Why obstructive jaundice in chronic pancreatitis
Reading File
Finding Sources
Finding Sources
Searching PubMed
obstructive jaundice chronic pancreatitis bile duct stricture
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, well-cited answer. Here it is:
Obstructive Jaundice in Chronic Pancreatitis
Obstructive jaundice occurs in chronic pancreatitis through several distinct but overlapping mechanisms, all ultimately involving the intrapancreatic portion of the common bile duct (CBD), which runs through a groove in the posterior surface of the pancreatic head before entering the duodenum at the ampulla of Vater.
1. Encasing Fibrosis of the Pancreatic Head (Most Common Mechanism)
The hallmark of chronic pancreatitis is progressive parenchymal destruction replaced by dense fibrosis. When this fibrosing process involves the head of the pancreas, it directly encases and compresses the distal CBD, forming a biliary stricture.
"The fibrosing process within the pancreatic head can encase the distal bile duct and result in formation of a biliary stricture."
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
"Elevation of serum bilirubin and alkaline phosphatase may indicate cholestasis secondary to common bile duct stricture caused by chronic inflammation or fibrosis."
- Harrison's Principles of Internal Medicine 22E
"In chronic pancreatitis, compression of the duct occurs as a result of encroaching pancreatic fibrosis."
- Frameworks for Internal Medicine
The stricture produced by fibrosis is typically long-segment, smooth, and located in the distal CBD (intrapancreatic segment). Calcific chronic pancreatitis responds less well to dilation than non-calcific disease.
2. Extrinsic Compression by a Pseudocyst
Pancreatic pseudocysts - fluid collections enclosed by fibrous walls - can form in the head or uncinate region and directly compress the CBD from outside, producing extrahepatic biliary obstruction.
"Pseudocysts can also cause extrahepatic biliary obstruction from extrinsic common bile duct obstruction."
- Frameworks for Internal Medicine
The CT image below shows a classic case: a large pseudocyst (P) in the pancreatic head compressing both the CBD (curved arrow) and the duodenum (straight arrow), with a distended gallbladder (G) confirming obstruction:
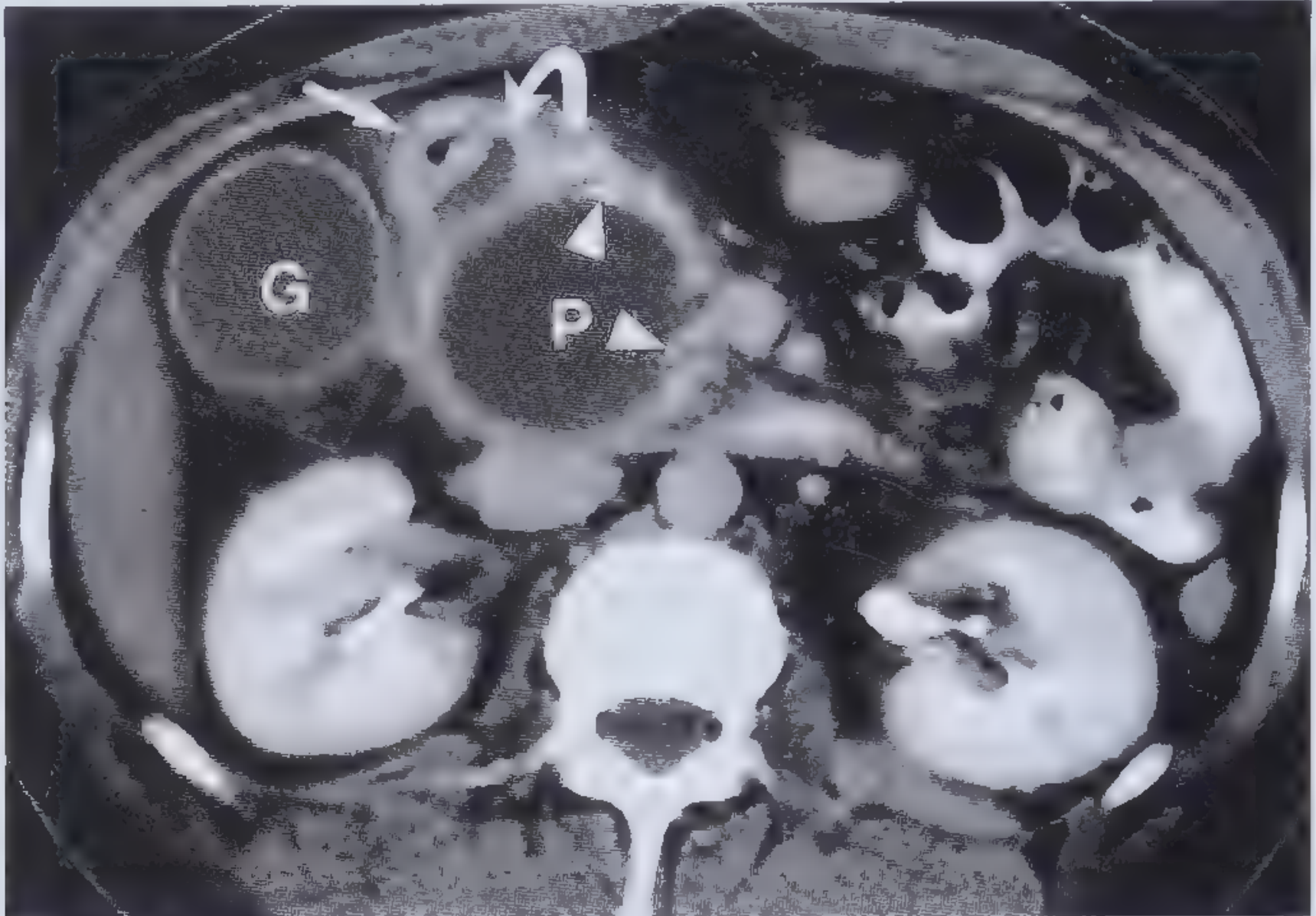
Pancreatic pseudocyst (P) compressing the CBD (curved arrow) and duodenum (straight arrow), with distended gallbladder (G). Small calcifications (arrowheads) confirm underlying chronic pancreatitis.
3. Acute-on-Chronic Exacerbation: Edema Superimposed on a Partial Stricture
In patients with an already narrowed CBD from progressive fibrosis, a flare of acute pancreatitis (superimposed on chronic) causes tissue edema that further compromises the already-narrowed duct, precipitating frank obstructive jaundice.
"Patients with chronic pancreatitis often experience recurrent cholestasis during episodes of acute pancreatitis when a partially compressed duct becomes further compromised by tissue edema."
- Frameworks for Internal Medicine
This explains why some patients with chronic pancreatitis have episodic, recurrent jaundice rather than persistent jaundice.
4. Inflammatory Mass in the Pancreatic Head ("Inflammatory Pseudotumor")
Severe chronic pancreatitis, particularly alcoholic pancreatitis, can produce a focal inflammatory mass in the head of the pancreas that is indistinguishable from carcinoma on imaging. This mass can compress the CBD just as a tumor would. Distinguishing it from pancreatic adenocarcinoma is one of the most clinically important challenges in this setting.
"The most common cause of this form of obstructive jaundice is carcinoma of the head of the pancreas. Biliary obstruction may also occur as a complication of either acute or chronic pancreatitis..."
- Harrison's Principles of Internal Medicine 22E
Summary Table
| Mechanism | Pathological Basis | Pattern of Jaundice |
|---|---|---|
| Fibrotic encasement of distal CBD | Progressive pancreatic head fibrosis | Persistent, progressive cholestasis |
| Pseudocyst compressing CBD | Fluid collection in pancreatic head/uncinate | Acute onset, often with pain |
| Acute-on-chronic edema | Flare superimposed on partial fibrotic stricture | Episodic, recurrent cholestasis |
| Inflammatory mass (pseudotumor) | Focal inflammatory enlargement of head | Mimics malignant obstruction |
Consequences and Management
Untreated biliary obstruction from chronic pancreatitis can progress to:
- Secondary biliary cirrhosis and portal hypertension (which can develop within months in alcohol-related chronic pancreatitis)
- Ascending cholangitis
Management options include:
- Endoscopic stenting - multiple side-by-side plastic stents or fully covered self-expandable metal stents (SEMS); up to 80% stricture resolution with covered SEMS at 3-6 months
- Surgery - biliary bypass (hepaticojejunostomy or choledochoduodenostomy) recommended for persistent cholestasis unresponsive to endoscopic therapy; preferred for calcific disease
- Pseudocyst drainage - endoscopic, radiologic, or surgical, when the pseudocyst is the compressing lesion
Sources: Frameworks for Internal Medicine, p. 184; Sleisenger & Fordtran's GI and Liver Disease (Biliary Strictures); Harrison's 22E (Extrinsic Compression of Bile Ducts, p. 212); Robbins & Kumar Basic Pathology; Clinical GI Endoscopy 3e
This is a shared conversation. Sign in to Orris to start your own chat.