Sudden and gradual painless and painful loss of vision - ophthalmology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have rich content from Kanski's, Tintinalli, Bailey & Love, and Goldman-Cecil. Let me compile the comprehensive answer.
Loss of Vision - A Systematic Ophthalmology Overview
Loss of vision is classified along two axes: onset (sudden vs. gradual) and pain (painful vs. painless). This 2x2 framework is the most practical clinical approach.
Framework: The 4 Categories
| Painless | Painful | |
|---|---|---|
| Sudden | CRAO, CRVO, Retinal detachment, Vitreous haemorrhage, AION (non-arteritic) | Acute angle-closure glaucoma, Optic neuritis, Uveitis, GCA (arteritic AION) |
| Gradual | Cataract, Glaucoma, Diabetic retinopathy, AMD, Macular hole | Optic neuritis (subacute), Orbital/intracranial tumour |
A. SUDDEN PAINLESS LOSS OF VISION
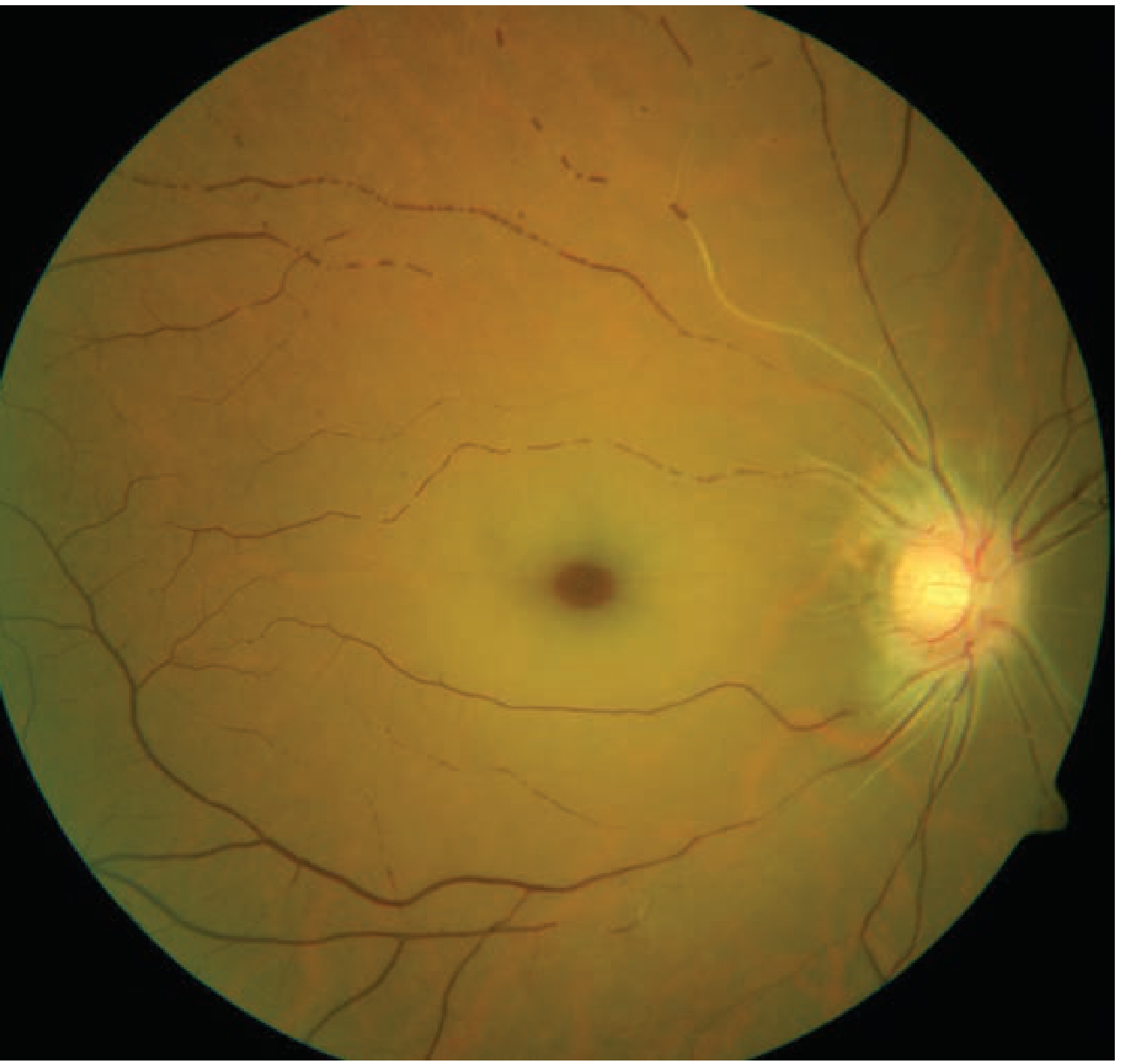
1. Central Retinal Artery Occlusion (CRAO)
Presentation: Sudden, profound, monocular, painless loss of vision. Pain may be present only in Giant Cell Arteritis (GCA)-related CRAO.
Pathophysiology: Occlusion of the central retinal artery (first branch of the ophthalmic artery) causes inner retinal infarction. The inner retina becomes pale, opaque, and oedematous. Because the macula (fovea) is the thinnest retinal region, the intact underlying choroidal circulation remains visible through it, creating the classic "cherry-red spot".
Signs:
- Severely reduced VA (may be perception of hand movements only)
- Profound RAPD (afferent pupillary defect), sometimes a complete amaurotic pupil
- Pale/white retinal oedema across all quadrants
- Cherry-red spot at macula
- Attenuated retinal arteries; "cattle-trucking" or "box-car" blood column segmentation
- Emboli visible in ~20%
- Rubeosis iridis (neovascularization of iris) may develop in ~20%, typically at 4-5 weeks
Cherry-red spot on fundoscopy (CRAO):
Causes: Carotid/cardiac embolus, thrombosis, GCA, vasculitis (SLE, PAN), sickle cell, trauma, vasospasm.
Investigation: FA (delayed arterial filling), ERG (diminished b-wave), OCT (hyperreflective embolic plaque at optic nerve head), carotid Doppler, echocardiography.
Treatment: Ophthalmic emergency - irreversible damage may occur within ~4 hours.
- Ocular massage (to dislodge emboli)
- IOP-lowering (topical beta-blocker, IV acetazolamide)
- Paracentesis of anterior chamber
- Nd:YAG embolysis (if embolus visible)
- Urgent systemic workup for stroke risk (same urgency as TIA)
- If GCA suspected: immediate high-dose IV methylprednisolone
- Kanski's Clinical Ophthalmology 10th ed., pp. 551-554; Tintinalli's Emergency Medicine, p. 1596
2. Branch Retinal Artery Occlusion (BRAO)
Presentation: Sudden painless altitudinal or sectoral visual field loss. May go unnoticed if central vision is spared.
Signs:
- Segmental pale retinal oedema ("ground glass" appearance) corresponding to ischaemic area
- Embolus often visible at arterial bifurcation point
- FA shows delayed filling and hypofluorescence of the involved segment
- Affected artery remains attenuated; visual field defect rarely recovers
- Kanski's Clinical Ophthalmology 10th ed., p. 551
3. Central Retinal Vein Occlusion (CRVO)
Presentation: Variable painless monocular vision loss, from mild blurring to sudden severe loss.
Risk factors: Hypertension, diabetes, dyslipidaemia, cardiovascular disease, hypercoagulable states, glaucoma, vasculitis.
Classic fundus appearance - "Blood-and-thunder fundus":
- Disc oedema
- Diffuse retinal haemorrhages in all four quadrants (flame-shaped superficial and deep dot/blot)
- Dilated, tortuous veins
- Cotton-wool spots possible

Distinguishing from papilloedema: The contralateral optic nerve is normal in CRVO; in papilloedema both discs are affected.
Complications: Neovascularization (NVI/NVD), neovascular glaucoma (rubeosis iridis develops in up to 90% of ischaemic CRVO), macular oedema.
Treatment: Anti-VEGF agents (intravitreal) for macular oedema; laser photocoagulation; systemic risk factor management.
- Tintinalli's Emergency Medicine, p. 1597; Kanski's Clinical Ophthalmology 10th ed.
4. Transient Monocular Vision Loss / Amaurosis Fugax
Presentation: Transient painless monocular loss of vision, classically described as "a curtain coming down over the eye." Lasts minutes; recovery usually more gradual than onset.
Causes (Goldman-Cecil classification):
| Category | Duration | Common Causes |
|---|---|---|
| Thromboembolism | 1-5 min | Carotid atherosclerosis, cardiac (AF, valvular), blood dyscrasias |
| Vasospasm | 5-30 min | Migraine |
| Vascular compression | Few seconds | Raised ICP (plateau waves), orbital tumour |
| Vasculitis | 1-5 min | Temporal arteritis (GCA) |
Importance: Embolic amaurosis fugax carries the same stroke risk as a cerebral TIA and must be investigated urgently (carotid imaging, echocardiography, FBC, lipids, ESR/CRP).
- Kanski's Clinical Ophthalmology 10th ed., p. 551; Goldman-Cecil Medicine, Table 392-1
5. Rhegmatogenous Retinal Detachment (RD)
Presentation: Gradual/sudden, painless monocular vision loss, often preceded by:
- Floaters (sudden increase - usually pigment "tobacco dust" or blood)
- Photopsia (flashing lights - due to vitreoretinal traction, typically at the periphery)
- Then a curtain-like peripheral visual field defect that can progress to involve central vision
The field defect may be absent in the morning (subretinal fluid reabsorbs overnight when supine) but returns later in the day.
Pathophysiology: Liquefied vitreous passes through a retinal break and accumulates under the neurosensory retina, separating it from the RPE. >40% of RDs occur in myopic eyes.
Signs:
- RAPD (if extensive)
- IOP lower than the fellow eye (~5 mmHg)
- "Tobacco dust" (Shafer's sign) - pigment cells in anterior vitreous
- Retinal break(s) - red discontinuities in retinal surface
Lincoff's Rules for break location (Modified):
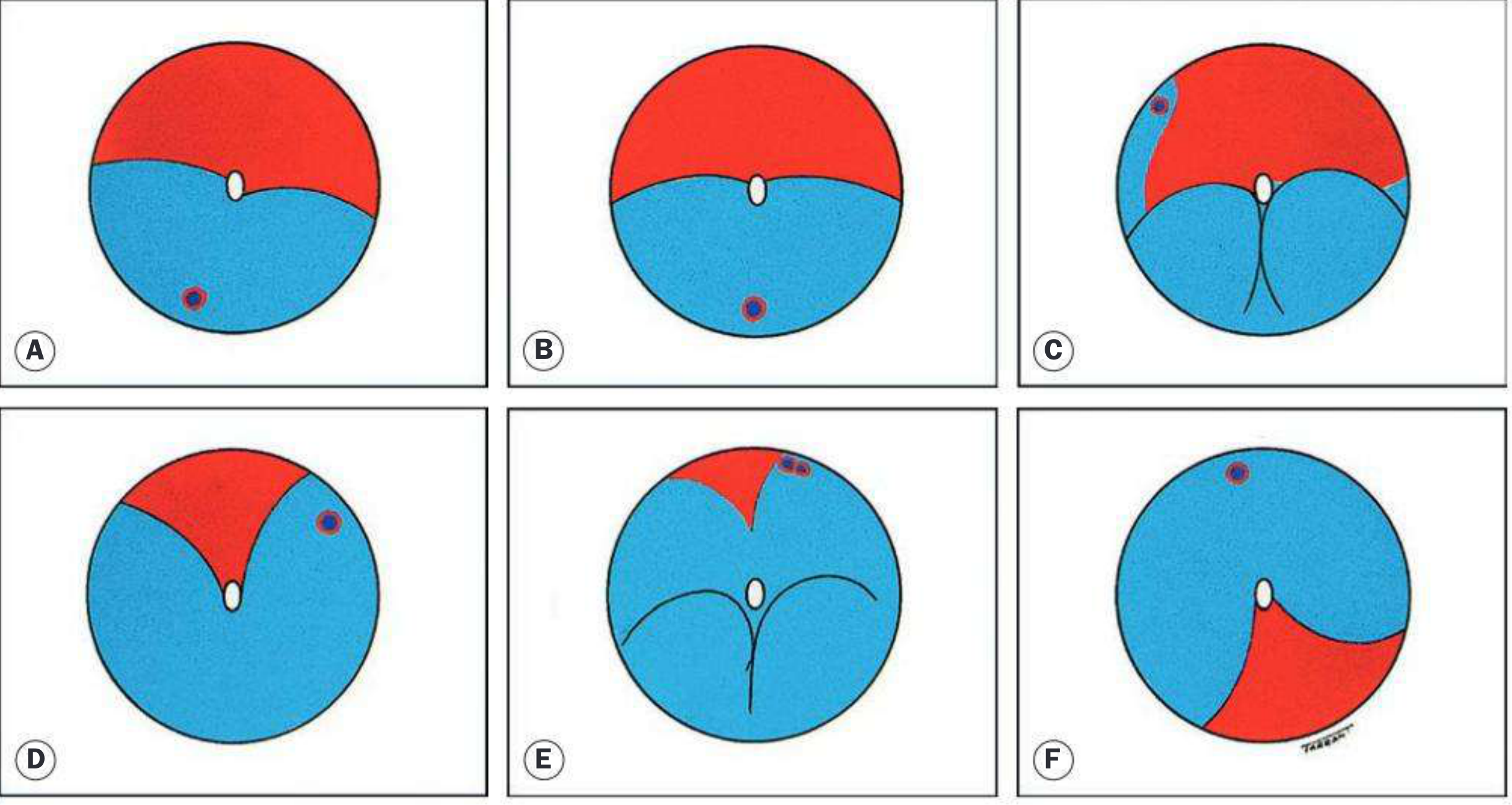
- SRF higher on temporal side → inferotemporal break (A)
- SRF at equal level inferiorly → 6 o'clock break (B)
- Bullous inferior RD → break above horizontal meridian (C)
- Upper nasal quadrant SRF revolves around disc → upper nasal break (D)
Break distribution: ~60% superotemporal, 15% superonasal, 15% inferotemporal, 10% inferonasal.
Treatment: Surgical - scleral buckling, pneumatic retinopexy, or vitrectomy (depending on break location and complexity).
- Kanski's Clinical Ophthalmology 10th ed., pp. 695-696
6. Vitreous Haemorrhage
Presentation: Sudden painless blurring or complete vision loss, often with floaters and dark shadows. Vision loss is proportional to the density of haemorrhage.
Causes: Proliferative diabetic retinopathy (most common), retinal tear/detachment, trauma, BRVO, valsalva retinopathy, subarachnoid haemorrhage (Terson syndrome).
Management: Urgent B-scan ultrasound to rule out underlying retinal detachment. Observe if no RD; vitrectomy if haemorrhage fails to clear.
B. SUDDEN PAINFUL LOSS OF VISION
1. Acute Angle-Closure Glaucoma (AACG)
Presentation: Sudden painful vision loss, typically in older hypermetropic patients. More prevalent in Asian populations.
Classic features:
- Severe unilateral ocular pain, often with nausea and vomiting (can mimic acute abdomen)
- Hazy/steamy cornea (corneal oedema due to raised IOP)
- Fixed, mid-dilated, oval, non-reactive pupil
- Conjunctival hyperaemia (ciliary injection)
- Vision markedly reduced
- Rock-hard eye on palpation
Pathophysiology: Pupil block causes aqueous humour to accumulate behind the iris, pushing the peripheral iris forwards and closing the iridocorneal angle, blocking aqueous outflow.
Diagnosis: Tonometry (IOP often >40 mmHg), gonioscopy.
Treatment (urgent):
- Topical pilocarpine (to constrict pupil and open angle)
- Oral/IV acetazolamide (carbonic anhydrase inhibitor)
- IV mannitol if refractory
- Definitive: Nd:YAG laser iridotomy (prophylactic iridotomy in the fellow eye simultaneously, as the condition is usually bilateral in predisposition)
- Bailey & Love's Short Practice of Surgery 28th ed., p. 6247
2. Optic Neuritis
Presentation: Subacute painful monocular vision loss developing over days (occasionally hours). Pain with eye movement is present in 19-92% of cases.
Features:
- VA ranges from mild reduction to no light perception
- Colour vision disproportionately impaired (red desaturation test positive)
- RAPD present
- Visual field defects (central scotoma common)
- Fundus: swollen optic disc (papillitis) in ~30%; normal disc (retrobulbar neuritis) in ~70%
- Pain on eye movement is a key distinguishing feature from AION
Causes: Most commonly demyelinating (MS - up to 50% develop MS within 15 years); also post-viral (measles, mumps, VZV), syphilis, TB, sarcoidosis, cryptococcus.
DDx from AION: AION is sudden onset and painless; optic neuritis has pain and subacute onset.
Treatment: High-dose IV methylprednisolone (1g/day × 3 days) speeds recovery but does not improve final visual outcome; prognosticated by MRI (number of white matter lesions).
- Tintinalli's Emergency Medicine, p. 1596
3. Anterior Ischaemic Optic Neuropathy (AION)
| Non-Arteritic (NAION) | Arteritic (AAION - GCA) | |
|---|---|---|
| Onset | Sudden, painless | Sudden; may have headache, jaw claudication |
| Age | 40-60 | >60 (usually >70) |
| Cause | Small vessel disease, sleep apnoea, nocturnal hypotension | Giant cell arteritis |
| Disc | Segmental pallid oedema | Chalky-white disc oedema |
| Vision | Altitudinal field defect | Severe loss, can progress to NLP |
| ESR/CRP | Normal | Markedly elevated (ESR 70-110 mm/hr) |
| Other symptoms | None | PMR, temporal artery tenderness, jaw claudication |
| Treatment | No proven treatment | Immediate high-dose steroids (IV methylprednisolone 500-1000 mg/day × 3 days) to protect the fellow eye |
GCA (temporal arteritis) is a medical emergency - steroids must NOT be delayed while awaiting temporal artery biopsy (biopsy within 1 week of starting steroids is still diagnostic).
- Tintinalli's Emergency Medicine, p. 1597; Kanski's Clinical Ophthalmology 10th ed.
C. GRADUAL PAINLESS LOSS OF VISION
1. Cataract
Presentation: Progressive, bilateral (though often asymmetric) painless blurring. Typical complaints: glare, haloes, monocular diplopia, colour desaturation, reduced contrast.
Types: Nuclear sclerosis (commonest), posterior subcapsular (worst VA in bright light), anterior cortical.
Treatment: Surgical - phacoemulsification with IOL implantation.
2. Chronic Open-Angle Glaucoma (COAG)
Presentation: Insidious, typically bilateral, painless peripheral visual field loss. Patients are often unaware until the disease is advanced ("silent thief of sight").
Key features:
- Raised IOP (>21 mmHg) in most, but normal-tension glaucoma exists
- Characteristic optic disc cupping (increased cup:disc ratio >0.6)
- RNFL thinning on OCT
- Arcuate/altitudinal field defects on perimetry
Treatment: Prostaglandin analogue eye drops first-line (latanoprost); laser trabeculoplasty; trabeculectomy.
3. Age-Related Macular Degeneration (AMD)
Dry AMD: Slow progressive central vision loss. Drusen and RPE atrophy. No treatment restores lost vision; AREDS2 supplements may slow progression.
Wet (Neovascular) AMD: Faster-onset central vision loss due to choroidal neovascularization (CNV) leaking fluid under the retina. Presents with metamorphopsia (distorted vision), central scotoma.
Risk factors: Advanced age, hyperopia, blue eyes, family history, soft drusen, smoking, hypertension.
OCT findings: Sub-RPE fluid (Type 1/occult CNV), sub-neurosensory fluid (Type 2/classic CNV).
Treatment for wet AMD: Intravitreal anti-VEGF injections (ranibizumab, bevacizumab, aflibercept, faricimab) are the mainstay.
4. Diabetic Retinopathy
Presentation: Gradual painless bilateral visual loss. Vision loss may be sudden if vitreous haemorrhage occurs in proliferative DR.
Stages:
- Non-proliferative DR (NPDR): microaneurysms, dot/blot haemorrhages, hard exudates, cotton-wool spots
- Proliferative DR (PDR): neovascularization (NVD/NVE), vitreous haemorrhage, tractional retinal detachment
- Diabetic maculopathy: macular oedema (commonest cause of visual impairment in DR)
Treatment: Tight glycaemic/BP control; intravitreal anti-VEGF or laser for macular oedema; PRP (panretinal photocoagulation) for PDR; vitrectomy for non-clearing haemorrhage or tractional RD.
Quick Reference Summary Table
| Condition | Onset | Pain | Laterality | Key Feature | Emergency? |
|---|---|---|---|---|---|
| CRAO | Sudden | No (except GCA) | Unilateral | Cherry-red spot | Yes |
| BRAO | Sudden | No | Unilateral | Sector field loss, visible embolus | Yes |
| CRVO | Sudden | No | Unilateral | "Blood-and-thunder" fundus | Yes |
| Amaurosis fugax | Transient | No | Unilateral | "Curtain" lasts minutes | Yes (stroke risk) |
| Retinal detachment | Sudden/gradual | No | Unilateral | Floaters + curtain field defect | Yes |
| Vitreous haemorrhage | Sudden | No | Unilateral | Dark floaters, obscured fundus | Yes |
| Acute angle closure | Sudden | Severe | Unilateral | Hard red eye, fixed oval pupil | Yes |
| Optic neuritis | Subacute (days) | Yes (on movement) | Usually unilateral | RAPD, colour loss, MS association | Yes |
| NAION | Sudden | No | Unilateral | Altitudinal field loss, small disc | Yes |
| AAION (GCA) | Sudden | Headache | Unilateral/bilateral | Elevated ESR, jaw claudication | Yes |
| Cataract | Gradual | No | Bilateral | Glare, reduced contrast | No |
| Glaucoma (COAG) | Gradual | No | Bilateral | Peripheral field loss, cupping | No |
| AMD (dry) | Gradual | No | Bilateral | Central loss, drusen | No |
| AMD (wet) | Faster | No | Bilateral | Metamorphopsia, CNV on OCTA | Urgent |
| Diabetic retinopathy | Gradual | No | Bilateral | Microaneurysms, exudates | Urgent |
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed. | Tintinalli's Emergency Medicine, 9th ed. | Goldman-Cecil Medicine, Table 392-1 | Bailey & Love's Short Practice of Surgery, 28th ed.
This is a shared conversation. Sign in to Orris to start your own chat.