SAH
Reading File
Finding Sources
Searching PubMed
"subarachnoid hemorrhage"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Here is a comprehensive overview of Subarachnoid Hemorrhage (SAH):
Subarachnoid Hemorrhage (SAH)
Definition
SAH is bleeding into the subarachnoid space (between the arachnoid and pia mater). It accounts for up to 10% of all strokes and is the most common cause of sudden stroke-related death. - Rosen's Emergency Medicine
Etiology
| Cause | Frequency |
|---|---|
| Ruptured saccular (berry) aneurysm | ~80% of non-traumatic SAH |
| AVM / cavernous angioma | Less common |
| Mycotic aneurysms, neoplasms, CNS vasculitis | Rare |
| Perimesencephalic hemorrhage (benign form) | Anterior to midbrain, no vascular abnormality |
Berry aneurysms typically form at or near junctions of major cerebral vessels, especially the circle of Willis. ~25% of patients with a berry aneurysm have more than one. Most aneurysms never rupture; risk of rupture increases with aneurysm size.
Risk factors: Hypertension, smoking, excessive alcohol, sympathomimetic drug use. Genetic associations include autosomal dominant polycystic kidney disease, Marfan syndrome, Ehlers-Danlos type IV, and coarctation of the aorta.
Clinical Features
- Thunderclap headache - "worst headache of my life," peaks in seconds to minutes
- Headaches peaking >60 minutes after onset are unlikely to be SAH
- Syncope (may be the initial manifestation)
- Nausea, vomiting
- Neck stiffness, photophobia
- Seizures
- Sentinel headache - up to 1/3 of patients recall a milder headache days to weeks prior
- Focal neuro deficits in up to 20% (e.g., CN III palsy from posterior communicating artery aneurysm causing pupillary dilation)
- ~50% have altered or fluctuating consciousness
ECG changes in up to 90%: ST-T wave changes, U waves, QT prolongation - can mimic acute cardiac ischemia.
Grading
Hunt and Hess Scale
| Grade | Condition |
|---|---|
| 0 | Unruptured aneurysm |
| 1 | Asymptomatic or minimal headache, slight nuchal rigidity |
| 2 | Moderate/severe headache, nuchal rigidity, no deficit except CN palsy |
| 3 | Drowsiness, confusion, mild focal deficit |
| 4 | Stupor, moderate-severe hemiparesis |
| 5 | Deep coma, decerebrate posturing, moribund |
Fisher Scale (CT-based) grades subarachnoid blood distribution and predicts vasospasm risk (Groups 1-4).
Diagnosis
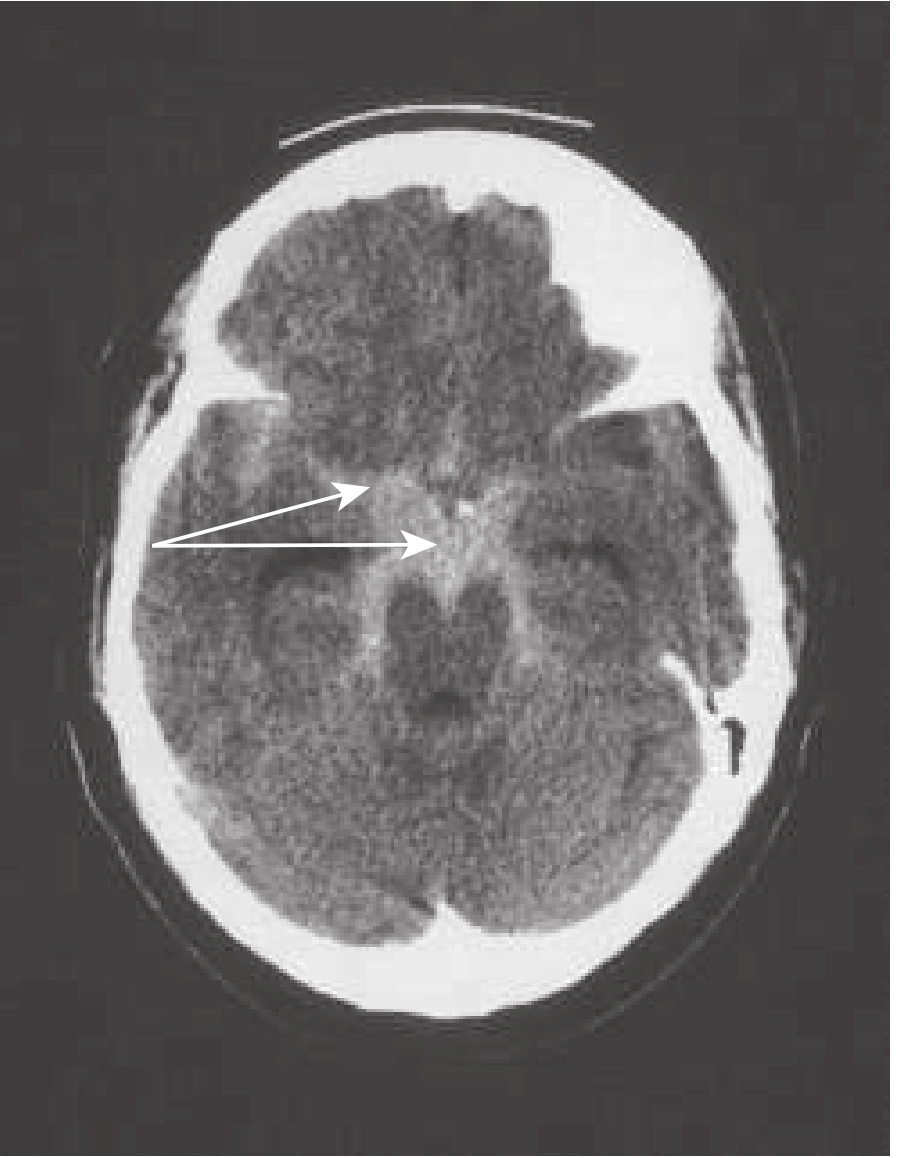
Step 1 - Non-contrast CT head (NCCT):
- Sensitivity ~100% within first 3 days; drops to ~50% by end of week 1
- Within 6 hours of onset, sensitivity approaches near-100% on modern multidetector CT
CT appearance of SAH:
Step 2 - Lumbar puncture (if CT is negative but clinical suspicion is high):
- Elevated RBC count
- Xanthochromia - detectable ~2 hours post-hemorrhage, persists for weeks
Step 3 - Vascular imaging:
- CTA or MRA to identify and characterize the aneurysm
- If CTA is negative with clear SAH: four-vessel conventional catheter angiography with 3D reconstruction is mandatory
- If 4-vessel angio and CTA both negative: six-vessel angiography (including external carotid) to rule out dural fistula
Ottawa SAH Rule (any one = workup indicated):
- Age ≥40
- Neck pain or stiffness
- Loss of consciousness
- Onset during exertion
- Thunderclap (instantly peaking) headache
- Limited neck flexion on exam
Differential Diagnosis
- Cervical artery dissection
- Cerebral venous thrombosis
- Reversible cerebral vasoconstriction syndrome
- Hemorrhagic or ischemic stroke
- Migraine, cluster headache
- CNS infection (meningitis) - distinguished by fever and slower onset
Management
Immediate priorities
| Issue | Management |
|---|---|
| Airway (Grade ≥3) | Early endotracheal intubation |
| Blood pressure | Target SBP <160 mmHg or MAP <130 mmHg; IV nicardipine or labetalol; maintain MAP >95 mmHg |
| Vasospasm prevention | Nimodipine 60 mg PO/NGT q4h (start immediately) |
| Pain | IV fentanyl (50 mcg aliquots) titrated; avoid oversedation |
| Nausea | Metoclopramide 10 mg IV or ondansetron 4 mg IV |
| Agitation | Fentanyl 50 mcg IV; add midazolam 1 mg IV if needed |
| Seizures | Levetiracetam or fosphenytoin for clinical seizures |
| Environment | Bed rest, quiet, dark room |
Corticosteroids are NOT beneficial.
Definitive treatment of the aneurysm
- Endovascular coil embolization is generally preferred over neurosurgical clipping
- Choice depends on aneurysm size, location, morphology, and local expertise
Disposition
All patients with ruptured aneurysms require ICU-level monitoring of hemodynamics and neurological status.
Prognosis
- ~10% die before reaching hospital; another ~10% die prior to hospital evaluation
- Overall mortality: 40-50%
- ~1/3 of survivors have functional and cognitive deficits
- WFNS Grade V (GCS 3) still carries ~22% good outcome rate in some studies
- Rebleeding with coma: 50% mortality
- Bilateral pupillary loss: ~95% mortality
Complications: vasospasm/delayed cerebral ischemia (DCI), rebleeding, hydrocephalus, brain edema, cardiac arrhythmias.
Sources: Rosen's Emergency Medicine 9e, p. 1467; Bradley and Daroff's Neurology in Clinical Practice; Plum and Posner's Diagnosis and Treatment of Stupor and Coma
Is patient of tubercular meningitis neck is extended
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Great content retrieved. Here is the complete, authoritative answer:
Neck Position in Tubercular Meningitis (TBM)
Short Answer
The neck in TBM is NOT simply "extended" - the correct term is nuchal rigidity (stiff neck), which means resistance to passive flexion. In severe cases, however, the patient may lie with the neck in extension as part of opisthotonus.
Understanding the Terminology
| Term | Meaning |
|---|---|
| Nuchal rigidity | Neck resists passive flexion - cannot touch chin to chest |
| Neck extension | Neck is held backward - NOT the primary description |
| Opisthotonus | Severe arching of the entire spine with neck hyperextension - seen in advanced/severe meningitis |
Nuchal Rigidity - The Correct Sign
Nuchal rigidity ("stiff neck") is the pathognomonic sign of meningeal irritation and is present when the neck resists passive flexion. The patient is unable to touch their chin to their chest.
It is present in 75% of TBM cases (Adams and Victor's Neurology).
This is accompanied by:
- Kernig's sign - Pain in the hamstrings when knees are straightened with hips flexed at 90°
- Brudzinski's sign - Passive flexion of the neck causes spontaneous flexion of the hips and knees
Why the Confusion About "Extension"?
When a patient has severe meningeal irritation and lies in bed, they often adopt a posture of neck extension and back arching - this is called opisthotonus. In this position:
- The neck is hyperextended (bent backward)
- The back is arched
- The knees may be drawn up
This occurs because meningeal inflammation causes reflex muscle spasm - the patient extends the neck to relieve stretch on the inflamed meninges. This is the extreme form of the same mechanism that causes nuchal rigidity.
Clinical Features of TBM Specifically
TBM differs from bacterial meningitis in key ways (Adams and Victor's Principles of Neurology):
- Subacute onset - symptoms evolve over 1-2 weeks (not hours like pyogenic meningitis)
- Early symptoms: low-grade fever, malaise, headache (>50%), lethargy, confusion, stiff neck (75%)
- In young children and infants: stiff neck may be absent - apathy, hyperirritability, vomiting, and seizures predominate
- Cranial nerve palsies (especially ocular palsies) in ~20%
- Signs of raised ICP: papilledema, CN VI palsy, deteriorating consciousness
Summary
| Question | Answer |
|---|---|
| Is the neck "stiff"? | Yes - nuchal rigidity in 75% of TBM |
| Does the neck resist flexion? | Yes - cannot flex chin to chest |
| Is the neck "extended"? | Only in opisthotonus (severe/advanced disease) |
| Is extension the primary clinical description? | No - stiffness (rigidity) is |
"Nuchal rigidity ('stiff neck') is the pathognomonic sign of meningeal irritation and is present when the neck resists passive flexion." - Harrison's Principles of Internal Medicine 22e
"Stiff neck (75% of cases), with Kernig and Brudzinski signs. Characteristically, these symptoms evolve much less rapidly in tuberculous than in bacterial meningitis." - Adams and Victor's Principles of Neurology, 12e
Bottom line: In TBM, the neck is stiff and resists flexion (nuchal rigidity). In advanced/severe cases, the neck may appear extended as part of opisthotonus. The correct clinical term is nuchal rigidity, not neck extension.
Difference between 25g spinal needle v/s 25g pencil tip needle
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Here is a complete, textbook-backed comparison:
25G Quincke (Standard Spinal) vs. 25G Pencil-Point Needle
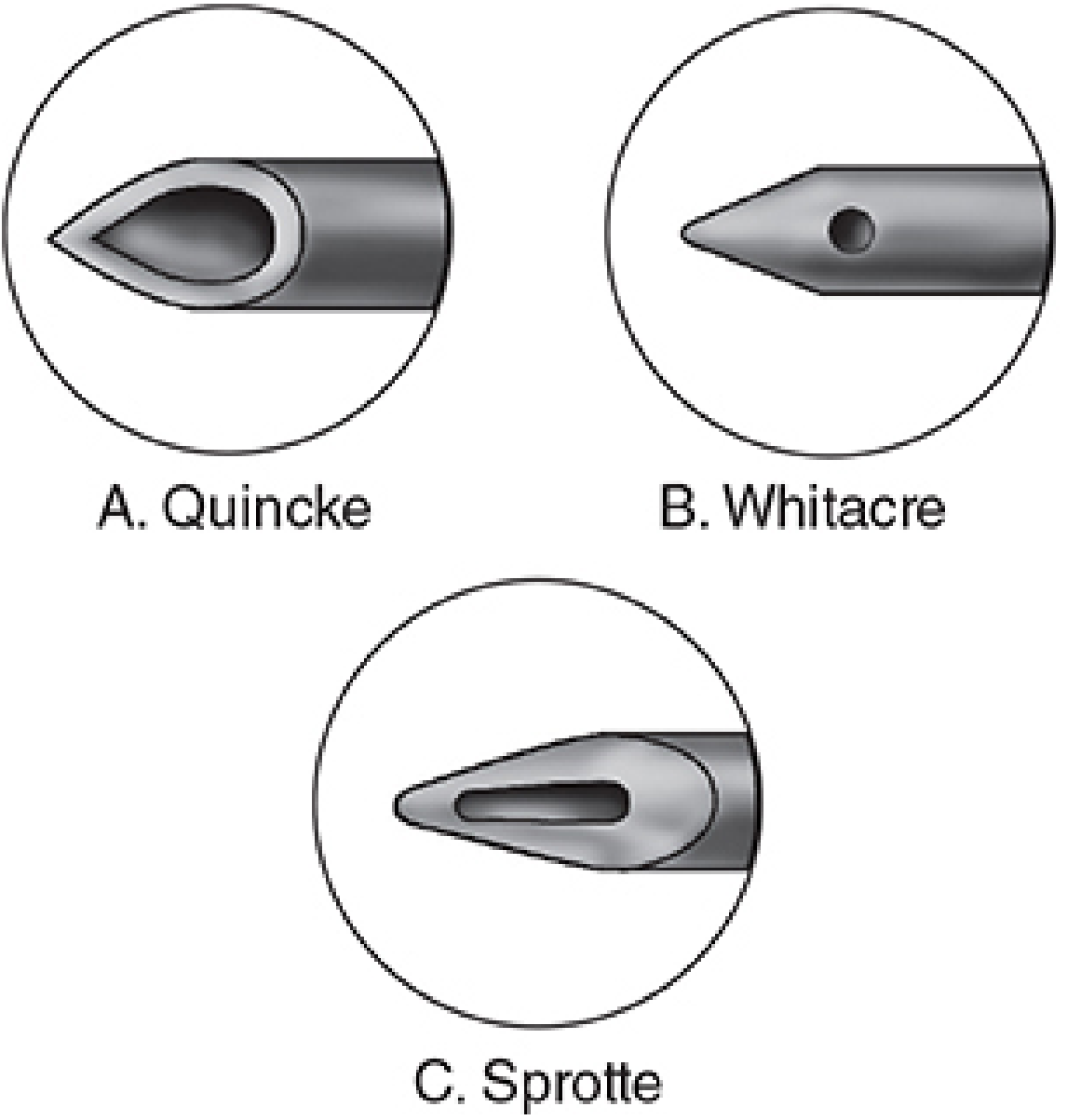
Fig: Spinal needle tip designs - A. Quincke, B. Whitacre (pencil-point), C. Sprotte (pencil-point with long opening). Morgan & Mikhail's Clinical Anesthesiology 7e
Side-by-Side Comparison
| Feature | 25G Quincke (Standard) | 25G Pencil-Point (Whitacre/Sprotte) |
|---|---|---|
| Tip design | Sharp, beveled cutting tip | Rounded, conical, atraumatic tip |
| Mechanism of dura entry | Cuts dural fibers | Separates / spreads dural fibers |
| Injection port | End (tip) injection | Side hole injection |
| Dural hole character | Clean-cut, smooth opening | Jagged/irregular opening |
| Post-dural puncture headache (PDPH) | Higher incidence | Lower incidence |
| Why lower PDPH? | Clean cut = persistent CSF leak | Jagged hole → inflammatory edema → better self-sealing |
| Tactile feel | Less tactile feedback | Better tactile sensation of tissue layers |
| Technical ease | Easier to place | Slightly more resistance; may need introducer |
| CSF flow | Good end-flow | Sprotte: vigorous side-flow; Whitacre: side-flow |
| Sprotte-specific pitfall | - | Long side-opening may straddle dura → failed block if only partial intrathecal |
Key Point: Why the Same Gauge Behaves Differently
Even at the same 25G diameter, the pencil-point needle causes significantly less PDPH:
"The incidence of headache is reduced with the use of pencil-point needles (Whitacre or Sprotte), compared with cutting bevel (Quincke) spinal needles."
- Barash's Clinical Anesthesia 9e
"The introduction of blunt tip (pencil-point) needles has markedly decreased the incidence of post-dural puncture headache."
- Morgan & Mikhail's Clinical Anesthesiology 7e
The mechanism is twofold:
- The rounded tip separates rather than cuts dural fibers
- The jagged hole left by a pencil-point needle triggers a stronger local inflammatory response → edema → better closure of the dural defect
PDPH Incidence by Needle Type & Gauge
| Needle | PDPH Rate |
|---|---|
| 16G Quincke | >70% |
| 22G Quincke | ~40% |
| 25G Quincke | ~3-5% |
| 25G Pencil-point | <1% |
| 29G (any) | <2% |
(Barash's Clinical Anesthesia 9e; Miller's Anesthesia 10e)
Types of Pencil-Point Needles
| Name | Side Opening | Special Feature |
|---|---|---|
| Whitacre | Small round side hole | Most common pencil-point |
| Sprotte | Long oval side opening | More vigorous CSF flow; risk of straddling dura |
| Gertie Marx | Side hole | Used in obstetric anesthesia |
| Pencan | Side hole | Similar to Whitacre |
Clinical Bottom Line
- Both are 25G - so the dural hole size is identical
- The key difference is tip geometry and dural entry mechanism
- Pencil-point is preferred for spinal anesthesia and obstetric patients (higher PDPH risk)
- Use a 25G pencil-point over 25G Quincke whenever PDPH prevention is the priority
- For diagnostic LP where CSF pressure measurement is needed, a 20-22G atraumatic needle is the best overall choice (25G can be too floppy and slow for adequate flow)
Sources: Morgan & Mikhail's Clinical Anesthesiology 7e; Miller's Anesthesia 10e; Barash's Clinical Anesthesia 9e; Roberts & Hedges' Clinical Procedures in Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.