Basis of phantom limb Notes for mbbs 1st year physiology
Reading File
Finding Sources
Finding Sources
Searching the Web
phantom limb sensation mechanism physiology MBBS notes
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive content from multiple authoritative sources. Let me compile the full MBBS 1st year physiology notes:
Phantom Limb - MBBS 1st Year Physiology Notes
1. Definition
Phantom limb is the perception of sensations (including pain) arising from a body part that has been amputated or is no longer present. The term "phantom" refers only to the missing limb - the sensations themselves are very real to the patient.
- First described by French military surgeon Ambroise Paré (1551): "the patients, long after the amputation is made, say they still feel pain in the amputated part. Of this they complain strongly, a thing worthy of wonder and almost incredible to people who have not experienced this."
- Incidence: 50-80% of all amputees experience phantom sensations.
2. Types of Phantom Phenomena
| Type | Description |
|---|---|
| Phantom limb sensation | Non-painful sensations - tingling, warmth, cold, movement, numbness |
| Phantom limb pain (PLP) | Painful perception in the absent limb - stabbing, throbbing, burning, or cramping |
| Stump pain | Pain at the residual limb (amputation site) - may coexist with PLP |
| Telescoping | Feeling that the phantom limb is "retracting" toward the stump and shrinking; seen in ~30% of amputees |
Phantom phenomena are not limited to limbs. They also occur after removal of the breast, eye (phantom eye syndrome), tooth (phantom tooth pain), rectum, penis, and tongue.
3. Predisposing Factors
- Pre-amputation chronic pain in the limb (the strongest predictor - pain is often similar in character to the pre-existing pain)
- More intense in the distal portions of the phantom
- Exacerbated by emotional stress, changes in weather, pressure on the stump
- Less social support and catastrophizing worsen PLP
4. Pathophysiological Basis (Theories)
Phantom limb is explained by mechanisms at multiple levels of the neuroaxis. These theories are not mutually exclusive and likely operate together.
A. Peripheral Mechanism (Neuroma Theory)
- After amputation, cut nerve endings form neuromas (tangled, disorganized regenerating axons) at the stump
- Neuromas fire spontaneously and ectopically, sending abnormal sensory impulses centrally
- These abnormal inputs are misinterpreted by the brain as coming from the (now absent) limb
- Explains stump pain well, but cannot fully explain central phantom sensations after nerve section
B. Spinal Cord (Central Sensitization) Mechanism
- Amputation deprives dorsal horn neurons of their normal afferent input
- This leads to:
- Increased excitability of dorsal horn neurons (central sensitization)
- Reduction of inhibitory processes (loss of GABAergic and glycinergic inhibition)
- Structural changes at the central nerve endings of primary sensory neurons, interneurons, and projection neurons
- The "unmasked" hyperexcitable spinal neurons misinterpret residual/adjacent inputs as coming from the amputated limb
- Mechanism similar to wind-up and central sensitization seen in other chronic pain states
C. Supraspinal (Cortical Reorganization) - THE KEY MECHANISM for MBBS
This is the most important and widely accepted theory.
The somatosensory cortex is organized as a somatotopic map (Penfield's homunculus). When a limb is amputated:
- The cortical area that previously received input from the amputated limb is deprived of its normal sensory input
- Adjacent cortical areas (especially the mouth/face representation, which is adjacent to the hand area on the homunculus) "invade" or expand into the now-deprived hand/arm area
- This cortical remapping (neuroplasticity) means that stimulating the face now activates neurons in the cortex that the brain "thinks" are still connected to the absent hand
- The patient therefore feels sensations in the phantom limb when their face is touched
Classic example (Ramachandran's finding):
In patients with arm amputation, stroking different parts of the face can produce the distinct sensation of being touched in the area of the missing hand/fingers.
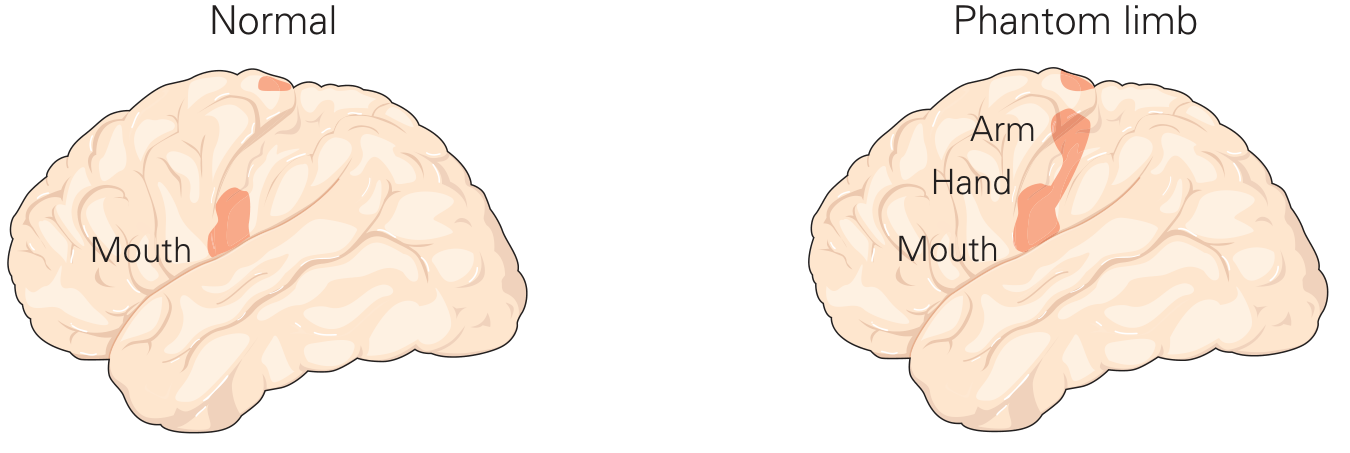
Kandel's Principles of Neural Science (6th Ed) - Cortical reorganization in phantom limb pain: the mouth representation expands into the deprived hand/arm cortical area.
Thalamic reorganization also occurs:
- In leg amputees, single neuron recordings show that thalamic neurons in the ventral posterior nucleus (which previously received leg/foot input) now respond to stimulation of the stump (thigh)
- Thalamic reorganization is closely related to the perception of phantom limbs
D. Neuromatrix Theory (Melzack, 1990)
- The brain has a genetically programmed "neuromatrix" - a network of neurons that generates a characteristic pattern of impulses representing the body (neurosignature)
- This neuromatrix includes the thalamus, somatosensory cortex, limbic system, and prefrontal areas
- Even without peripheral input, the neuromatrix continues to generate the body's "neurosignature," producing the sense that the limb is still present
- Explains why phantom limbs occur even in congenital amputees (born without a limb) - the neuromatrix exists independently of peripheral sensory experience
E. Gate Control Theory (Melzack & Wall)
- Amputation reduces large-fiber (A-beta) input to the spinal cord
- The "gate" in the dorsal horn is no longer held closed
- Small C-fiber nociceptive signals pass more freely, generating pain perceptions
5. Role of Cortical Plasticity - Summary Table
| Level | Change | Result |
|---|---|---|
| Peripheral | Neuroma formation | Ectopic firing → phantom sensations |
| Spinal cord | Dorsal horn hyperexcitability, loss of inhibition | Amplified/distorted pain signals |
| Thalamus | Remapping of VPN neurons to adjacent body area | Misattribution of stimuli to absent limb |
| Somatosensory cortex | Adjacent representation expands into deprived area | Touch on face → sensation in phantom hand |
| Neuromatrix | Persistent body schema without peripheral input | Limb "felt" even in congenitally absent limbs |
6. Important Clinical Points for Viva/Exam
- Phantom limb is a NORMAL consequence of amputation - it is NOT a psychiatric condition
- Pain more common if patient had pre-existing pain in the limb before amputation
- Telescoping = gradual retraction and shrinking of the phantom, associated with more PLP
- Mirror box therapy (Ramachandran): Visual feedback using a mirror creates the illusion that the amputated limb is present and moving - this "tricks" the brain's cortical reorganization and can reduce phantom pain
- Spinal cord stimulation - passes electric current via electrode next to spinal cord; interferes with ascending pain impulses; amputees feel tingling instead of pain
- Epidural anesthesia during amputation surgery reduces incidence of phantom pain by preventing acute pain-mediated central sensitization
- TENS, opioids, calcitonin, ketamine, and tricyclic antidepressants have been used in treatment
7. Key Points to Remember (Quick Revision)
- Phantom limb = sensation from absent limb; affects 50-80% of amputees
- Mechanism = Cortical reorganization (neuroplasticity) is the core answer
- Adjacent cortical areas invade the deprived representation → touch on face = sensation in hand
- Also involves: neuroma ectopic firing, dorsal horn central sensitization, thalamic remapping, and neuromatrix persistence
- Telescoping = phantom shrinks toward stump
- Mirror therapy exploits visual cortical plasticity to relieve PLP
- Phantom limb is NOT limited to amputation - occurs after any body part removal
Sources:
- Ganong's Review of Medical Physiology (26th Ed), Phantom Limb Pain section
- Bradley & Daroff's Neurology in Clinical Practice, Phantom-Limb Pain and Stump Pain
- Kandel's Principles of Neural Science (6th Ed), Ch. 20 - Cortical Reorganization in Phantom Limb Pain
- Harrison's Principles of Internal Medicine (22nd Ed)
For examBasis of phantom limb Notes for mbbs 1st year physiology
For examBasis of phantom limb Notes for mbbs 1st year physiology
Basis of phantom limb for short notes for exam pov
Here are concise exam-focused short notes on Phantom Limb for MBBS 1st Year Physiology:
PHANTOM LIMB - Short Notes (Exam)
Definition
Perception of sensations (pain or non-painful) from a body part that has been amputated or is no longer present.
- Affects 50-80% of amputees
- First described by Ambroise Paré (1551)
Types
| Type | Features |
|---|---|
| Phantom sensation | Tingling, warmth, numbness, movement |
| Phantom limb pain | Burning, stabbing, cramping in absent limb |
| Stump pain | Pain at residual limb (neuroma) |
| Telescoping | Phantom appears to retract/shrink toward stump |
BASIS / MECHANISMS (Most Important for Exam)
1. Peripheral Mechanism - Neuroma Theory
- Cut nerve endings form neuromas at the stump
- Neuromas fire spontaneously (ectopically)
- Brain misinterprets signals as coming from the absent limb
2. Spinal Cord - Central Sensitization
- Loss of afferent input → dorsal horn neurons become hyperexcitable
- Loss of inhibitory interneurons (GABAergic)
- "Gate" opens → C-fiber pain signals pass freely (Gate Control Theory)
3. Cortical Reorganization (THE MOST IMPORTANT THEORY)
- The somatosensory cortex (Penfield's homunculus) is organized somatotopically
- After amputation, the cortical area for the amputated limb is deprived of input
- Adjacent cortical areas invade the deprived zone (neuroplasticity)
- In arm/hand amputees: the face/mouth representation expands into the hand area
- Touching the face → patient feels sensation in the phantom hand
- Similarly occurs at thalamic level (VPN neurons remap to stump)
4. Neuromatrix Theory (Melzack)
- Brain has a built-in "neuromatrix" - a neural network encoding the entire body image
- Even without peripheral input, it continues generating the body's "neurosignature"
- Explains phantom limb in congenital amputees (born without a limb)
Summary Flowchart
Amputation
↓
Peripheral: Neuroma → ectopic firing
↓
Spinal: Dorsal horn hyperexcitability (central sensitization)
↓
Thalamus: Remapping of VPN neurons
↓
Cortex: Somatosensory cortical reorganization
↓
Brain perceives sensation from ABSENT limb = PHANTOM LIMB
Important Viva Points
- Phantom limb is NOT psychiatric - sensations are real
- More likely if patient had pre-existing pain before amputation
- Phantom pain is worst in the distal part of the phantom
- Telescoping = phantom retracts toward stump; associated with more pain
- Mirror box therapy (Ramachandran) - visual illusion of limb movement reduces pain by reversing cortical reorganization
- Spinal cord stimulation - electrode near spinal cord blocks ascending pain → patient feels tingling instead of pain
- Epidural anesthesia during surgery reduces incidence of phantom pain
One-Line Exam Answer
Phantom limb is caused by cortical reorganization (neuroplasticity) in the somatosensory cortex, where adjacent areas invade the deprived representation of the amputated limb, combined with peripheral neuroma firing, spinal central sensitization, thalamic remapping, and persistence of the neuromatrix body image.
Sources: Ganong's Review of Medical Physiology (26th Ed) | Bradley & Daroff's Neurology | Kandel's Principles of Neural Science (6th Ed)
This is a shared conversation. Sign in to Orris to start your own chat.