Hypokalaemia causes how to treat, what is the deficeit, how much kcl can be given
Reading File
Searching the Web
hypokalaemia treatment KCl dose deficit calculation guidelines 2024
Finding Sources
Searching PubMed
"hypokalemia" AND "treatment" AND "potassium replacement"
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive information from multiple authoritative textbooks and guidelines. Let me compile the full answer.
Hypokalaemia: Causes, Deficit Estimation, and Treatment
Definition
Hypokalaemia = serum K+ < 3.5 mmol/L
- Mild: 3.0-3.4 mmol/L
- Moderate: 2.5-2.9 mmol/L
- Severe: < 2.5 mmol/L
Causes
Hypokalaemia occurs by three main mechanisms: intracellular shift, reduced intake, and increased loss (renal or GI).
1. Intracellular Shift (K+ moves into cells)
| Cause | Mechanism |
|---|---|
| Alkalosis | Stimulates Na+-K+-ATPase |
| Insulin / glucose administration | Stimulates Na+-K+-ATPase |
| Beta-2-adrenergic agonists (salbutamol, theophylline) | Stimulates Na+-K+-ATPase |
| Familial hypokalemic periodic paralysis | Defective Ca++/K+ channels |
| Thyrotoxic hypokalemic paralysis | Excess catecholamines |
| Barium / chloroquine / hydroxychloroquine poisoning | K+ channel inhibition |
| Nutritional recovery / refeeding | Anabolism drives K+ into cells |
2. Reduced Intake
- Rare alone; usually prolonged starvation ("tea and toast" diet)
3. Gastrointestinal Loss
- Vomiting - K+ lost in urine (secondary hyperaldosteronism from volume depletion) more than in vomitus
- Diarrhoea / laxative abuse - direct stool loss
- Intestinal drainage, bowel prep (colonoscopy prep)
4. Renal Loss (most common overall)
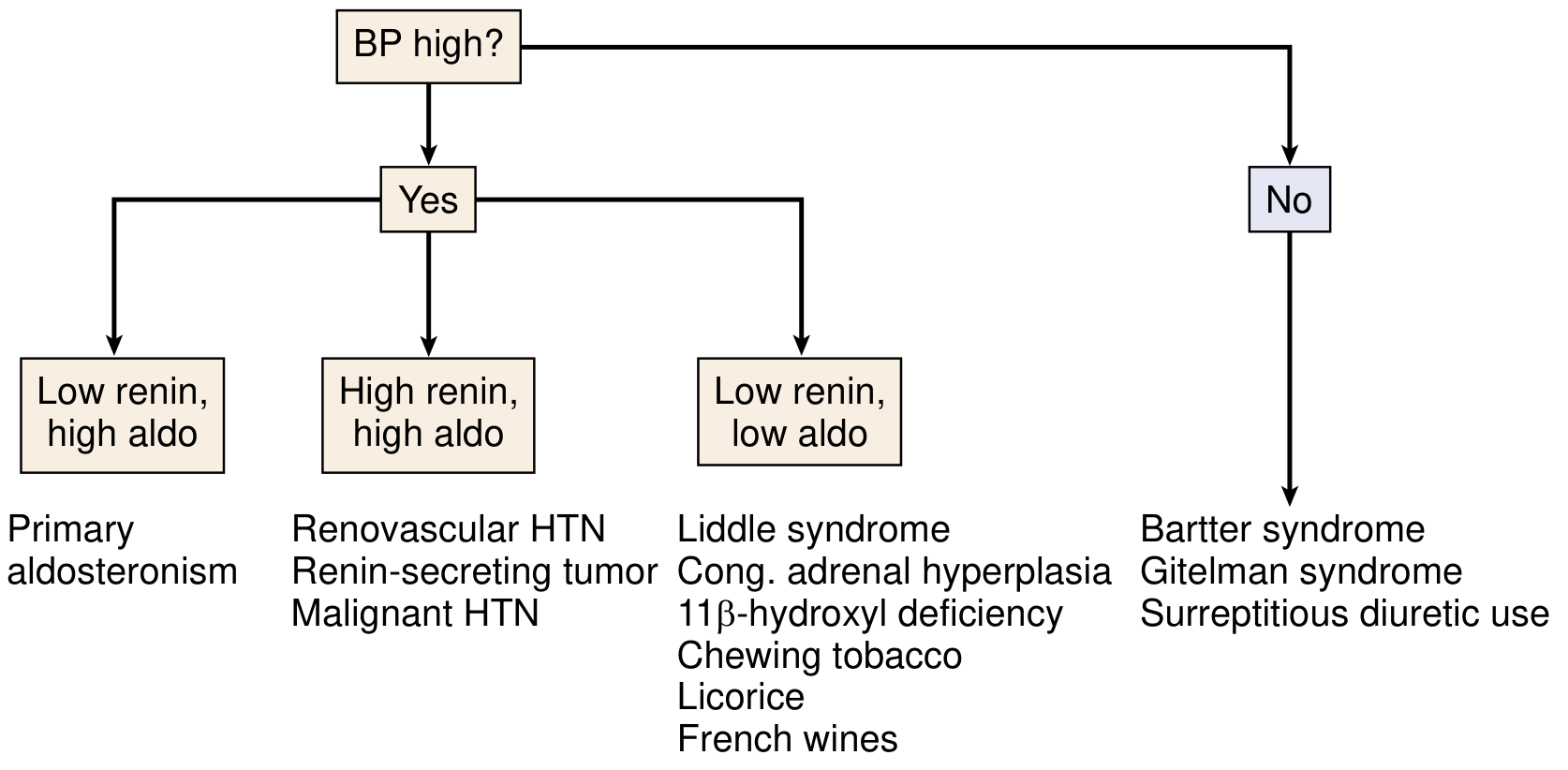
With hypertension:
| Renin | Aldosterone | Diagnosis |
|---|---|---|
| Low | High | Primary hyperaldosteronism (adenoma or bilateral hyperplasia) |
| High | High | Renovascular HTN, renin-secreting tumour, malignant HTN |
| Low | Low | Liddle syndrome, congenital adrenal hyperplasia, 11β-HSD deficiency, licorice, chewing tobacco |
Without hypertension (normal BP):
- Loop diuretics, thiazide diuretics (most common cause overall)
- Osmotic diuresis (hyperglycaemia, mannitol)
- Bartter syndrome, Gitelman syndrome
- Distal or proximal renal tubular acidosis
- Hypomagnesaemia (cisplatin, alcohol, diuretics)
- Surreptitious diuretic use
Differential diagnosis flowchart (from NKF Primer on Kidney Diseases):
Potassium Deficit Estimation
This is a clinical estimate - not exact - because many factors beyond total body stores affect serum K+:
For every 1 mEq/L fall in serum K+, the total body deficit is approximately 200-400 mEq
As much as 100-300 mmol of potassium may be lost from the body for each 1 mmol/L drop in serum K+.
Important caveats:
- The formula may overestimate deficit in transcellular shift states (e.g. hypokalemic periodic paralysis, insulin overdose) - do NOT overcorrect these
- The formula may underestimate true deficit in chronic depletion
- Concurrent acid-base status alters the relationship: alkalosis drives K+ into cells, worsening apparent (but not necessarily actual) hypokalemia
Practical deficit estimation table:
| Serum K+ (mmol/L) | Approximate Total Body Deficit |
|---|---|
| 3.0 - 3.5 | ~100-200 mmol |
| 2.5 - 3.0 | ~200-400 mmol |
| 2.0 - 2.5 | ~400-600 mmol |
| < 2.0 | up to 800+ mmol |
Treatment
Step 1: Treat the underlying cause
Remove or correct the precipitating factor (stop offending diuretic, treat vomiting, treat primary aldosteronism, etc.)
Step 2: Choose the potassium salt
- KCl (potassium chloride) - preferred; also corrects co-existing metabolic alkalosis (most common scenario)
- Potassium citrate - use in acidotic patients (e.g. renal tubular acidosis)
- Potassium phosphate - use when co-existing phosphate deficit
- Avoid potassium gluconate (non-reabsorbable anion - does not adequately replete the deficit)
Step 3: Choose the route
Oral replacement (preferred when possible):
- Used when K+ > 3.0 mmol/L, patient is not vomiting, and haemodynamically stable
- Usual dose: 40-100 mmol/day in divided doses (max 40 mmol per single dose)
- Total daily dose should not exceed 200 mmol/24 hours (FDA)
- If K+ 3.0-3.4 mmol/L: Sando-K 2 tablets TDS = 72 mmol K/day
- Dietary potassium increase can be considered if K+ > 3.0 mmol/L
Intravenous (IV) replacement:
Indicated when:
- Patient cannot take oral/enteral route
- Symptomatic hypokalaemia (paralysis, cardiac arrhythmias)
- Serum K+ < 3.0 mmol/L
- On IV aminophylline, DKA protocol
How Much KCl Can Be Given IV?
Standard / Peripheral IV rates:
| Serum K+ | Concentration | Rate | Setting |
|---|---|---|---|
| 3.0-3.5 mmol/L | 10 mmol in 500 mL (0.9% NaCl + 0.15% KCl) | 100-200 mL/hr | General ward |
| 2.5-3.0 mmol/L | 20-40 mmol in 1 L | Up to 10-20 mmol/hr | General ward (monitor) |
| < 2.5 mmol/L | Higher concentration | Up to 20-40 mmol/hr | HDU/ICU, cardiac monitoring |
Key safety limits:
| Setting | Max rate | Max concentration (peripheral) | Notes |
|---|---|---|---|
| General ward | 10 mmol/hr | ≤ 40 mmol/L | Safe for peripheral line |
| Monitored (telemetry) | 20 mmol/hr | ≤ 60 mmol/L | Requires ECG monitoring |
| ICU/Central line | 40 mmol/hr | Up to 200 mmol/L centrally | Continuous ECG, nurse 1:1 |
- If rate > 10 mmol/hr or K+ < 3.0 mmol/L, patient must be in a monitored setting
- Concentrations > 60 mmol/L must only be given via a central line
- Recheck serum K+ after each replacement course before giving further doses
- Do not use glucose-containing solutions for initial correction - insulin release will drive K+ further into cells
Total daily IV limits:
- Adults: typically 100-200 mmol/day IV
- Higher amounts may be needed in severe/ongoing losses but require specialist (nephrology/ICU) oversight and pharmacy input
Monitoring During Treatment
- Serial serum K+ measurements (1-4 hourly in severe cases)
- ECG monitoring - watch for: U waves, T-wave flattening, ST depression, prolonged QU interval
- Urine output (renal function must be confirmed before giving K+)
- Serum Mg²+ - hypomagnesaemia perpetuates hypokalaemia and must be corrected simultaneously; K+ replacement will fail if Mg²+ is not replaced
- Avoid glucose-containing solutions
Special Situations
| Situation | Action |
|---|---|
| Digoxin therapy | Higher target K+ (3.5-5.0); even mild hypokalaemia potentiates toxicity |
| DKA | Replace K+ carefully; K+ shifts in with insulin - pre-empt fall |
| Hypokalemic periodic paralysis | Do NOT over-replace; deficit is transcellular, not real |
| Metabolic alkalosis | Use KCl specifically; treats both problems |
| Hypomagnesaemia | Correct Mg²+ first/concurrently |
| Prerenal azotaemia with hyperglycaemia | Volume expansion with NaCl alone can cause life-threatening K+ loss; must give K+ proactively |
Sources: Goldman-Cecil Medicine (9780323930345); NKF Primer on Kidney Diseases 8e (9780323791229); Henry's Clinical Diagnosis & Management by Laboratory Methods (9780323673204); NHS Grampian Acute Hypokalaemia Guideline 2024/2025; FDA KCl label
A patient of pot 1.2 meq/ litre with no diarr, vomitting, with no resp efforts then how to approach
Finding Sources
Searching the Web
severe hypokalemia 1.2 mEq respiratory failure management ICU potassium replacement emergency
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have all the information needed. This is a high-stakes clinical scenario - let me deliver a structured, step-by-step emergency approach.
Critical Clinical Scenario: K+ 1.2 mEq/L + No Respiratory Effort
This is a medical emergency. K+ of 1.2 mEq/L with absent respiratory effort = hypokalaemic respiratory paralysis with respiratory arrest. Resuscitation and potassium replacement must happen simultaneously.
Immediate Assessment (First 60 Seconds)
Why no respiratory effort?
At K+ < 2.0 mmol/L, flaccid paralysis involving the diaphragm and intercostal muscles can occur. This is hypokalaemic ascending neuromuscular paralysis - the cranial nerves are typically spared.
- No diarrhoea / no vomiting = GI loss excluded
- The cause is likely: renal loss, transcellular shift, or a disorder not yet identified
Step-by-Step Emergency Management
STEP 1 - Secure the Airway IMMEDIATELY
Call resuscitation team / code blue
- Bag-mask ventilate the patient right now
- Prepare for emergency endotracheal intubation (RSI)
- Connect to mechanical ventilation - the respiratory muscles will not recover until K+ is substantially corrected (this may take hours)
- Do NOT wait for labs before ventilating - airway first
STEP 2 - Monitoring (simultaneous with airway)
| Monitor | Reason |
|---|---|
| 12-lead ECG immediately | K+ 1.2 = extreme risk of VT / VF / torsades |
| Continuous cardiac monitoring (telemetry) | Mandatory throughout replacement |
| Pulse oximetry | Respiratory status |
| IV access x2 - at minimum one large bore peripheral | One for K+ infusion, one for resuscitation |
| Central venous catheter (internal jugular / subclavian / femoral) | Required for high-rate/high-concentration K+ replacement |
STEP 3 - Urgent Bloods
Draw before giving any treatment (do not delay resuscitation, but draw simultaneously):
| Test | Reason |
|---|---|
| Serum K+, Na+, Cl-, HCO3-, glucose | Confirm, check for metabolic alkalosis/acidosis |
| Serum Mg²+ | ~50% of severe hypokalaemia has concomitant hypomagnesaemia - must replace Mg²+ or K+ replacement will fail |
| Serum phosphate, calcium | Co-deficiencies |
| Urea, creatinine | Renal function before aggressive K+ replacement |
| ABG | Confirm respiratory failure, acid-base status |
| Urine K+ / urine creatinine (TTKG or spot urine K/Cr) | Determine if cause is renal vs extrarenal |
| Thyroid function (TSH) | Thyrotoxic hypokalemic paralysis if clinically relevant |
| Aldosterone / renin | If BP elevated and cause unknown |
| Serum CK | Rhabdomyolysis risk at K+ < 2.5 |
STEP 4 - Estimate the Potassium Deficit
For every 1 mEq/L fall in serum K+, body deficit = 200-400 mEq
Target: 4.0 mEq/L (in cardiac patients, or 3.5 mEq/L minimum)
K+ is 1.2 mEq/L, need to raise by ~2.8-3.0 mEq/L:
Estimated deficit = 2.8 × 200 to 2.8 × 400 = 560 to 1120 mEq total
This is a massive deficit. It will take multiple cycles of infusion over 12-24+ hours. You will not correct this in one go - nor should you attempt to.
Important: This formula overestimates in transcellular shift (e.g. periodic paralysis, thyrotoxic paralysis). Check the clinical picture and cause. Do not over-replace if shift is suspected.
STEP 5 - IV Potassium Replacement Protocol
Route: Central venous catheter is mandatory at this level of severity and infusion rate.
| Phase | Rate | Concentration | Setting | Notes |
|---|---|---|---|---|
| Emergency (first 1-2 hrs) | 20-40 mmol/hr | KCl in 0.9% NaCl (NOT glucose) | ICU, continuous ECG | Max 40 mmol/hr via central line only |
| Ongoing replacement | 10-20 mmol/hr | KCl 20-40 mmol in 500 mL NaCl 0.9% | ICU/HDU | After K+ > 2.5 |
| Maintenance/fine-tuning | 10 mmol/hr | Peripheral acceptable | HDU/monitored ward | When K+ > 3.0 |
Key rules:
- Use 0.9% NaCl as the vehicle - NEVER glucose (glucose triggers insulin release, which drives K+ into cells and worsens hypokalaemia)
- Concentration > 60 mmol/L = central line only
- Peripheral veins can safely receive up to 40 mmol/L at max 10 mmol/hr
Recheck serum K+ every 1-2 hours in ICU and adjust dose accordingly.
STEP 6 - Correct Magnesium Simultaneously
~50% of patients with severe hypokalaemia have hypomagnesaemia. Potassium replacement is refractory until Mg²+ is replete. Magnesium is an essential cofactor for K+ uptake into cells.
- Magnesium sulphate 2g (8 mmol) IV over 15-30 mins, then consider infusion if Mg²+ is low
- Even if you don't have the Mg²+ result yet, empiric Mg²+ replacement is reasonable in this setting
- Also reduces arrhythmia risk independently
STEP 7 - ECG Monitoring and Arrhythmia Management
Hypokalaemia ECG changes (in order of worsening K+):
| K+ level | ECG findings |
|---|---|
| 3.0-3.5 | T-wave flattening, mild U waves |
| 2.5-3.0 | Prominent U waves, U > T in V2-V3 |
| < 2.5 | ST depression, prolonged QU interval |
| < 1.5 | Widened QRS, P-wave changes, VT, torsades de pointes, VF |
If torsades de pointes develops:
- MgSO4 2g IV bolus immediately
- Defibrillate if pulseless VF
- Overdrive pacing if recurrent torsades
- Continue aggressive K+ replacement
- Avoid drugs that prolong QT (class IA, IC, III antiarrhythmics)
STEP 8 - Find the Underlying Cause
No vomiting, no diarrhoea, no obvious GI loss - the differential now shifts to:
No GI cause → Think:
├── Renal K+ wasting (most common)
│ ├── Diuretics (loop/thiazide) — check medication list
│ ├── Primary hyperaldosteronism
│ ├── Bartter / Gitelman syndrome
│ ├── RTA type 1 or 2
│ └── Hypomagnesaemia-induced renal wasting
├── Transcellular shift (no true deficit)
│ ├── Insulin excess / glucose load
│ ├── Beta-2 agonist (salbutamol, bronchodilators)
│ ├── Thyrotoxic hypokalemic paralysis
│ ├── Familial hypokalemic periodic paralysis
│ └── Barium / hydroxychloroquine toxicity
├── Excess mineralocorticoid activity
│ ├── Cushing syndrome / exogenous steroids
│ └── Liquorice / carbenoxolone / chewing tobacco
└── Rare: prolonged starvation + catabolism
Urine K+ interpretation:
- Urine K+ < 20 mEq/L (or TTKG < 2) = extrarenal loss or transcellular shift
- Urine K+ > 40 mEq/L (or TTKG > 4) = renal K+ wasting (diuretics, hyperaldosteronism, Bartter, RTA)
STEP 9 - ICU Care and Ongoing Monitoring
| Parameter | Frequency |
|---|---|
| Serum K+ | Every 1-2 hours initially, then 4-hourly |
| Serum Mg²+ | Every 4-6 hours |
| Urine output | Hourly (foley catheter) |
| ECG / telemetry | Continuous |
| ABG | As needed for ventilator management |
| Recheck cause | Once K+ stabilised above 3.0 |
Target K+ = 4.0 mEq/L in this critically ill patient (higher target reduces arrhythmia risk, especially if on digoxin or if cardiac disease).
Summary Card
K+ 1.2 mEq/L + No respiratory effort
1. AIRWAY → Bag-mask → RSI → Mechanically ventilate
2. ACCESS → 2x IV (large bore) + Central venous catheter
3. MONITOR → Continuous ECG + cardiac telemetry
4. BLOODS → K+, Mg²+, phosphate, Ca²+, ABG, renal function, urine K+
5. REPLACE → KCl 20-40 mmol/hr via central line in 0.9% NaCl
6. Mg²+ → MgSO4 2g IV empirically → prevents refractory hypoK
7. AVOID → Glucose solutions, drugs prolonging QT
8. RECHECK → K+ every 1-2 hours, adjust infusion
9. CAUSE → Find it (urine K+, aldosterone/renin, TFTs, medication review)
10. WEAN VENT → Only after K+ > 3.0 and neuromuscular function recovering
Sources: Sabiston Textbook of Surgery 8e (9780443124341); Rosen's Emergency Medicine (9780323757898); Goldman-Cecil Medicine (9780323930345); RECAPEM Hypokalemia Emergency Protocol; Medscape Hypokalemia Treatment Guidelines
Patient ca and mg are wnl, airway secured, central line given …ryles tube given how. Much correction to be given
Finding Sources
Finding Sources
Finding Sources
Searching the Web
severe hypokalemia 1.2 combined IV and enteral nasogastric potassium correction protocol ICU rate total dose
Reading File
Reading File
I have all the data needed. Here is the precise correction plan for this specific scenario.
Correction Protocol: K+ 1.2 mEq/L | Central Line + Ryle's Tube | Ca²+/Mg²+ Normal
Recap of the Deficit
| Parameter | Value |
|---|---|
| Current K+ | 1.2 mEq/L |
| Target K+ | 4.0 mEq/L (critically ill patient, ventilated) |
| Gap to close | 2.8 mEq/L |
| Estimated deficit | 2.8 × 200 to 2.8 × 400 = 560 to 1120 mEq |
Use 800 mEq as your working estimate (midpoint). You will not give all of this at once - it is given in phases over 24-48 hours, guided by serial K+ levels every 1-2 hours.
Phase 1 - Emergency IV Correction via Central Line (Hours 0-2)
Goal: Raise K+ above 2.5 mEq/L and terminate arrhythmia risk as fast as safely possible.
IV KCl infusion via central line:
| Parameter | Value |
|---|---|
| Rate | 20-40 mmol/hr via central line |
| Concentration | KCl 40 mmol in 100 mL of 0.9% NaCl (= 400 mmol/L) |
| Vehicle | 0.9% NaCl ONLY - never glucose |
| Duration of phase 1 | 2 hours |
| Total given in phase 1 | 80 mmol (at 40 mmol/hr x 2 hrs) |
| Monitoring | Continuous ECG, recheck serum K+ at 1 hr and 2 hrs |
40 mmol/hr is the absolute maximum rate ever used - only justified here because K+ = 1.2 with respiratory arrest. This rate requires ICU, continuous cardiac monitoring, and nurse 1:1.
Check K+ at 1 hour. If K+ has risen to > 2.0 and no arrhythmia → step down to 20 mmol/hr.
Phase 2 - Dual Route: IV + Enteral via Ryle's Tube (Hours 2-12)
Now that the Ryle's tube is in place, you can run both routes simultaneously - this is safe and recommended. Oral/enteral potassium is well absorbed from the GI tract and using both routes speeds up total body repletion while allowing the IV rate to be reduced.
IV (central line) - reduced rate:
| Parameter | Value |
|---|---|
| Rate | 20 mmol/hr |
| Concentration | 40 mmol in 250 mL 0.9% NaCl (= 160 mmol/L) |
| Duration | Until K+ > 3.0 mEq/L |
| Total over 10 hrs | ~200 mmol |
Enteral via Ryle's tube (simultaneous):
| Parameter | Value |
|---|---|
| Agent | KCl oral solution / syrup (or crushed KCl effervescent tablets dissolved in water) |
| Dose per administration | 40 mmol (40 mEq) per dose via NG tube |
| Frequency | Every 4-6 hours |
| Daily enteral dose | 100-200 mmol/day via NG |
| Flush | Flush tube with 30 mL water after each dose |
Oral/enteral potassium has a safety advantage: the GI mucosa absorbs it more slowly than IV, buffering against sudden surges. Using both routes gives faster total repletion without exceeding safe IV rates.
Phase 3 - Maintenance Correction (Hours 12-48)
Once K+ > 3.0:
| Route | Dose | Notes |
|---|---|---|
| IV (central or peripheral) | 10-20 mmol/hr, 40 mmol in 500 mL 0.9% NaCl | Step down further as K+ rises |
| Enteral (NG) | 40-60 mmol every 6 hours | Continue until oral intake possible |
| Total daily target | 120-200 mmol/day combined | Titrate to serial K+ |
Hour-by-Hour Summary Table
| Time | IV Rate | Enteral Dose | Expected K+ Rise | Action |
|---|---|---|---|---|
| 0-1 hr | 40 mmol/hr | Nil | +0.3-0.5 | Check K+ at 1 hr |
| 1-2 hr | 20-40 mmol/hr | Nil | +0.3-0.5 | Check K+ at 2 hr |
| 2-6 hr | 20 mmol/hr | 40 mmol via NG | +0.5-0.8 | Check K+ at 4 hr |
| 6-12 hr | 20 mmol/hr | 40 mmol via NG q6h | +0.5-1.0 | Check K+ at 8 hr, 12 hr |
| 12-24 hr | 10-20 mmol/hr | 40-60 mmol q6h | +0.5-1.0 | Titrate to serial K+ |
| 24-48 hr | 10 mmol/hr or less | 40 mmol q6h | Maintain 3.5-4.5 | Wean IV, continue enteral |
Expected total K+ correction time: 24-48 hours to reach and sustain 4.0 mEq/L. Replenishing intracellular stores takes days even after serum K+ normalises.
Critical Rules for This Patient
| Rule | Reason |
|---|---|
| Never exceed 40 mmol/hr IV | Risk of cardiac arrest from hyperkalemia |
| Never use glucose solution as vehicle | Insulin response will worsen hypokalemia |
| Check K+ every 1-2 hrs in ICU | Serum level can overshoot - hyperkalemia is equally dangerous |
| Count ALL sources of K+ | IV + NG + any K+ in maintenance fluids + TPN if running |
| Do not correct too fast if periodic paralysis suspected | Transcellular shift, not true deficit |
| Keep urine output > 0.5 mL/kg/hr | K+ replacement requires adequate renal function to be safe |
| Do not start ventilator weaning until K+ > 3.0 and neuromuscular function recovering |
When to Recheck and When to Stop IV K+
| K+ Level | Action |
|---|---|
| < 2.0 | Max rate 40 mmol/hr IV, continuous ECG |
| 2.0-2.5 | Reduce IV to 20 mmol/hr, continue NG |
| 2.5-3.0 | IV 10-20 mmol/hr + NG 40 mmol q6h |
| 3.0-3.5 | IV 10 mmol/hr or peripheral, NG continue |
| > 3.5 | Stop IV, maintain on NG only |
| > 4.5 | Stop all K+ immediately, recheck in 1 hr |
Quick Summary
K+ 1.2 | Central line + Ryle's tube | Ca, Mg normal
PHASE 1 (0-2h): IV 40 mmol/hr via central (KCl in 0.9% NaCl)
Recheck K+ at 1h and 2h
PHASE 2 (2-12h): IV 20 mmol/hr via central
+ NG 40 mmol q6h via Ryle's tube
Recheck K+ every 2-4 hrs
PHASE 3 (12-48h): IV 10 mmol/hr (step down)
+ NG 40-60 mmol q6h
Target K+ = 4.0 mEq/L
TOTAL estimated: 600-1000 mmol over 24-48 hrs
MAX safe IV rate: 40 mmol/hr (central only, continuous ECG)
VEHICLE: 0.9% NaCl ALWAYS — never glucose
Sources: Sabiston Textbook of Surgery 8e; Goldman-Cecil Medicine 2025; StatPearls NIH Potassium; Medscape Hypokalemia Treatment Guidelines
Make a ppt of it
Reading File
Reading File
Reading File
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
The patient is not on diutectics how to find cause
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.