Meritox lemi disease
Reading File
Finding Sources
Searching the Web
Meritox lemi disease medical condition
Finding Sources
Searching the Web
"Meritox" OR "lemi disease" medical syndrome diagnosis
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I have comprehensive information now. I can see you were asking about Lemierre's syndrome (phonetically "lemi-air"). Here is a complete overview:
Lemierre's Syndrome ("The Forgotten Disease")
Note: "Meritox lemi disease" appears to be a phonetic spelling of Lemierre's syndrome (named after French bacteriologist André Lemierre, who first described it in 1936). If you meant something else, please clarify.
What Is It?
Lemierre's syndrome is a septic thrombophlebitis of the internal jugular vein, typically following an oropharyngeal infection. It is caused in ~81% of cases by Fusobacterium necrophorum - an anaerobic, gram-negative rod found as normal flora of the oropharynx and GI tract. It was common in the pre-antibiotic era (mortality >50%), nearly disappeared after the 1940s, but cases are now rising again - possibly due to changing antibiotic prescribing patterns.
Incidence: ~3.6 cases/million/year. It primarily affects young, otherwise healthy adults (ages 16-30).
- Symptom to Diagnosis: An Evidence-Based Guide, 4th Ed.
- Harrison's Principles of Internal Medicine, 22nd Ed.
Pathogenesis
- Primary oropharyngeal infection (pharyngitis, peritonsillar abscess, dental infection)
- Spread to the parapharyngeal space
- Invasion of the internal jugular vein wall → septic thrombophlebitis
- Septic emboli travel hematogenously to distant organs (primarily lungs, but also liver, joints, CNS)
Clinical Features
Initial Phase
- Sore throat, high spiking fevers, rigors
- Unilateral neck pain, tenderness, and swelling (along the sternocleidomastoid)
- Oropharyngeal findings: ulceration, pseudomembrane, or erythema
Red-flag symptoms (not typical of simple pharyngitis)
- Dyspnea (24%)
- Pleuritic chest pain (31%) - suggests septic pulmonary emboli
- Abdominal pain (14%)
- Trismus (9%)
The symptoms of thrombophlebitis and septic emboli can mask the initial throat symptoms - this is why it's often missed.
Complications from Septic Emboli
| Site | Complication |
|---|---|
| Lungs | Septic emboli, lung abscesses, pleural effusion, empyema |
| Bone/joints | Septic arthritis, osteomyelitis |
| Liver | Liver abscess |
| CNS | Brain abscess, meningitis, cavernous sinus thrombosis |
Mortality with treatment: >15%. Harrison's Principles of Internal Medicine, 22nd Ed.
Diagnosis
High clinical suspicion is essential - signs and symptoms are nonspecific.
Classic diagnostic criteria (all 4 strongly support the diagnosis):
- Anaerobic primary infection of the oropharynx
- Positive blood culture (bacteremia) - note: F. necrophorum may take 5-8 days to isolate
- Metastatic infection at 1 or more distant site
- Thrombophlebitis of the internal jugular vein
Investigations:
- CT neck with IV contrast - best diagnostic modality; shows intraluminal thrombus, wall enhancement, soft tissue swelling along the IJV
- Doppler ultrasound - useful but limited for deep structures (below the mandible, above the clavicle)
- Chest X-ray / CT chest - to identify pulmonary septic emboli or abscesses
- Blood cultures (anaerobic bottles critical)
- CBC: leukocytosis with neutrophilia; elevated CRP
Below is a chest X-ray showing a lung abscess from septic emboli in Lemierre's syndrome:
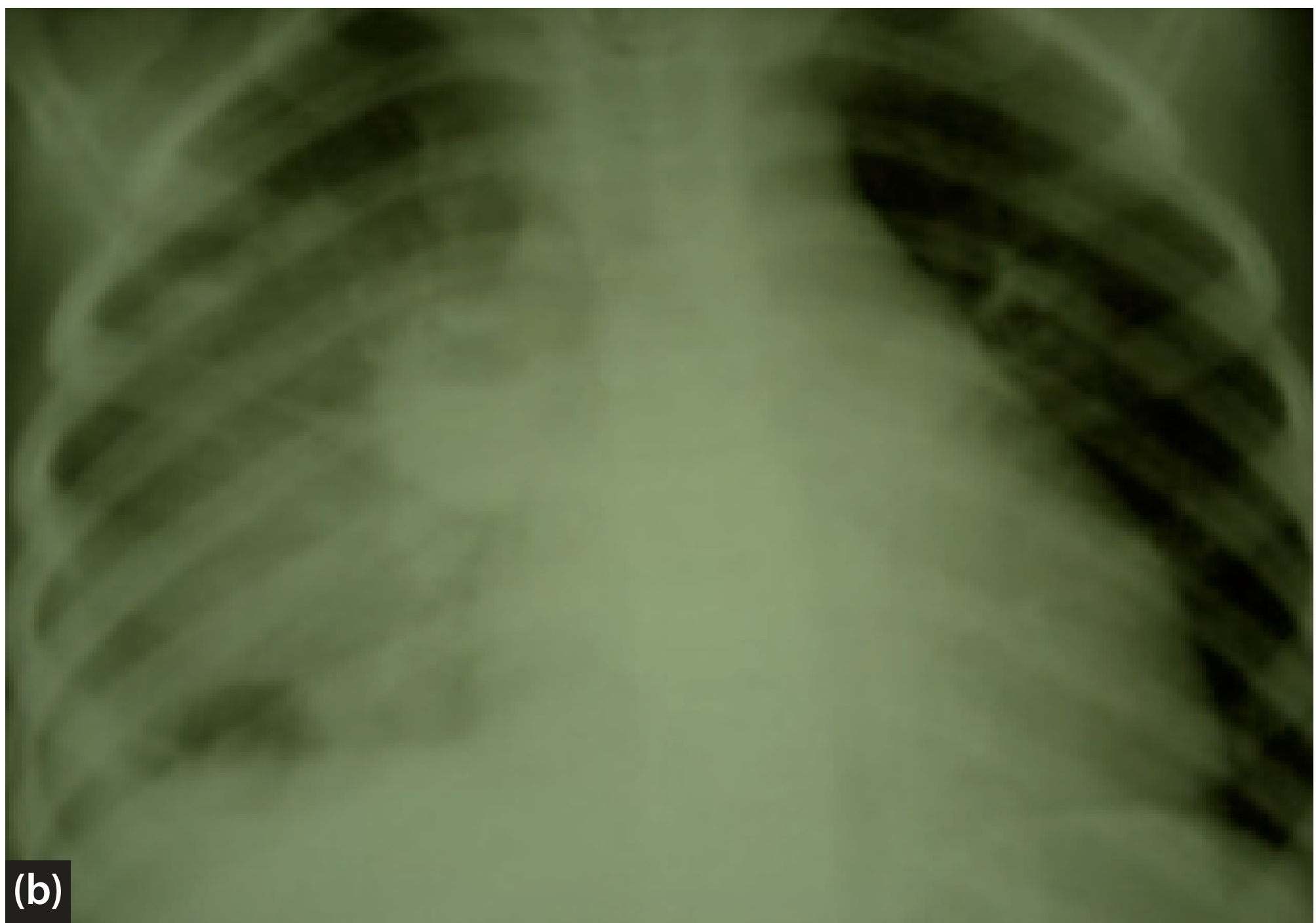
Scott-Brown's Otorhinolaryngology, Head & Neck Surgery, Vol. 2
Treatment
Antibiotics (mainstay)
- F. necrophorum is susceptible to:
- Beta-lactamase-resistant beta-lactams (e.g., piperacillin-tazobactam, ampicillin-sulbactam)
- Clindamycin
- Metronidazole
- Chloramphenicol
- Variable response to 2nd and 3rd-generation cephalosporins
- Duration: typically several weeks of IV antibiotics
Surgical
- Required if abscesses develop (neck, lung, liver) or antibiotic treatment fails
- Ligation/excision of the suppurated IJV is rarely needed but used for recurrent septic emboli
Anticoagulation
-
Controversial - no controlled trials due to rarity. Some centers use it for persistent emboli, but routine use is not established.
-
Symptom to Diagnosis: An Evidence-Based Guide, 4th Ed.
-
Cummings Otolaryngology Head and Neck Surgery
Key Points to Remember
- Sometimes called the "forgotten disease" - many clinicians miss it because it's rare and mimics simple pharyngitis early on
- Think of Lemierre's in any young patient with: sore throat + unilateral neck swelling + high fevers + pulmonary infiltrates/emboli
- F. necrophorum is also an endemic cause of pharyngitis in adolescents - the exact progression to Lemierre's syndrome is not fully understood
- Blood cultures should include anaerobic bottles
- Fusobacterium bloodstream infections in older adults warrant workup for occult GI or GU malignancy (Harrison's 22e)
This is a shared conversation. Sign in to Orris to start your own chat.