teach me urology hacks of emergency
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Excellent - I now have comprehensive content across all major emergency urology topics. Here is the complete guide:
Emergency Urology Hacks - The Practical Field Guide
Sources: Rosen's Emergency Medicine, Roberts & Hedges' Clinical Procedures in Emergency Medicine, Tintinalli's Emergency Medicine, Campbell-Walsh-Wein Urology, Brenner & Rector's The Kidney, Sabiston Textbook of Surgery, Bailey & Love's Surgery
1. TESTICULAR TORSION - The "6-Hour Clock"
The single most important rule in emergency urology: time = testicle.
| Window | Salvage Rate |
|---|---|
| < 6 hours | > 90% |
| 6-12 hours | ~50% |
| > 24 hours | < 10% |
The Diagnostic Table (No single finding rules it out)
| Feature | Torsion | Appendix Torsion | Epididymitis |
|---|---|---|---|
| Age | <1 yr, puberty | 7-14 years | Adult |
| Onset | Hours | 1-2 days | Days-weeks |
| Pain location | Whole testicle | Upper pole | Epididymis |
| Testis position | High-riding, transverse | Normal, vertical | Normal, vertical |
| Systemic signs | Nausea/vomiting | None | Possibly fever |
| Cremasteric reflex | ABSENT | Intact | Intact |
| Pyuria | Rare | No | Yes |
| Doppler USS | Absent/decreased flow | Normal flow | Increased flow |
Hack: Absent cremasteric reflex + high-riding transverse testicle = torsion until proven otherwise. Do NOT wait for ultrasound if clinical suspicion is high - go straight to OR.
Manual Detorsion Technique (Buys Time While Prepping OR)
The "open the book" maneuver - two thirds of torsions twist lateral-to-medial, so you detorse medial-to-lateral (like opening a book outward):
- Call urology AND prep for OR simultaneously
- Give spermatic cord anesthesia (optional): 1% lidocaine without epinephrine, 10 mL into the cord at the external inguinal ring
- Stand at the patient's right side (right-hand dominant)
- Rotate the right testicle counter-clockwise (medial to lateral) - rotate 180 degrees first
- May need 2-3 full rotations - endpoint is pain relief
- If pain worsens, detorse in the opposite direction (some torse the other way)
- Confirm with bedside Doppler - return of flow = success
- Surgical exploration is still mandatory even after successful manual detorsion
Key hack: Even if manual detorsion succeeds clinically, surgical bilateral orchiopexy is still required - the risk of re-torsion is 100% without fixation.
- Rosen's Emergency Medicine, p. 1401
- Roberts & Hedges' Clinical Procedures in Emergency Medicine, p. 1302
2. PRIAPISM - Compartment Syndrome of the Penis
The rule: Ischemic (low-flow) priapism = painful, dark blood = emergency. Non-ischemic (high-flow) = painless, bright red blood = NOT urgent.
Distinguishing Ischemic vs. Non-Ischemic
| Feature | Ischemic (Low-Flow) | Non-Ischemic (High-Flow) |
|---|---|---|
| Pain | Yes, severe | Painless or mild |
| Blood gas | Dark, deoxygenated | Bright red, oxygenated |
| Cause | Sickling, drugs, idiopathic | Post-traumatic AV fistula |
| Urgency | EMERGENCY | Elective |
| Treatment | Aspiration + alpha-agonist | Angioembolization (urology/IR) |
Over one third of patients with severe priapism suffer permanent ED despite treatment - act fast.
Step-by-Step ED Management (Ischemic Priapism)
- Pain control - parenteral opioid or light sedation
- Trial of terbutaline: 0.25-0.5 mg SC (repeat in 15 min), or 5 mg PO
- Intracorporal alpha-agonist injection (first-line definitive):
- Phenylephrine: dilute to 100-500 mcg/mL, inject 1 mL into lateral corpus at 3 or 9 o'clock position using a 23-gauge butterfly needle
- Repeat every 20 min x 3 doses max
- Monitor BP - systemic absorption causes hypertension
- Note: only ONE corpus needs to be accessed (they communicate)
- If still erect: aspiration - withdraw 20-30 mL of dark blood
- If still erect: corporal irrigation - normal saline aspirate-irrigate cycle until blood turns bright red (arterial = success)
- Persistent erection = call urology for Winter shunt or cavernosum-spongiosum shunt
- After resolution: wrap penis loosely in elastic bandage, 3-day oral alpha-agonist, urgent urology follow-up
Hack: The spongy urethra and glans are SOFT in priapism - only the corpora cavernosa are rigid. This confirms diagnosis. Injection at 3 or 9 o'clock avoids the dorsal neurovascular bundle.
Common causes to ask about: Sickle cell disease (highest recurrence), PDE5 inhibitor overdose, antipsychotics (especially chlorpromazine, trazodone), cocaine
- Roberts & Hedges' Clinical Procedures, p. 1306
3. ACUTE URINARY RETENTION - The Foley Is Your Friend
Common Causes by Category
Obstructive: BPH (most common in men), prostate cancer, phimosis, paraphimosis, urethral stricture, clot retention, meatal stenosis, calculus, foreign body
Infectious/Inflammatory: Acute prostatitis, urethritis, vulvovaginitis, genital herpes
Neurogenic: Spinal cord injury, MS, Parkinson's, cauda equina syndrome (RED FLAG - do not miss), diabetic neuropathy
Drugs (memorize these):
- Anticholinergics (bladder relaxation)
- Tricyclics, antihistamines
- Alpha-agonists (cold/decongestant tablets, ephedrine)
- NSAIDs, calcium channel blockers (inhibit detrusor)
Hack: Always ask about recent cold/flu medications. Pseudoephedrine is a silent culprit.
ED Management
- Catheterize immediately - 14-18 Fr Foley catheter
- If Foley fails (stricture, false passage): try a coude-tip catheter; do NOT force
- Suprapubic catheter if urethral access impossible
- Rapid complete decompression is the current recommendation - the old "clamp the catheter every 500 mL" is NOT supported by evidence
- Urine output > 200 mL/hour after decompression = post-obstructive diuresis - watch electrolytes and replace fluids if sustained
- Leave catheter 3-7 days before voiding trial - early removal has up to 70% recurrence rate
- Start tamsulosin 0.4 mg daily at time of catheter insertion (improves TWOC success in BPH patients)
- Do NOT give prophylactic antibiotics for catheter insertion alone - promotes resistance
- Check creatinine only if prolonged obstruction or pre-existing renal disease is suspected
Disposition:
- Uncomplicated AUR with BPH + catheter draining well = discharge with catheter and urology follow-up
- Fever, renal impairment, neurologic deficits, failed catheterization = admit
RED FLAG: AUR + saddle anesthesia + bilateral leg weakness = cauda equina syndrome - emergency MRI spine NOW.
- Rosen's Emergency Medicine, pp. 1408-1410
4. RENAL COLIC - Pain Control First, Then Work Up
Pain Management (The Priority)
- NSAIDs are first-line (ketorolac 15-30 mg IV) - as effective as opioids, fewer side effects, less nausea
- Opioids if NSAIDs contraindicated (renal impairment, allergy, anticoagulation)
- Antiemetics (ondansetron or metoclopramide) are often needed
- IV fluids for hydration, antiemetics, and stone passage facilitation
- Forced IV hydration does NOT speed stone passage - do not over-hydrate
Medical Expulsive Therapy (MET)
- Tamsulosin 0.4 mg daily for stones 5-10 mm - reduces ureteral smooth muscle tone and increases spontaneous passage rate
- AUA recommendation: tamsulosin for stones < 10 mm with 4-6 weeks observation
- EAU recommendation: alpha-blockers for stones > 5 mm
- Tamsulosin is superior to nifedipine for MET
- Cochrane review (67 studies, 10,509 participants): alpha-blockers increase clearance AND shorten expulsion time
When to Admit (Cannot Discharge)
- Infection + obstruction = urological emergency (urosepsis in the making) - needs urgent nephrostomy/stent
- Persistent uncontrolled pain
- Intractable vomiting
- Solitary kidney with obstruction
- Stone > 10 mm (< 1% chance of spontaneous passage)
- Bilateral obstruction
Hack: The triad of fever + flank pain + obstructed stone = urosepsis. This needs emergency decompression (nephrostomy tube or ureteral stent) within hours, not days. Antibiotics alone are insufficient.
- Brenner & Rector's The Kidney, p. 1735
5. PARAPHIMOSIS - Reduce It Before It Necroses
Paraphimosis is the inability to reduce the retracted foreskin back over the glans - the constricting ring causes progressive venous obstruction, edema, and eventually arterial ischemia.
Reduction Steps
Step 1 - Analgesia first:
- Dorsal penile nerve block: inject 1% lidocaine WITHOUT epinephrine at 2 o'clock and 10 o'clock positions at the penile base, just deep to Buck's fascia (3-5 mm depth). Feel a slight "pop" through the fascia. Do not use epinephrine - causes vasoconstriction/ischemia.
Step 2 - Reduce edema:
- Ice pack for 3-minute increments (avoid cold injury)
- Manual palm compression of glans + foreskin for 5 minutes
- Elastic bandage wrapped from glans to base for 5-7 minutes
Step 3 - Manual reduction:
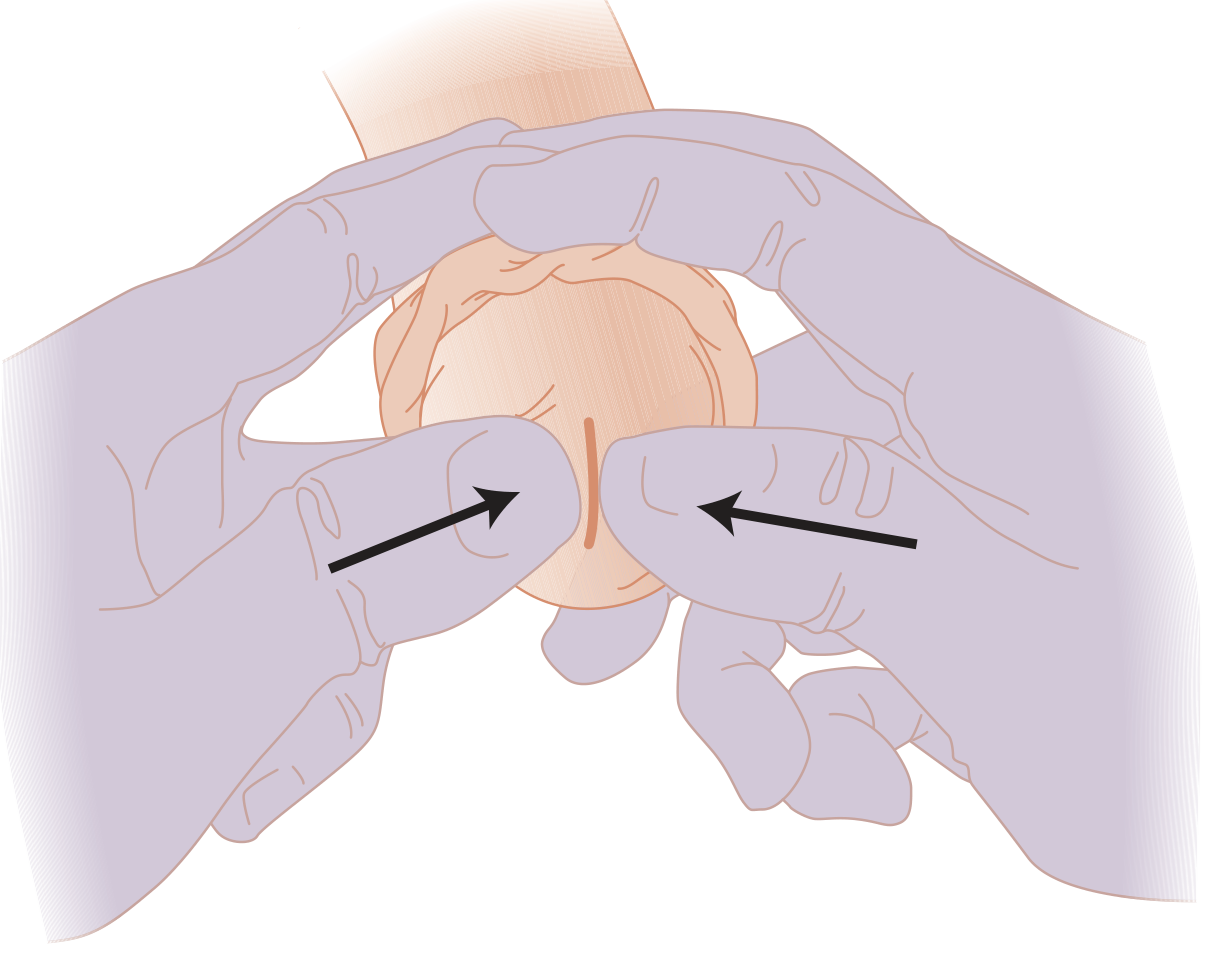
Place both thumbs over the glans, both index and long fingers surrounding the trapped foreskin. Push glans back (proximally) while pulling foreskin forward (distally) simultaneously. Apply slow, constant pressure for several minutes.
If manual reduction fails:
-
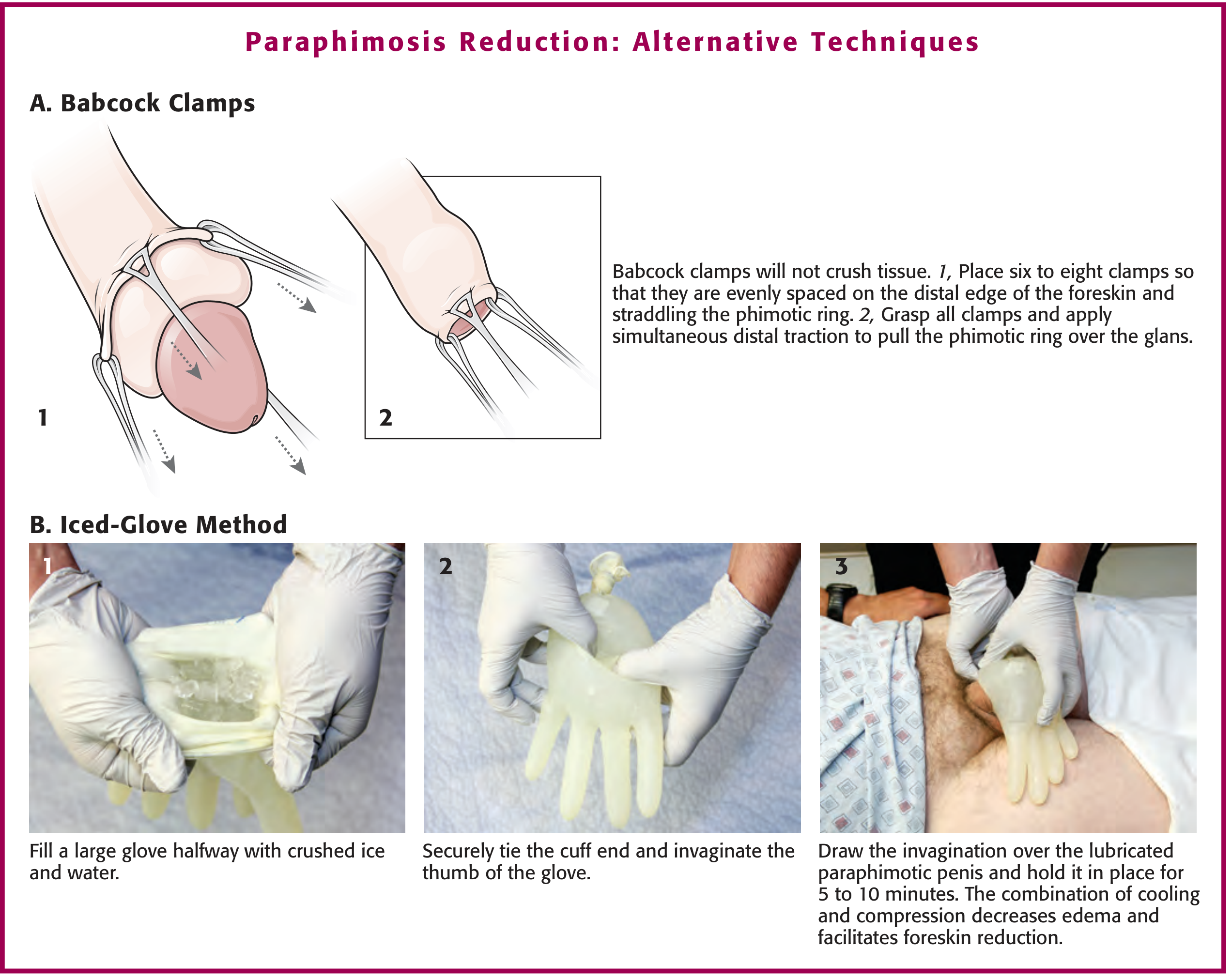
Iced-glove method: Fill a large glove halfway with crushed ice + water, tie the cuff, invaginate the thumb of the glove, draw over the lubricated paraphimotic penis for 5-10 minutes. Cooling + compression reduces edema.
-
Babcock clamp technique: 6-8 Babcock clamps evenly spaced on the distal foreskin straddling the phimotic ring; grasp all simultaneously and apply distal traction.
-
Dundee technique: Multiple micropunctures in the edematous foreskin with a hypodermic needle, then express edema fluid manually.
-
Hyaluronidase injection into the foreskin: hydrolysis of hyaluronic acid increases tissue permeability, dramatically reduces edema for easier reduction.
-
Surgical dorsal slit if all else fails - call urology.
-
Tintinalli's Emergency Medicine, p. 918
-
Roberts & Hedges' Clinical Procedures, p. 1314
6. FOURNIER'S GANGRENE - Never Miss It
This is a necrotizing fasciitis of the male genitalia and perineum - a true surgical emergency with mortality up to 20-40%.
Who Gets It
Diabetics, peripheral vascular disease, alcoholism, malnutrition, immunocompromised (HIV, steroids, transplant). Polymicrobial (aerobes + anaerobes + gram-positives + gram-negatives).
Presentation (Do Not Be Fooled)
- Severe scrotal/perineal pain, often out of proportion to early skin findings
- Scrotal/genital swelling and discoloration
- Crepitus - pathognomonic (subcutaneous gas from anaerobes)
- Foul-smelling discharge
- Early cases may have nearly normal-looking skin - pain + crepitus alone should trigger surgical consult
Hack: CT pelvis/perineum with contrast detects gas in tissue planes BEFORE visible skin necrosis appears. If you suspect Fournier's and skin looks normal, get the CT.
Treatment (No Delays)
- Broad-spectrum IV antibiotics immediately covering gram-positives, gram-negatives, and anaerobes (e.g., piperacillin-tazobactam + metronidazole, or meropenem)
- Urgent surgical debridement - aggressive, wide margins
- ICU-level supportive care
- Testes and deep penile structures (beneath tunica vaginalis and Buck's fascia) are usually spared and should be preserved
- Urethral catheter drainage is sufficient initially - suprapubic tube rarely needed acutely
- Wound care + skin grafting after infection controlled
- Sabiston Textbook of Surgery, p. 2819
Quick Reference: Emergency Urology Red Flags
| Presentation | Do NOT Miss | Key Action |
|---|---|---|
| Acute scrotal pain < 6h | Testicular torsion | Immediate OR, manual detorsion en route |
| Erection > 4 hours + painful | Ischemic priapism | Corporal aspiration + phenylephrine |
| AUR + saddle anesthesia + leg weakness | Cauda equina | Emergency MRI spine |
| Obstructed kidney + fever | Urosepsis | Urgent decompression (stent/nephrostomy) |
| Scrotal pain + crepitus + sick patient | Fournier's gangrene | CT + surgical team NOW |
| Foreskin trapped + distal edema | Paraphimosis | Reduce with ice + compression before necrosis |
Clinical bottom line: In emergency urology, the primary mistake is delay. Testicular torsion and Fournier's gangrene both have narrow windows. Priapism causes irreversible impotence after just a few hours. When in doubt, act and call urology simultaneously - not after.
This is a shared conversation. Sign in to Orris to start your own chat.