Find out Blood Group of your own Bloof Find out abnormal Constituments quring Sample
Checking Date & Time
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have rich content from the textbooks. Let me compile the comprehensive answer.
🩸 Blood Grouping & Abnormal Urine Constituents
PART 1 — Blood Group Determination (ABO & Rh Typing)
What is a Blood Group?
Blood group refers to genetically encoded antigens on red blood cells (RBCs), inherited by autosomal Mendelian rules with codominance. The ABO and Rh (D antigen) systems are the most clinically important because they are the most immunogenic.
— Henry's Clinical Diagnosis and Management by Laboratory Methods
The ABO System
The ABO system is based on H antigen (a precursor on all RBCs):
- Type A → transferase adds N-acetylgalactosamine to H antigen → A antigen
- Type B → transferase adds galactose to H antigen → B antigen
- Type AB → both transferases present → A and B antigens
- Type O → neither transferase → H antigen persists
Because infants are rapidly exposed to intestinal bacteria with A/B-like antigens, they develop antibodies against whichever ABO antigens they lack:
| Blood Type | Antigens on RBCs | Antibodies in Plasma | Frequency (USA) | Can Agglutinate |
|---|---|---|---|---|
| O | None (H antigen) | Anti-A + Anti-B | 45% | A, B, AB cells |
| A | A | Anti-B | 41% | B, AB cells |
| B | B | Anti-A | 10% | A, AB cells |
| AB | A and B | None | 4% | None |
— Ganong's Review of Medical Physiology, 26th Edition
How ABO Typing is Performed
Two steps are required for serologic ABO determination:
1. Forward (Front) Type — Detects antigens on patient's RBCs:
- Patient RBCs + Reagent Anti-A → agglutination if A antigen present
- Patient RBCs + Reagent Anti-B → agglutination if B antigen present
2. Reverse (Back) Type — Detects naturally occurring antibodies in patient's plasma:
- Patient plasma + Reagent A₁ cells → agglutination if Anti-A present
- Patient plasma + Reagent B cells → agglutination if Anti-B present
Both results must agree with a single conclusion. Disagreement = ABO discrepancy requiring investigation.
ABO Typing Interpretation Table (from Tietz Textbook of Laboratory Medicine, 7th Ed.):
| ABO Group | RhD | Anti-A | Anti-B | Anti-D | A₁ Cell | B Cell |
|---|---|---|---|---|---|---|
| O | Positive | 0 | 0 | 4+ | 4+ | 4+ |
| O | Negative | 0 | 0 | 0 | 4+ | 4+ |
| A | Positive | 4+ | 0 | 4+ | 0 | 4+ |
| A | Negative | 4+ | 0 | 0 | 0 | 4+ |
| B | Positive | 0 | 4+ | 4+ | 4+ | 0 |
| B | Negative | 0 | 4+ | 0 | 4+ | 0 |
| AB | Positive | 4+ | 4+ | 4+ | 0 | 0 |
| AB | Negative | 4+ | 4+ | 0 | 0 | 0 |
(0 = no agglutination; 4+ = strong agglutination)
— Tietz Textbook of Laboratory Medicine, 7th Edition
Rh (D) Typing
The Rh type detects the presence or absence of the D antigen on RBCs:
- Patient RBCs + Reagent Anti-D → agglutination = Rh Positive; no agglutination = Rh Negative
- The D antigen is the most immunogenic blood group antigen after A and B (relative potency = 0.70 — meaning ~70% of D-negative individuals will form Anti-D if transfused with D-positive blood)
- Weak D / Partial D variants require Anti-Human Globulin (AHG) enhancement and molecular genotyping for definitive classification
Relative Immunogenicity of Key Antigens:
| Antigen | Relative Potency | Antigen | Relative Potency |
|---|---|---|---|
| D | 0.70 | K | 0.10 |
| C | 0.041 | E | 0.0338 |
| Fya | 0.0046 | Jka | 0.0014 |
— Henry's Clinical Diagnosis and Management by Laboratory Methods
PART 2 — Abnormal Constituents Found During Urine Examination (Urinalysis)
A routine urine examination looks for normal and abnormal constituents — substances that should not appear in urine, or appear in excess.
Abnormal Chemical Constituents
| Constituent | Clinical Significance | Detection |
|---|---|---|
| Protein (Proteinuria) | Renal disease, nephrotic syndrome, preeclampsia, heart failure, DM nephropathy | Reagent strip (albumin-sensitive); Sulfosalicylic acid (SSA) for globulins; quantitative 24-hr collection |
| Glucose (Glucosuria) | Diabetes mellitus, renal glycosuria, Fanconi syndrome | Reagent strip (glucose oxidase method) |
| Ketones (Ketonuria) | DKA, starvation, high-fat diets, vomiting | Reagent strip (nitroprusside reaction) |
| Blood/Hemoglobin (Hematuria/Hemoglobinuria) | Kidney stones, glomerulonephritis, trauma, hemolysis | Reagent strip (pseudoperoxidase reaction) |
| Bilirubin (Bilirubinuria) | Hepatocellular disease, obstructive jaundice | Reagent strip (diazonium reaction) |
| Urobilinogen (excess) | Hemolytic anemia, hepatic disease | Reagent strip |
| Nitrite | Bacterial UTI (gram-negative organisms) | Reagent strip |
| Leukocyte Esterase | Pyuria, UTI | Reagent strip |
Abnormal Crystals Found in Urine (Pathological)
These crystals are significant and indicate disease (unlike normal crystals seen in acidic/alkaline urine):
| Crystal | Appearance | pH | Clinical Significance |
|---|---|---|---|
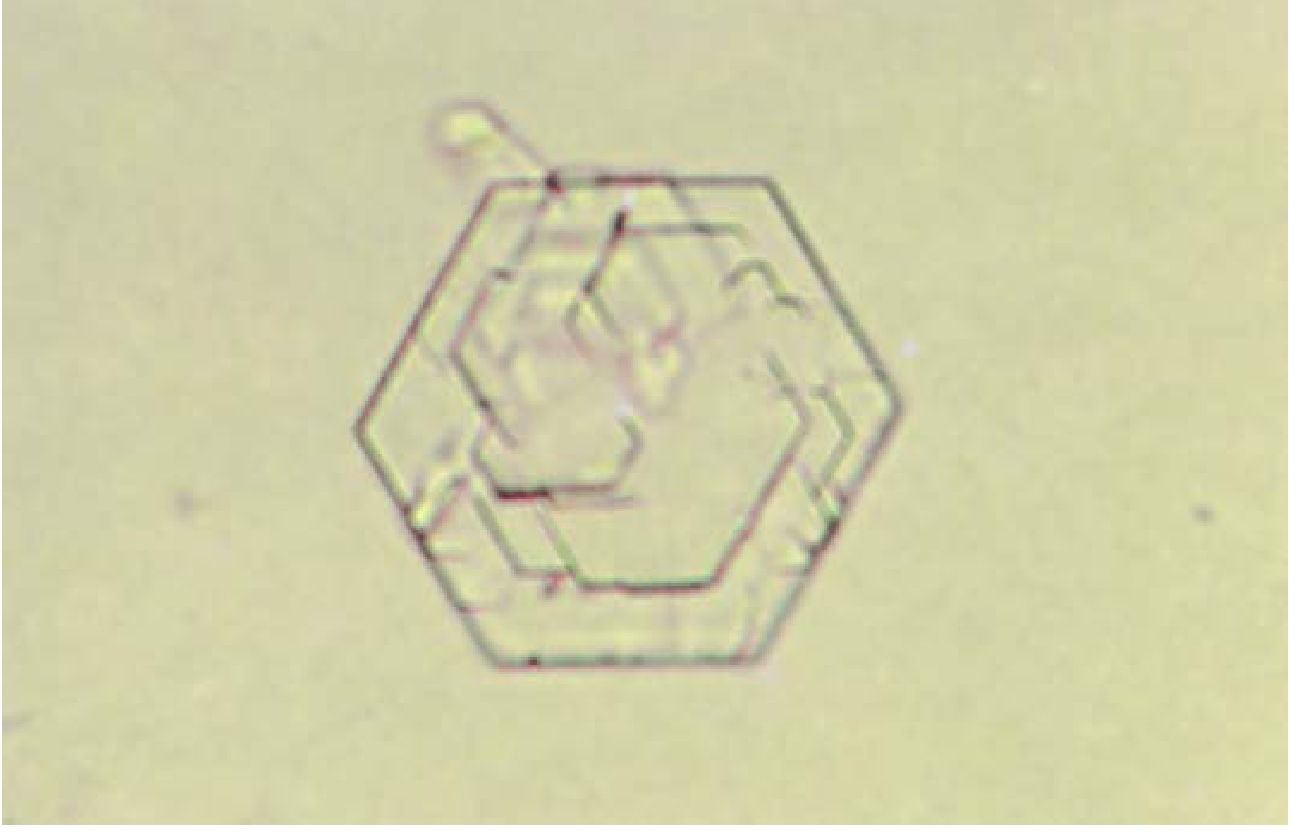
| Cystine | Colorless, hexagonal plates (refractile) | Acid | Cystinuria, cystine calculi — confirm with cyanide-nitroprusside test |
| Tyrosine | Fine silky needles in sheaves/clumps; yellow → black under microscope | Acid | Severe liver disease, tyrosinemia (inborn error of metabolism) |
| Leucine | Yellow, oily-appearing spheres with concentric lamellae | Acid | Severe liver disease, maple syrup urine disease |
| Cholesterol | Flat, transparent plates with notched corner | Acid | Nephrotic syndrome, chyluria |
| Sulfonamide crystals | Various sheaf/fan shapes | Acid | Sulfonamide drug therapy (e.g., sulfamethoxazole — Bactrim/Septra) |
| Ampicillin | Long, fine, colorless needles | Acid | High-dose ampicillin therapy |
| Radiographic dye (Diatrizoate) | Flat rhombic plates, easily polarized | Acid | Post-IV contrast; high specific gravity (>1.040) |

— Henry's Clinical Diagnosis and Management by Laboratory Methods
Abnormal Cells & Formed Elements in Urine
| Element | Significance |
|---|---|
| RBCs (>3/HPF) | Hematuria — glomerulonephritis, calculi, tumor, trauma |
| WBCs (>5/HPF) | Pyuria — UTI, pyelonephritis, interstitial nephritis |
| RBC casts | Glomerulonephritis (pathognomonic) |
| WBC casts | Pyelonephritis, interstitial nephritis |
| Granular casts | Chronic renal disease |
| Waxy/broad casts | Advanced renal failure |
| Malignant tumor cells | Renal pelvis, ureter, bladder carcinoma |
| Viral inclusion cells | CMV, polyomavirus (BK virus) infections |
| Myeloma cells | Multiple myeloma with renal involvement |
Key Points Summary
Blood Grouping:
- ABO typing requires both forward (antigen detection) and reverse (antibody detection) testing
- Rh typing identifies the D antigen — Rh+ or Rh−
- D is the most immunogenic non-ABO antigen (70% sensitization rate)
- ABO + Rh type must be determined before any blood transfusion
Abnormal Urine Constituents:
- Pathological crystals (cystine, tyrosine, leucine) indicate metabolic or hepatic disease
- Chemical abnormalities (protein, glucose, ketones, blood, bilirubin) detected by dipstick reagent strip
- Casts and abnormal cells in urine sediment provide critical diagnostic clues for renal and systemic disease
This is a shared conversation. Sign in to Orris to start your own chat.