What is Ischemia
Reading File
Finding Sources
Searching PubMed
ischemia pathophysiology mechanisms
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Here is a thorough, textbook-grounded explanation of ischemia:
Ischemia
Definition
Ischemia is the reduction or complete cessation of blood flow to a tissue or organ, resulting in a deficiency of oxygen AND metabolic substrates (glucose, etc.) simultaneously. This distinguishes it from simple hypoxia, where blood flow is maintained and at least some anaerobic glycolysis can continue.
"Ischemia, a common cause of cell injury in clinical medicine, results from hypoxia induced by reduced blood flow, most often due to a mechanical arterial obstruction. It can also occur due to reduced venous drainage."
- Robbins, Cotran & Kumar - Pathologic Basis of Disease
Why Ischemia Is More Damaging Than Hypoxia Alone
In pure hypoxia, flowing blood still delivers glucose so cells can produce some ATP via anaerobic glycolysis. In ischemia, blood flow stops entirely, so:
- Aerobic metabolism ceases (no oxygen)
- Anaerobic glycolysis also fails once glycolytic substrates run out or metabolic waste products (lactic acid) accumulate and cannot be washed away
- The result is faster, more severe cell injury
Causes
| Category | Examples |
|---|---|
| Arterial obstruction | Atherosclerotic plaque, thrombosis, embolism |
| Vasospasm | Coronary artery spasm, Raynaud's phenomenon |
| Hypoperfusion | Shock, severe hypotension, cardiac failure |
| Venous obstruction | Thrombosis causing back-pressure and reduced arterial inflow |
| Compression | Tumor, compartment syndrome, strangulated hernia |
Cellular Mechanisms of Ischemic Injury
The diagram below (from Robbins Pathology) summarizes the cascade beautifully:
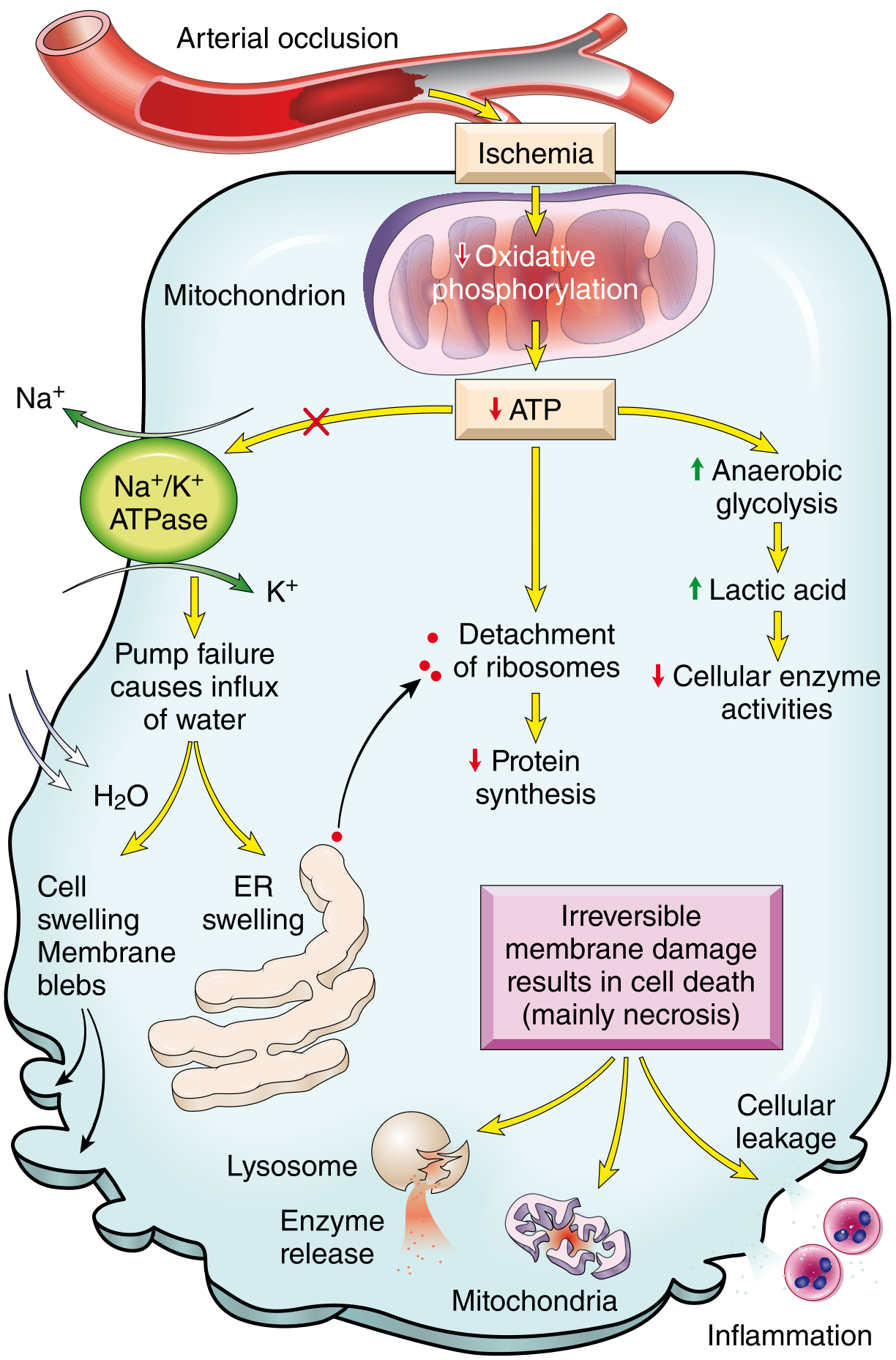
Fig. 2.24 - Functional and morphologic consequences of decreased intracellular ATP in ischemic cell injury (Robbins, Cotran & Kumar - Pathologic Basis of Disease)
Step-by-step cellular cascade:
- Reduced blood flow → oxygen tension falls → oxidative phosphorylation fails
- ATP depletion triggers multiple parallel injury pathways:
- Na⁺/K⁺ ATPase pump failure → Na⁺ accumulates inside cell → water influx → cell and ER swelling, membrane blebs
- Anaerobic glycolysis upregulates → lactic acid accumulates → intracellular pH drops → reduces cellular enzyme activity
- Ribosome detachment from ER → reduced protein synthesis
- If ischemia is brief and mild: these changes are reversible
- If ischemia continues: irreversible membrane damage occurs → lysosomal rupture → enzyme release → necrosis
Reversible vs. Irreversible Injury
| Feature | Reversible | Irreversible |
|---|---|---|
| Duration | Short (minutes) | Prolonged (>20-60 min depending on tissue) |
| Changes | Cell swelling, ER swelling, blebs | Membrane rupture, lysosomal lysis |
| Outcome | Recovery if perfusion restored | Cell death (necrosis) |
| Example (heart) | Angina | Myocardial infarction |
The heart tolerates ischemia for roughly 20 minutes before irreversible injury occurs. The brain is far more sensitive - irreversible neuronal damage begins within 4-6 minutes.
Ischemia-Reperfusion Injury
Paradoxically, restoring blood flow to ischemic tissue can cause additional damage through:
- Oxidative stress - Reoxygenation generates a burst of reactive oxygen species (ROS) from leukocytes and damaged endothelium; antioxidant defenses are already depleted
- Intracellular calcium overload - Influx of Ca²⁺ during reperfusion opens mitochondrial permeability transition pores, further depleting ATP
- Inflammation - Dead cells release "danger signals"; cytokines recruit neutrophils which cause additional tissue destruction
- Complement activation - IgM antibodies deposited in ischemic tissue activate complement on reperfusion
This is clinically relevant in myocardial infarction treated with thrombolytics or angioplasty, and in stroke managed with tPA.
Protective Responses
The body activates Hypoxia-Inducible Factor-1 (HIF-1), a transcription factor that:
- Promotes angiogenesis (new blood vessel formation)
- Stimulates cell survival pathways
- Upregulates glycolytic enzymes
The most proven clinical intervention remains therapeutic hypothermia (cooling to ~33°C), which reduces metabolic demand, limits cell swelling, suppresses free radical formation, and blunts inflammation - used in post-cardiac arrest care and neonatal hypoxic-ischemic encephalopathy.
Common Clinical Manifestations by Organ
| Organ | Condition | Key Symptoms |
|---|---|---|
| Heart | Angina / MI | Chest pain, dyspnea |
| Brain | TIA / Stroke | Focal neurological deficits, altered consciousness |
| Gut | Mesenteric ischemia | Abdominal pain out of proportion to exam, bloody diarrhea |
| Limb | Peripheral arterial disease / acute limb ischemia | The 6 P's: Pain, Pallor, Pulselessness, Paresthesia, Paralysis, Poikilothermia |
| Kidney | Renal ischemia | AKI, oliguria |
| Eye | Ocular ischemic syndrome | Visual loss, amaurosis fugax |
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease; Barash - Clinical Anesthesia 9e; Henry's Clinical Diagnosis and Management; Goldman-Cecil Medicine
Bradycardia
Finding Sources
Searching PubMed
bradycardia management treatment
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Here is a comprehensive, textbook-based guide to bradycardia:
Bradycardia
Definition
Bradycardia is a heart rate of fewer than 60 beats per minute (bpm). It can be physiological (normal) or pathological depending on the clinical context.
Sinus bradycardia ECG (lead III) - Guyton & Hall Medical Physiology:

Types and Causes
1. Physiological Bradycardia
- Athletes: Well-trained athletes have larger, stronger hearts with higher stroke volumes per beat. At rest, increased arterial filling triggers baroreceptor reflexes that reduce heart rate. Additionally, exercise training downregulates the If ("funny") current ion channels in the SA node, reducing intrinsic pacemaker activity.
- Sleep: Heart rate normally drops during deep sleep due to increased vagal tone.
- Young adults with high resting vagal tone
2. Pathological Bradycardia - by Mechanism
| Mechanism | Examples |
|---|---|
| SA node disease | Sick sinus syndrome (SSS), fibrotic degeneration |
| Increased vagal tone | Vasovagal syncope, carotid sinus hypersensitivity, inferior MI, hemoperitoneum |
| AV conduction block | First-, second-, third-degree AV block |
| Drugs | Beta-blockers, calcium channel blockers, digoxin, amiodarone, dexmedetomidine |
| Metabolic/systemic | Hypothyroidism, hypothermia, hypoxia, hyperkalemia |
| Neurological | High cervical spinal cord injury (loss of sympathetic tone) |
| Cardiac | Inferior wall MI (sinoatrial node involvement), cardiomyopathy |
| Severe sepsis | Global cardiac dysfunction |
AV Block - The Conduction Ladder
AV block is a major cause of pathological bradycardia. Understanding the degrees is essential:
| Degree | ECG Finding | Clinical Significance |
|---|---|---|
| 1st degree | PR interval > 0.20 sec; every P conducts | Normal variant in up to 2% of young adults; no treatment usually needed |
| 2nd degree - Mobitz I (Wenckebach) | Progressive PR lengthening → dropped QRS; cycle repeats | Block at AV node level; often benign but monitor |
| 2nd degree - Mobitz II | Fixed PR interval → intermittent dropped QRS | Block below AV node (His-Purkinje); more dangerous; may need pacing |
| 3rd degree (Complete heart block) | No relationship between P waves and QRS; escape rhythm | Life-threatening; requires pacemaker |
Sick Sinus Syndrome (SSS)
A group of dysrhythmias from disease of the SA node and surrounding tissue, producing:
- Sinus bradycardia
- Sinus arrest
- SA exit block
- Bradycardia-tachycardia syndrome - bradycardia alternating with tachyarrhythmia (usually AF)
Most common in older adults due to fibrotic degeneration. Long-term management requires permanent pacemaker placement to allow safe use of pharmacologic therapy for the tachycardic episodes.
Symptoms
Symptoms arise when heart rate is so slow that cardiac output falls. Common presentations:
- Dizziness / lightheadedness (most common)
- Syncope or near-syncope - can occur with sudden drop in rate (e.g., carotid sinus syndrome can stop the heart for 5-10 seconds)
- Fatigue and exercise intolerance (chronotropic incompetence)
- Dyspnea
- Palpitations (from escape beats)
- Hemodynamic compromise - hypotension, shock in severe cases
"The most common bradycardia-induced symptoms are dizziness or lightheadedness, syncope or near-syncope."
- Goldman-Cecil Medicine
Management
Step 1 - Assess Hemodynamic Stability
If the bradycardia is not causing hemodynamic compromise, it may not require treatment (e.g., asymptomatic sinus bradycardia in a fit young person).
Step 2 - Treat the Underlying Cause
Always prioritize reversing the cause: stop offending drugs, treat hypothyroidism, manage MI, treat hypoxia.
Step 3 - Pharmacological Treatment (Symptomatic/Unstable)
| Drug | Dose | Notes |
|---|---|---|
| Atropine | 1 mg IV q3-5 min (max 3 mg) | First-line for sinus bradycardia and AV nodal block |
| Dopamine infusion | Titrated | Second-line if atropine fails |
| Epinephrine infusion | Titrated | For severe or refractory bradycardia |
| Isoproterenol | 2-10 mcg/min | Post-heart transplant patients (atropine is ineffective in denervated hearts) |
Important caveat: Atropine is ineffective for:
- Junctional or ventricular bradycardia from complete AV node dysfunction
- Dexmedetomidine-induced bradycardia (due to alpha-2 agonist mechanism)
- Post-transplant bradycardia (denervated heart)
Step 4 - Pacing
| Type | When Used |
|---|---|
| Transcutaneous (external) pacing | Emergency, immediate bridge |
| Transvenous temporary pacing | Bridge to definitive treatment or recovery |
| Permanent pacemaker | Symptomatic bradycardia from irreversible cause (SSS, complete AV block, Mobitz II) |
"Pacemakers are implanted either to alleviate symptoms caused by bradycardia or to prevent severe symptoms in patients in whom symptomatic bradycardia is likely to develop."
- Goldman-Cecil Medicine
Key Clinical Pearls
- Inferior wall MI commonly causes sinus bradycardia because the RCA supplies the SA node in ~60% of people; treat with atropine
- Carotid sinus syndrome - even mild neck pressure can trigger extreme bradycardia/asystole and syncope
- Vasovagal syncope involves both hypotension and bradycardia; treat with lifestyle modification, hydration, compression stockings; rarely needs pacing
- High cervical spinal cord injury causes bradycardia via loss of sympathetic tone; treat with atropine + vasopressors
- A rate below 40 bpm may allow emergence of a junctional escape rhythm
- First-degree AV block - avoid nodal blocking agents; generally does not require treatment on its own
Sources: Guyton & Hall - Medical Physiology; Rosen's Emergency Medicine; Sabiston - Textbook of Surgery; Goldman-Cecil Medicine; Braunwald's Heart Disease; Harrison's Principles of Internal Medicine 22e
This is a shared conversation. Sign in to Orris to start your own chat.