detail |
|---|---|
| Simplicity and speed | Percutaneous insertion; fast to place, available at most centres |
| Afterload reduction | Reduces myocardial O2 consumption without requiring extra energy from the heart |
| Coronary perfusion | Directly augments diastolic coronary filling |
| Hemodynamic improvement | Increases mean arterial pressure and cardiac output modestly |
| Ease of monitoring | Reliable arterial waveform available continuously |
| No oxygenation required | Simpler than ECMO |
| Widely available | Less specialist training than Impella or TandemHeart |
| Removable | Can be weaned and removed percutaneously once no longer needed |
| Low thrombocytopenia | Compared to other MCS devices (Impella, TandemHeart), lower haematological complications |
Disadvantages / Limitations
| Disadvantage | Detail |
|---|---|
| Modest cardiac output support | Only augments CO by ~0.5-1.0 L/min - far less than Impella (up to 4 L/min) or ECMO (2-6 L/min) |
| ECG/rhythm dependence | Requires a consistent cardiac rhythm for proper trigger timing; less effective in tachyarrhythmias, irregular rhythms (AF) |
| LV function requirement | Does not replace LV function; ineffective if the heart has no intrinsic output |
| No oxygenation | Cannot correct hypoxaemia |
| Limb ischaemia | Major limb ischaemia (the most serious vascular complication) from femoral artery occlusion |
| Vascular complications | Bleeding at insertion site, haematoma, pseudoaneurysm, aortic injury |
| Infection | Risk with prolonged use |
| Stroke | Rare but reported (thromboembolic) |
| Thrombocytopenia | Mechanical destruction of platelets, though less severe than Impella/TandemHeart |
| Balloon rupture | Risk of helium embolism (rare, as helium absorbs rapidly) |
| Aortic position issues | Malposition can obstruct the left subclavian artery (too high) or renal arteries (too low) |
| IABALLO SHOCK II data | The landmark IABP-SHOCK II trial (2012) showed no mortality benefit of IABP vs. medical therapy alone in AMI-complicated cardiogenic shock undergoing revascularization (30-day mortality 39.7% vs. 41.3%; RR 0.96; P=0.69), which has shifted guidelines away from routine use in this setting |
Complication Rates (Benchmark Registry)
- Major complications: 2.6%
- All complications combined: 8.1%
The most clinically significant complication is major limb ischaemia, followed by bleeding and infection.
Summary Table: IABP vs. Other MCS Devices
| Feature | IABP | Impella | TandemHeart | VA-ECMO |
|---|---|---|---|---|
| Flow (L/min) | ~0.5-1.0 | 2.5-4.0 | Up to 4.0 | 2-6 |
| Oxygenation | No | No | No | Yes |
| LV support | Indirect (afterload reduction) | Direct | Direct | Biventricular |
| Ease of insertion | Highest | Moderate | Specialist | Specialist |
| Complications | Thrombocytopenia (mild) | Haemolysis, bleeding | Haemolysis, bleeding | Haemolysis, bleeding |
Sources:
- Fischer's Mastery of Surgery, 8th ed., p. 345
- Braunwald's Heart Disease, 12th ed. (Table 59.2)
- Tintinalli's Emergency Medicine, 9th ed.
- Rosen's Emergency Medicine, 9th ed. (Table 66.2)
See send as university exam answer need to be deep enough
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have everything needed for a thorough university exam answer. Here is the full, deep, exam-ready response:
INTRA-AORTIC BALLOON PUMP (IABP)
I. INTRODUCTION
The intra-aortic balloon pump (IABP) is the most widely used mechanical circulatory support (MCS) device in clinical practice. First described by Harken in 1958 and clinically introduced by Kantrowicz in 1967, it provides temporary haemodynamic support through the principle of counterpulsation - augmenting diastolic pressure while simultaneously reducing systolic afterload.
The device consists of:
- A double-lumen, 7.5- to 8.0-French catheter with a polyethylene balloon (volume 30-50 mL for adults) attached at its distal end
- One lumen connects to the pneumatic pump console and drives balloon inflation/deflation
- One lumen allows continuous aortic pressure monitoring
- The pump console, which controls timing via ECG or arterial pressure triggers
Inflation gas: Helium is used exclusively because its low molecular weight and low viscosity allow rapid transfer in and out of the balloon, and it is absorbed rapidly into blood in the event of balloon rupture, minimising the risk of systemic gas embolism.
II. PRINCIPLES OF OPERATION
A. Device Position
The balloon is positioned in the descending thoracic aorta, just distal to the origin of the left subclavian artery and proximal to the renal arteries. This ensures:
- Diastolic augmentation benefits coronary and cerebral perfusion (proximal displacement of blood)
- Deflation reduces LV afterload without occluding major branch vessels
Insertion is most commonly via the left femoral artery (percutaneous Seldinger technique), confirmed by fluoroscopy or intraoperative transesophageal echocardiography. Alternative sites include axillary/subclavian artery (allows patient ambulation) or surgical graft to the ascending aorta when peripheral vascular disease precludes femoral access.
B. The Counterpulsation Cycle
The IABP acts in direct opposition to the normal cardiac cycle:
Phase 1 - Rapid Inflation in Diastole:
- Triggered at: dicrotic notch on the arterial pressure tracing (= aortic valve closure) or mid-T-wave on ECG
- The balloon rapidly inflates, displacing a volume of blood (~40 mL) bidirectionally - proximally toward the coronary ostia and aortic root, distally toward the peripheral circulation
- Effect: Diastolic augmentation - peak diastolic pressure rises, often exceeding the previous systolic pressure
- This markedly increases coronary perfusion pressure (since ~85% of coronary filling occurs in diastole) and augments cerebral blood flow
Phase 2 - Rapid Deflation Before Systole:
- Triggered at: peak R wave on ECG (just before LV contraction)
- Sudden deflation creates a partial vacuum in the aorta
- Effect: Aortic end-diastolic pressure falls (assisted aortic end-diastolic pressure lower than unassisted)
- The LV ejects against reduced resistance (afterload reduction)
- LV wall stress, myocardial oxygen demand (MVO2), and LV end-diastolic pressure all decrease
- Cardiac output augmented by approximately 0.5-1.0 L/min
C. Haemodynamic Effects Summary
| Parameter | Effect of IABP |
|---|---|
| Diastolic blood pressure | Increased (diastolic augmentation) |
| Aortic end-diastolic pressure | Decreased (afterload reduction) |
| LV afterload | Decreased |
| Myocardial O2 consumption (MVO2) | Decreased |
| Coronary perfusion pressure | Increased |
| Cerebral perfusion | Increased |
| Cardiac output | Modestly increased (~0.5-1.0 L/min) |
| LV end-diastolic pressure/volume | Decreased |
| LV wall stress | Decreased |
| Mean arterial pressure | Increased |
The net result is a favourable shift in myocardial O2 supply-demand balance: more supply (increased coronary perfusion) and less demand (afterload reduction).
D. Timing and Trigger Modes
The IABP console accepts two trigger modes:
- ECG trigger - inflation at mid-T-wave; deflation at R-wave peak (most commonly used)
- Arterial pressure trigger - inflation at dicrotic notch; deflation timed to precede next systolic upstroke
Correct timing is critical. Timing errors have defined haemodynamic consequences:
| Error | Waveform sign | Consequence |
|---|---|---|
| Early inflation | Inflation before dicrotic notch | Premature aortic valve closure; increases cardiac work |
| Late inflation | Inflation well after dicrotic notch | Suboptimal diastolic augmentation |
| Early deflation | Assisted aortic end-diastolic pressure rises before next systole | Loss of afterload reduction; no LV offloading |
| Late deflation | Assisted systole peak rises; U-shaped trough before next systole | LV ejects against inflated balloon; markedly increases afterload |
The device is typically set at 1:1 counterpulsation (one balloon cycle per heartbeat). During weaning, ratio is decreased to 1:2 and then 1:3 to assess haemodynamic tolerance before removal.
E. Prerequisite for Effectiveness
Critically, the IABP does not replace cardiac function - it augments it. The patient must have:
- Some residual LV function and forward cardiac output
- A reasonably organised electrical rhythm (less effective in rapid tachyarrhythmias or atrial fibrillation with irregular RR intervals)
- Effective triggers for balloon cycling
III. INDICATIONS
A. Primary Indications
1. Cardiogenic Shock
- Post-acute MI cardiogenic shock (with or without revascularisation)
- Acute decompensated heart failure with hypotension
- Used as a bridge to definitive therapy (PCI, CABG, LVAD, or transplant)
- In hospitals without direct PCI capability: IABP + thrombolysis followed by transfer to a tertiary centre is the best management option
2. Acute MI Mechanical Complications
- Acute papillary muscle rupture causing severe mitral regurgitation
- Post-infarction ventricular septal rupture
- Reduces afterload, decreasing the regurgitant fraction and supporting haemodynamics while awaiting surgical correction
3. High-Risk Percutaneous Coronary Intervention (PCI)
- Prophylactic pre-procedural placement in patients with severely reduced LV function, left main disease, or last remaining vessel
- A meta-analysis of 9 RCTs (n = 1,171) in high-risk CABG patients showed significantly lower mortality and major adverse cardiac and cerebrovascular events (MACCEs) with preemptive IABP vs. controls
4. Perioperative Cardiac Surgery Support
- Pre-operative: high-risk patients before CABG to reduce operative mortality
- Post-operative: failure to wean from cardiopulmonary bypass; post-CABG low cardiac output syndrome
- Bridge while the heart recovers ("rested" on CPB with IABP running)
5. Unstable Angina Refractory to Medical Therapy
- Reduces ischaemic burden while awaiting revascularisation
6. Bridge to Transplant or Permanent LVAD
- Temporary support maintaining end-organ perfusion in terminal heart failure
IV. CONTRAINDICATIONS
Absolute Contraindications
| Condition | Reason |
|---|---|
| Severe aortic regurgitation | Diastolic inflation increases regurgitant volume back into the LV, dramatically worsening LV volume overload and pulmonary oedema |
| Aortic dissection | Balloon inflation can propagate or extend the dissection; direct trauma to the aortic wall |
Relative Contraindications
| Condition | Concern |
|---|---|
| Abdominal aortic aneurysm | Risk of rupture from mechanical stress |
| Severe peripheral arterial disease | Inability to pass catheter; limb ischaemia risk |
| Severe aortoiliac occlusive disease | Access obstruction; risk of limb ischaemia |
| Significant coagulopathy | Haemorrhage at insertion site |
| Severe tachyarrhythmia / irregular rhythm | Inadequate trigger accuracy; reduced efficacy |
| Profound shock / cardiac arrest | Provides only partial support; consider ECMO instead |
| Uncontrolled sepsis | Risk of seeding device |
V. ADVANTAGES
1. Widely Available and Fast to Insert
- Percutaneous insertion via femoral artery; can be placed within minutes at the bedside, in the catheterisation lab, or in the operating theatre
- Available at most cardiac centres without need for specialist surgical support
2. Dual Physiological Benefit
- Simultaneously increases coronary perfusion AND decreases myocardial O2 demand - a uniquely favourable combination not achieved by pharmacological agents alone
- Inotropes increase O2 demand while improving output; vasodilators reduce afterload but may drop coronary perfusion pressure
3. No External Bypass Circuit Required
- Unlike ECMO or TandemHeart, no oxygenator, venous cannula, or priming circuit needed
- Simpler setup and management
4. Continuous Haemodynamic Monitoring
- The arterial lumen provides continuous aortic pressure monitoring
- The waveform pattern is a real-time quality check on timing accuracy
5. Reversible and Easy to Wean
- Support frequency reduced gradually (1:1 → 1:2 → 1:3)
- Device removed percutaneously with manual compression; no surgical closure required
6. Effective LV Offloading in Mechanical Complications
- In papillary muscle rupture or VSD, afterload reduction substantially reduces the regurgitant/shunt fraction, stabilising the patient for surgery
7. Modest Haematological Impact
- Compared to Impella or TandemHeart, IABP causes less haemolysis and thrombocytopenia due to its non-contact, non-rotary mechanism
VI. DISADVANTAGES AND LIMITATIONS
1. Modest Cardiac Output Augmentation
- Increases CO by only ~0.5-1.0 L/min - inadequate for severe biventricular failure
- Compare: Impella provides 2.5-4.0 L/min; ECMO provides 2-6 L/min (full biventricular support)
2. Rhythm Dependence
- Requires a consistent cardiac rhythm for accurate ECG triggering
- In rapid tachyarrhythmias (HR >130 bpm) or irregular rhythms (atrial fibrillation), timing is inaccurate and haemodynamic benefit is substantially reduced
3. Requires Residual LV Function
- Cannot sustain circulation in complete cardiac standstill or severe biventricular failure
- Profound shock or cardiac arrest represents a relative contraindication
4. No Oxygenation
- Does not correct hypoxaemia; patients with combined cardiorespiratory failure require ECMO
5. Vascular Complications
- Limb ischaemia (most serious): femoral artery occlusion; incidence ~3-7%
- Haematoma and bleeding at the insertion site
- Pseudoaneurysm, arteriovenous fistula
- Retroperitoneal haematoma (rare)
6. Malposition Risks
- Too high: may occlude the left subclavian artery
- Too low: may occlude renal arteries or compromise mesenteric flow
7. Systemic Complications
- Stroke (thromboembolic, from aortic plaque disruption)
- Infection (bacteraemia, local insertion-site infection with prolonged use)
- Thrombocytopenia (mechanical platelet destruction)
- Balloon rupture with gas embolism (rare; helium absorbs rapidly)
8. IABP-SHOCK II Trial - Lack of Mortality Benefit in AMI-CS
- The landmark IABP-SHOCK II trial (2012, n=600) - a prospective, randomised, open-label, multicentre trial - showed no significant reduction in 30-day mortality with IABP vs. medical therapy alone in AMI complicated by cardiogenic shock in patients undergoing early revascularisation
- 30-day mortality: 39.7% (IABP) vs. 41.3% (control); RR 0.96; 95% CI 0.79-1.17; P=0.69
- No significant differences in secondary endpoints, time to haemodynamic stabilisation, or ICU length of stay
- 6-year follow-up confirmed no long-term survival benefit
- This has led current ESC and AHA/ACC guidelines to downgrade the routine use of IABP in cardiogenic shock complicating AMI (Class III / no benefit recommendation)
VII. COMPLICATIONS (Benchmark Registry Data)
| Complication | Rate |
|---|---|
| Major complications (overall) | 2.6% |
| All complications | 8.1% |
| IABP-related complications (high-risk CABG meta-analysis) | 5.6% |
| Most common specific complications | Limb ischaemia, insertion-site haematoma |
VIII. WEANING AND REMOVAL
IABP weaning is achieved by:
- Decreasing counterpulsation frequency: 1:1 → 1:2 → 1:3
- Reducing augmentation volume (partial inflation)
The device is removed when the patient tolerates 1:3 support without haemodynamic deterioration. Removal is percutaneous with manual compression of the femoral artery for 30-45 minutes; surgical cutdown is not required unless access was via surgical graft.
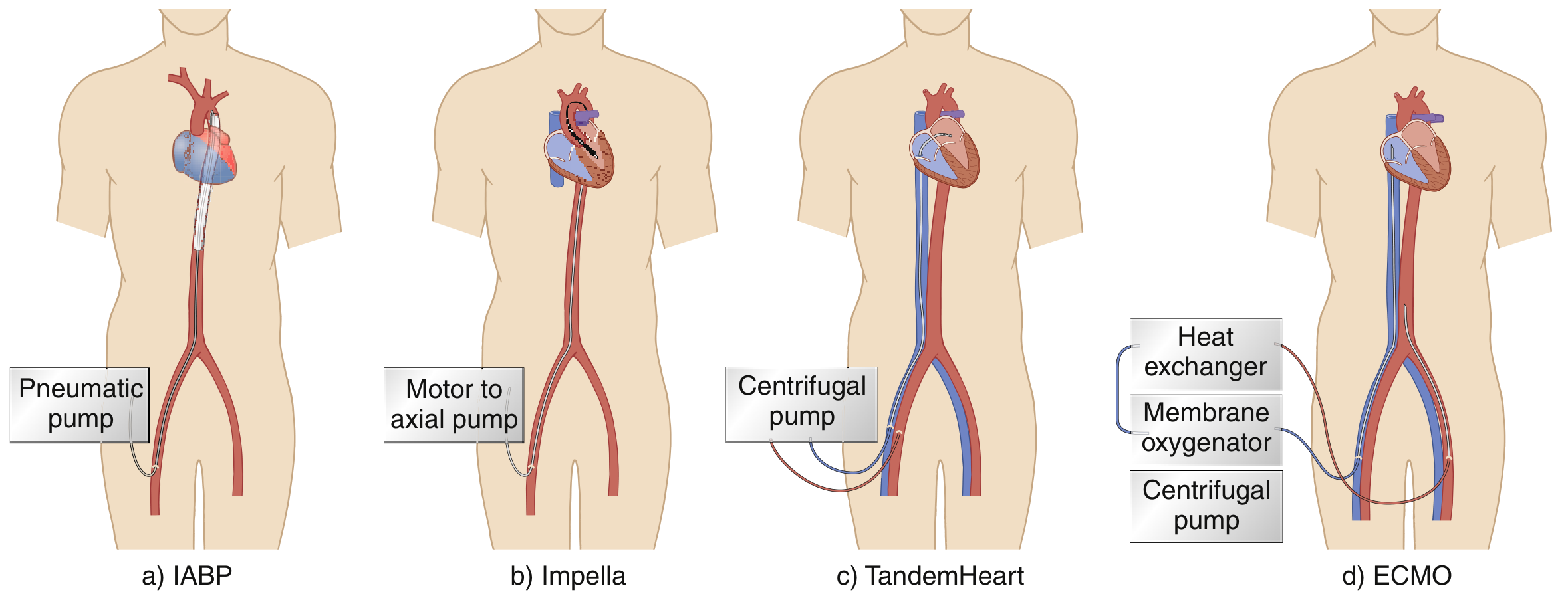
IX. COMPARISON WITH OTHER MCS DEVICES
| Feature | IABP | Impella CP | TandemHeart | VA-ECMO |
|---|---|---|---|---|
| Flow support (L/min) | 0.5-1.0 | 2.5-4.0 | Up to 4.0 | 2-6 |
| Mechanism | Counterpulsation | Axial rotary pump | Centrifugal pump | Centrifugal + oxygenator |
| LV support | Indirect (afterload) | Direct (transvalvular) | Direct (transseptal) | Biventricular |
| Oxygenation | No | No | No | Yes |
| Ease of use | Highest | Moderate | Specialist | Specialist |
| Haemolysis | Minimal | Moderate | Moderate-high | Moderate |
| ECG dependence | Yes | No | No | No |
| Ambulation possible | With axillary insertion | Limited | No | No |
X. SUMMARY
The IABP remains the most commonly used, most accessible, and most rapidly deployable MCS device. Its dual mechanism - diastolic augmentation of coronary perfusion and systolic afterload reduction - makes it uniquely suited to ischaemic cardiogenic shock and perioperative cardiac failure. Its advantages include ease of placement, wide availability, continuous haemodynamic monitoring, and reversibility. Its limitations are a modest cardiac output increment (~0.5-1.0 L/min), rhythm dependence, and the inability to support a completely failing heart. The IABP-SHOCK II trial fundamentally challenged its routine use in AMI-cardiogenic shock, shifting the paradigm toward careful case selection rather than universal insertion. Modern MCS algorithms reserve IABP for specific indications (mechanical complications, peri-CABG support, bridge to decision) while employing higher-output devices (Impella, ECMO) for refractory biventricular failure.
Sources: Braunwald's Heart Disease 12e; Fischer's Mastery of Surgery 8e; Sabiston Textbook of Surgery 21e; Tintinalli's Emergency Medicine 9e; Rosen's Emergency Medicine 9e; Fuster & Hurst's The Heart 15e; Mulholland & Greenfield's Surgery 7e
This is a shared conversation. Sign in to Orris to start your own chat.