~/piles-treatment/build_doc.js
const {
Document, Packer, Paragraph, TextRun, Table, TableRow, TableCell,
HeadingLevel, AlignmentType, BorderStyle, WidthType, ShadingType,
VerticalAlign, PageBreak, UnderlineType, convertInchesToTwip
} = require('docx');
const fs = require('fs');
// Helper: Heading 1
function h1(text) {
return new Paragraph({
text,
heading: HeadingLevel.HEADING_1,
spacing: { before: 300, after: 120 },
});
}
// Helper: Heading 2
function h2(text) {
return new Paragraph({
text,
heading: HeadingLevel.HEADING_2,
spacing: { before: 240, after: 80 },
});
}
// Helper: Heading 3
function h3(text) {
return new Paragraph({
text,
heading: HeadingLevel.HEADING_3,
spacing: { before: 180, after: 60 },
});
}
// Helper: body paragraph
function p(text, bold = false) {
return new Paragraph({
children: [new TextRun({ text, bold, size: 22 })],
spacing: { after: 80 },
});
}
// Helper: bullet
function bullet(text) {
return new Paragraph({
text,
bullet: { level: 0 },
spacing: { after: 60 },
run: { size: 22 },
});
}
// Helper: sub-bullet
function bullet2(text) {
return new Paragraph({
text,
bullet: { level: 1 },
spacing: { after: 50 },
run: { size: 21 },
});
}
// Helper: warning box text
function warning(text) {
return new Paragraph({
children: [new TextRun({ text: '⚠ ' + text, bold: true, color: 'C0392B', size: 22 })],
spacing: { before: 80, after: 80 },
border: {
left: { style: BorderStyle.THICK, size: 9, color: 'C0392B' },
},
indent: { left: 200 },
});
}
// Helper: prescription box title
function rxTitle(text) {
return new Paragraph({
children: [new TextRun({ text, bold: true, size: 24, color: '1A5276' })],
spacing: { before: 120, after: 60 },
border: {
bottom: { style: BorderStyle.SINGLE, size: 6, color: '1A5276' },
},
});
}
// Helper: simple table
function makeTable(headers, rows, colWidths) {
const headerCells = headers.map((h, i) =>
new TableCell({
children: [new Paragraph({
children: [new TextRun({ text: h, bold: true, size: 20, color: 'FFFFFF' })],
alignment: AlignmentType.CENTER,
})],
shading: { fill: '1A5276', type: ShadingType.CLEAR, color: '1A5276' },
width: { size: colWidths ? colWidths[i] : Math.floor(9000 / headers.length), type: WidthType.DXA },
verticalAlign: VerticalAlign.CENTER,
})
);
const dataRows = rows.map((row, ri) =>
new TableRow({
children: row.map((cell, ci) =>
new TableCell({
children: [new Paragraph({
children: [new TextRun({ text: cell, size: 20 })],
alignment: AlignmentType.LEFT,
})],
shading: ri % 2 === 0
? { fill: 'EBF5FB', type: ShadingType.CLEAR, color: 'EBF5FB' }
: { fill: 'FFFFFF', type: ShadingType.CLEAR, color: 'FFFFFF' },
width: { size: colWidths ? colWidths[ci] : Math.floor(9000 / row.length), type: WidthType.DXA },
margins: { top: 60, bottom: 60, left: 100, right: 100 },
})
),
})
);
return new Table({
rows: [new TableRow({ children: headerCells }), ...dataRows],
width: { size: 9000, type: WidthType.DXA },
margins: { top: 60, bottom: 60, left: 100, right: 100 },
});
}
// ─────────────────────────────────────────────
// DOCUMENT CONTENT
// ─────────────────────────────────────────────
const doc = new Document({
title: 'Piles (Hemorrhoids) Detailed Prescription Treatment Guide',
creator: 'Orris Medical AI',
styles: {
default: {
heading1: {
run: { bold: true, size: 32, color: '1A5276', font: 'Calibri' },
paragraph: { spacing: { before: 360, after: 120 } },
},
heading2: {
run: { bold: true, size: 28, color: '154360', font: 'Calibri' },
paragraph: { spacing: { before: 240, after: 80 } },
},
heading3: {
run: { bold: true, size: 24, color: '1F618D', font: 'Calibri' },
paragraph: { spacing: { before: 180, after: 60 } },
},
document: {
run: { size: 22, font: 'Calibri' },
paragraph: { spacing: { after: 80 } },
},
},
},
sections: [
{
properties: {
page: {
margin: {
top: convertInchesToTwip(1),
right: convertInchesToTwip(1),
bottom: convertInchesToTwip(1),
left: convertInchesToTwip(1),
},
},
},
children: [
// ── TITLE PAGE ──────────────────────────────────
new Paragraph({
children: [
new TextRun({ text: 'PILES (HEMORRHOIDS)', bold: true, size: 52, color: '1A5276', font: 'Calibri' }),
],
alignment: AlignmentType.CENTER,
spacing: { before: 400, after: 80 },
}),
new Paragraph({
children: [
new TextRun({ text: 'Complete Prescription Treatment Guide', bold: true, size: 36, color: '2E86C1', font: 'Calibri' }),
],
alignment: AlignmentType.CENTER,
spacing: { after: 80 },
}),
new Paragraph({
children: [
new TextRun({ text: 'All Case Types | Drug · Dose · Duration | Evidence-Based', size: 26, color: '5D6D7E', font: 'Calibri' }),
],
alignment: AlignmentType.CENTER,
spacing: { after: 80 },
}),
new Paragraph({
children: [new TextRun({ text: 'Based on ASCRS 2024 | Sleisenger & Fordtran | Sabiston | Pfenninger & Fowler', size: 22, color: '7F8C8D', font: 'Calibri' })],
alignment: AlignmentType.CENTER,
spacing: { after: 600 },
}),
new Paragraph({
children: [new PageBreak()],
}),
// ══════════════════════════════════════════════
// SECTION 1: ANATOMY & CLASSIFICATION
// ══════════════════════════════════════════════
h1('SECTION 1: ANATOMY & CLASSIFICATION'),
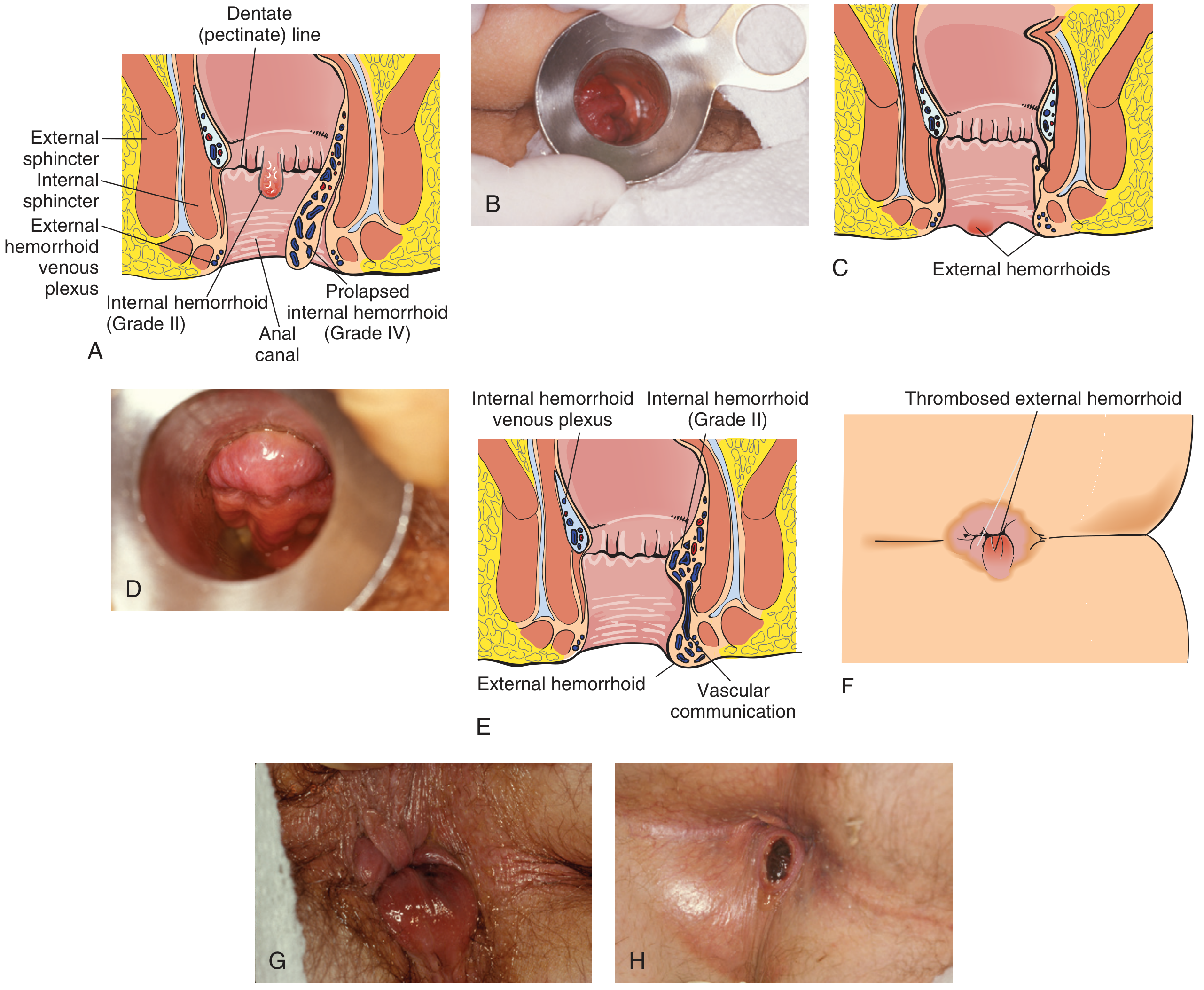
p('Hemorrhoids (piles) are pathologically enlarged, symptomatic vascular cushions in the anal canal. They are present normally in all individuals and become pathological only when symptomatic. The three primary hemorrhoidal columns are located at the right anterior, right posterior, and left lateral positions.'),
h2('1.1 Anatomical Location Reference'),
p('The dentate (pectinate) line is the crucial anatomical landmark that separates internal from external hemorrhoids.'),
bullet('ABOVE dentate line → Internal hemorrhoids (covered by mucosa, no somatic pain)'),
bullet('BELOW dentate line → External hemorrhoids (covered by anoderm, somatic innervation = PAINFUL)'),
bullet('BOTH components → Mixed hemorrhoids'),
h2('1.2 Classification of Internal Hemorrhoids (Goligher Grading)'),
makeTable(
['Grade', 'Anatomy', 'Symptoms', 'Prolapse Behavior'],
[
['Grade I', 'Enlarge into anal canal; do not prolapse', 'Painless bright-red rectal bleeding', 'No prolapse'],
['Grade II', 'Prolapse during straining/defecation', 'Bleeding, pressure, pruritus', 'Spontaneously self-reducing'],
['Grade III', 'Prolapse with straining', 'Bleeding, pressure, mucoid discharge', 'Requires manual digital reduction'],
['Grade IV', 'Chronically prolapsed / incarcerated', 'Pain, bleeding, mucoid discharge', 'Cannot be reduced; risk of strangulation'],
],
[1200, 2400, 2800, 2600]
),
new Paragraph({ spacing: { after: 120 } }),
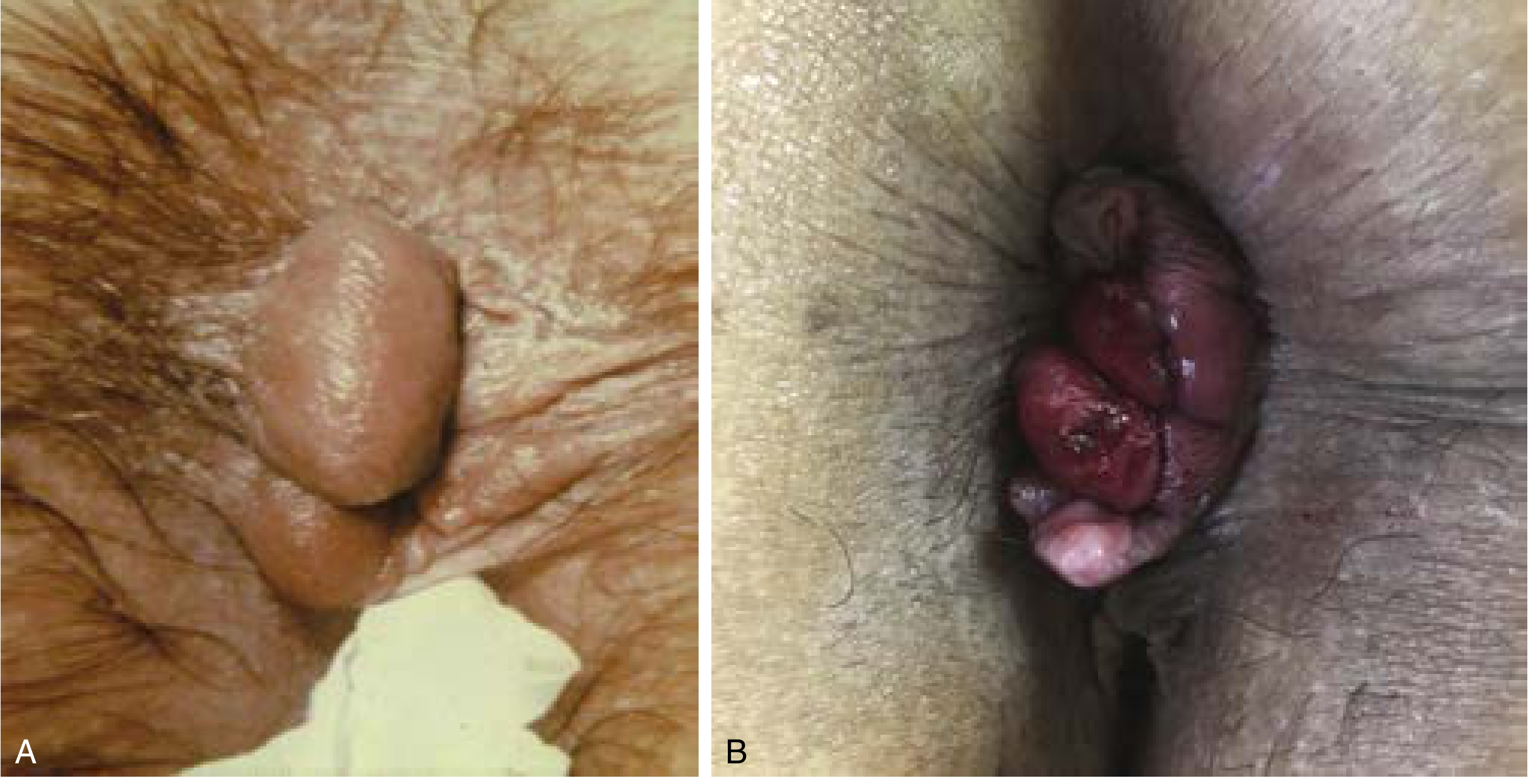
h2('1.3 External Hemorrhoids'),
makeTable(
['Type', 'Presentation', 'Key Feature'],
[
['Non-thrombosed', 'Soft skin folds, pruritus, hygiene problems', 'Painless unless thrombosed'],
['Thrombosed (TEH)', 'Sudden severe anal pain, firm blue-purple perianal lump', 'TIME-SENSITIVE: treat within 72 hours'],
],
[2500, 3500, 3000]
),
new Paragraph({ children: [new PageBreak()] }),
// ══════════════════════════════════════════════
// SECTION 2: UNIVERSAL BASELINE PRESCRIPTIONS
// ══════════════════════════════════════════════
h1('SECTION 2: UNIVERSAL BASELINE PRESCRIPTIONS (ALL GRADES)'),
p('The following medications and measures form the foundation of treatment across all hemorrhoid grades. They must be prescribed alongside any procedure-specific therapy.'),
h2('Rx 1 — Dietary Fiber Supplementation (Bulk-Forming Agents)'),
p('Grade A evidence — reduces bleeding, straining, and recurrence.'),
makeTable(
['Drug', 'Dose', 'Route', 'Frequency', 'Duration'],
[
['Psyllium husk (Ispaghula)', '5–10 g in 240 mL water', 'Oral', '1–3 times daily', 'Long-term (ongoing)'],
['Methylcellulose', '1.5–6 g/day divided', 'Oral', '2–3 times daily', 'Long-term'],
['Calcium polycarbophil', '1 g per dose', 'Oral', '1–4 times daily', 'Long-term'],
],
[2200, 2200, 1200, 1600, 1800]
),
p('NOTE: Always take with at least one full glass (240 mL) of water. Do not take at bedtime.', false),
new Paragraph({ spacing: { after: 100 } }),
h2('Rx 2 — Stool Softeners / Osmotic Laxatives'),
makeTable(
['Drug', 'Dose', 'Frequency', 'Duration', 'Indication'],
[
['Docusate sodium (DSS)', '100 mg', 'Twice daily', '2–4 weeks', 'Standard first-line softener'],
['Lactulose', '15–30 mL', 'Once or twice daily', 'Until regular bowel habit', 'Constipation predominant'],
['Polyethylene glycol 3350 (PEG)', '17 g in 240 mL water', 'Once daily', 'Short–medium term', 'Hard stool; fiber insufficient'],
],
[2000, 1400, 1600, 1800, 2200]
),
new Paragraph({ spacing: { after: 100 } }),
h2('Rx 3 — Topical Anesthetics (Symptomatic Relief)'),
warning('Topical agents provide SHORT-TERM symptom relief only. They have NO proven disease-modifying effect. Max 7–14 days of continuous use.'),
makeTable(
['Drug', 'Formulation', 'Application', 'Frequency', 'Max Duration'],
[
['Lidocaine 5%', 'Ointment/gel', 'Apply to anal area', '3–4 times daily', '14 days'],
['Pramoxine (Pramocaine)', 'Cream/ointment', 'Apply to anal area', '3–4 times daily', '14 days'],
['Dibucaine (Cinchocaine) 0.5–1%', 'Ointment', 'Apply AM, PM, after each stool', '3 times daily', '14 days'],
['Benzocaine', 'Cream/gel', 'Apply as needed', 'Up to 4 times daily', '7 days'],
],
[2200, 1600, 1800, 1800, 1600]
),
new Paragraph({ spacing: { after: 100 } }),
h2('Rx 4 — Topical Steroids (Short-Term Use Only)'),
warning('Hydrocortisone and betamethasone are NO LONGER recommended for long-term use in hemorrhoids (current SFDA/CHI guideline). Predisposition to candidiasis and skin atrophy.'),
makeTable(
['Drug', 'Formulation', 'Application', 'Frequency', 'MAX Duration'],
[
['Hydrocortisone 1–2.5%', 'Cream/ointment/suppository', 'Apply thin layer to anal area', 'Twice daily', '7 days ONLY'],
],
[2500, 2200, 2500, 1400, 1400]
),
new Paragraph({ spacing: { after: 100 } }),
h2('Rx 5 — Phlebotonics / Venoactive Drugs (Venotropics)'),
p('Phlebotonics improve venous tone, reduce capillary permeability, and improve lymphatic drainage. Cochrane review confirms efficacy for bleeding (OR 0.12), pruritus (OR 0.23), and discharge. Recommended SHORT-TERM in acute disease only (Grade A evidence for efficacy, Grade D against long-term use).'),
makeTable(
['Drug', 'Standard Dose', 'Frequency', 'Duration', 'Notes'],
[
['MPFF – Diosmin 90% + Hesperidin 10% (Daflon 500 mg)', '500 mg', 'Twice daily OR 1000 mg once daily', 'Acute: 2–3 months max; short courses', 'Best-evidence phlebotonic; Grade A'],
['Diosmin (plain)', '600 mg', 'Twice daily', '2–3 months; short acute courses', 'Available as supplement in USA'],
['Troxerutin / Hydroxyethylrutoside', '300 mg', 'Three times daily', 'Short-term acute treatment', ''],
['Calcium dobesilate 500 mg', '500 mg', 'Three times daily', 'Short-term ONLY', 'CAUTION: risk of agranulocytosis – monitor CBC'],
],
[2400, 1400, 1800, 1800, 1600]
),
new Paragraph({ spacing: { after: 100 } }),
h2('Non-Drug Measures (Mandatory for ALL Grades)'),
bullet('Warm sitz baths: 10–15 minutes, 2–3 times daily and after each bowel movement'),
bullet('Fluid intake: minimum 6–8 glasses (non-alcoholic, non-caffeinated) per day'),
bullet('High-fiber diet: 25–35 g dietary fiber per day'),
bullet('Reduce toilet sitting time to < 3 minutes; remove phones and reading material'),
bullet('Avoid straining and prolonged bearing down'),
bullet('Proper anal hygiene; avoid aggressive wiping'),
bullet('Witch hazel-impregnated pads after each stool for external symptoms'),
new Paragraph({ children: [new PageBreak()] }),
// ══════════════════════════════════════════════
// SECTION 3: GRADE-BY-GRADE PRESCRIPTION PLANS
// ══════════════════════════════════════════════
h1('SECTION 3: GRADE-BY-GRADE PRESCRIPTION TREATMENT PLANS'),
// ─── GRADE I ───────────────────────────────────
h2('CASE TYPE 1: Internal Hemorrhoids — Grade I'),
p('Presentation: Painless bright-red rectal bleeding; hemorrhoid visible on anoscopy but does NOT prolapse; no pain.', true),
h3('Step 1: First-Line Medical Treatment'),
p('Start ALL of the following simultaneously:'),
bullet('Psyllium husk 5–10 g in water, 1–2 times daily (ongoing)'),
bullet('Docusate sodium 100 mg twice daily × 4 weeks'),
bullet('Sitz baths 2–3 times daily'),
bullet('MPFF (Daflon) 500 mg twice daily × 4–8 weeks if bleeding persists'),
h3('Step 2: Topical Symptom Relief (if pruritus/discomfort)'),
bullet('Pramoxine 1% cream applied 3–4 times daily × 14 days maximum'),
bullet('Witch hazel pads after each stool'),
h3('Step 3: Office Procedure if Medical Therapy Fails (> 4–6 weeks)'),
makeTable(
['Procedure', 'Technique', 'Sessions', 'Recovery'],
[
['Infrared Photocoagulation (IRC)', 'Infrared probe 1.5 sec at 2–3 sites proximal to plexus', 'Multiple hemorrhoids per session', 'Minimal; preferred for Grade I'],
['Injection Sclerotherapy', '5% phenol in oil 3–5 mL injected into submucosa at anorectal ring', 'All 3 columns in 1 session; repeat at 4–6 wk', 'Dull ache 1–2 days; safe in anticoagulated pts'],
],
[2200, 3000, 2000, 1800]
),
new Paragraph({ spacing: { after: 120 } }),
// ─── GRADE II ──────────────────────────────────
h2('CASE TYPE 2: Internal Hemorrhoids — Grade II'),
p('Presentation: Prolapse during straining with SPONTANEOUS reduction; bleeding; pressure; pruritus.', true),
h3('Step 1: Baseline Medical Treatment (same as Grade I)'),
bullet('Psyllium husk + docusate sodium + sitz baths (as above)'),
bullet('MPFF (Daflon) 500 mg twice daily × 6–8 weeks — Grade II indication'),
bullet('Topical lidocaine 5% or pramoxine 1% PRN for discomfort × 14 days max'),
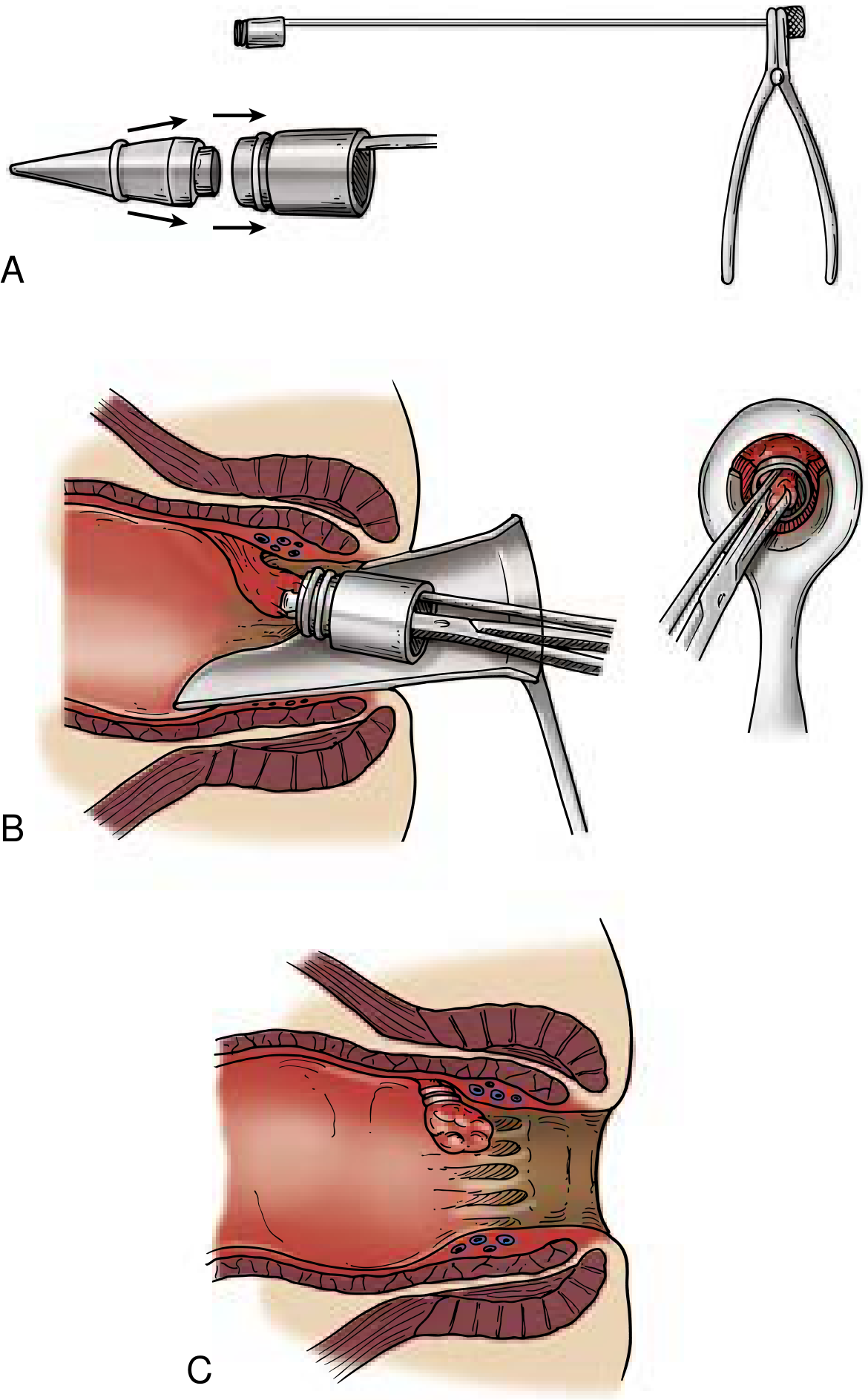
h3('Step 2: Preferred Office Procedure — Rubber Band Ligation (RBL)'),
p('RBL is the most effective office-based therapy for Grade II hemorrhoids (ASCRS 2024, Grade A).'),
makeTable(
['Parameter', 'Detail'],
[
['Band position', '2 cm ABOVE dentate line (no somatic sensation at this level)'],
['Hemorrhoids per session', '1 column at first session; up to 2 thereafter'],
['Session interval', '3–4 weeks apart'],
['Expected sessions', '2–4 sessions for complete resolution'],
['Success rate', '>90%'],
['Tissue slough timing', 'Band sloughs ~7 days; minor bleeding expected'],
['Contraindications', 'Anticoagulants, portal hypertension, immunocompromise'],
],
[3000, 6000]
),
h3('Step 3: Post-RBL Prescription'),
makeTable(
['Drug', 'Dose', 'Frequency', 'Duration', 'Purpose'],
[
['Paracetamol (acetaminophen)', '500–1000 mg', 'Every 6–8 hours PRN', 'First 48 hours', 'Dull ache relief post-procedure'],
['Ibuprofen', '400 mg with food', 'Every 8 hours PRN', '48–72 hours', 'Analgesic/anti-inflammatory'],
['Docusate sodium', '100 mg', 'Twice daily', '2 weeks post-procedure', 'Prevent hard stool on banded tissue'],
['Psyllium husk', '5–10 g/day', 'Daily', 'Ongoing', 'Stool consistency maintenance'],
],
[2200, 1400, 1800, 1800, 1800]
),
h3('Alternative: Sclerotherapy (for anticoagulated patients)'),
bullet('5% phenol in oil: 2–3 mL per column (ethanolamine: 1 mL per column)'),
bullet('All 3 columns treated in ONE session under anoscopy'),
bullet('Repeat after 4–6 weeks if needed'),
new Paragraph({ spacing: { after: 120 } }),
// ─── GRADE III ─────────────────────────────────
h2('CASE TYPE 3: Internal Hemorrhoids — Grade III'),
p('Presentation: Prolapse requires MANUAL digital reduction; bleeding; pressure; mucoid discharge. Most common grade requiring procedural/surgical intervention.', true),
h3('Step 1: Baseline Medical Treatment (Bridge Therapy)'),
bullet('Psyllium husk 5–10 g/day (ongoing)'),
bullet('Docusate sodium 100 mg twice daily'),
bullet('MPFF (Daflon) 500 mg twice daily × 2–3 months — significant benefit for Grade III'),
bullet('Sitz baths 2–3 times daily'),
bullet('Topical anesthetic PRN × 14 days max'),
h3('Step 2: Office Procedure — RBL (First-Line for Grade III)'),
p('Schedule 3–4 sessions at 3–4 week intervals. If Grade III fails after 3 courses of RBL, escalate to surgery.'),
h3('Step 3: Surgical Hemorrhoidectomy (for failures or large external component)'),
p('Conventional excisional hemorrhoidectomy (Milligan-Morgan open / Ferguson closed technique) is the gold standard for Grade III failing office procedures.'),
makeTable(
['Aspect', 'Details'],
[
['Anesthesia', 'Local with MAC, spinal, or general anesthesia; day surgery'],
['Position', 'Lithotomy or prone jack-knife'],
['Wound', 'Open (Milligan-Morgan) or closed (Ferguson) — equal efficacy'],
['Energy device', 'Scalpel, cautery, harmonic scalpel, LigaSure'],
['Prophylactic antibiotics', 'NOT routinely indicated'],
['Recurrence at 17 years', '26%; 11% require additional procedure'],
],
[3000, 6000]
),
h3('Post-Operative Prescription (Hemorrhoidectomy)'),
makeTable(
['Drug', 'Dose', 'Frequency', 'Duration', 'Evidence / Notes'],
[
['Paracetamol + Codeine', '500 mg / 30 mg', 'Every 4–6 hours PRN', '5–7 days', 'First-line post-op opioid analgesia'],
['Ibuprofen or Diclofenac', '400–600 mg / 50 mg with food', 'Every 8 hours', '5–7 days', 'NSAID adjunct; avoid if bleeding risk'],
['Metronidazole 400 mg', '400 mg', 'Three times daily', '7–10 days', 'REDUCES post-op pain (RCT evidence) + anaerobic cover'],
['Lactulose or Movicol', '15–20 mL / 1–2 sachets', 'Twice daily', '4–6 weeks post-op', 'MANDATORY — prevents hard stool on wound'],
['GTN 0.2–0.4% ointment', 'Thin perianal layer', '2–3 times daily', '4–8 weeks', 'Reduces post-op pain; promotes wound healing'],
['Topical lidocaine 2% gel', 'Apply to wound', '3–4 times daily', '1–2 weeks', 'Local wound analgesia'],
['Sitz baths', 'Warm water 10–15 min', '3 times daily', '4–6 weeks', 'Pain relief + wound hygiene'],
],
[2200, 1600, 1600, 1600, 2000]
),
new Paragraph({ spacing: { after: 120 } }),
// ─── GRADE IV ──────────────────────────────────
h2('CASE TYPE 4: Internal Hemorrhoids — Grade IV (Incarcerated / Prolapsed)'),
p('Presentation: Permanently prolapsed, CANNOT be reduced manually; pain; bleeding; risk of strangulation and gangrene. REQUIRES URGENT SURGICAL CONSULTATION.', true),
warning('Grade IV hemorrhoids with incarceration or gangrenous tissue require EMERGENCY surgical consultation and potentially urgent hemorrhoidectomy.'),
h3('Acute Management — Hospital Setting'),
makeTable(
['Drug', 'Dose', 'Route', 'Frequency', 'Duration', 'Purpose'],
[
['Morphine sulfate', '2–4 mg', 'IV', 'Every 2–4 hours PRN', 'Acute admission', 'Severe pain control'],
['Ceftriaxone 1–2 g', '1–2 g', 'IV', 'Once daily', '5–7 days', 'Perianal sepsis cover if strangulated'],
['Metronidazole 500 mg', '500 mg', 'IV', 'Every 8 hours', '5–7 days', 'Anaerobic bacterial cover'],
['MPFF (Daflon) — Acute Protocol', '1500 mg Day 1–4; then 1000 mg Day 5–7', 'Oral', 'Once daily (total 7-day course)', '7 days only', 'Reduces acute hemorrhoidal crisis symptoms'],
],
[1800, 1200, 900, 1800, 1300, 2000]
),
h3('Definitive Treatment'),
bullet('Elective surgical hemorrhoidectomy if no gangrene'),
bullet('Emergency hemorrhoidectomy for strangulation — same day'),
bullet('Gangrene with sepsis: immediate OR debridement + IV broad-spectrum antibiotics (Piperacillin-Tazobactam 4.5 g IV TDS)'),
p('Post-operative prescription: Same as Grade III hemorrhoidectomy protocol above.'),
new Paragraph({ children: [new PageBreak()] }),
// ══════════════════════════════════════════════
// SECTION 4: EXTERNAL & THROMBOSED HEMORRHOIDS
// ══════════════════════════════════════════════
h1('SECTION 4: EXTERNAL & THROMBOSED HEMORRHOIDS'),
h2('CASE TYPE 5: External Hemorrhoids — Non-Thrombosed'),
p('Presentation: Painless perianal skin folds (tags), pruritus, hygiene difficulty. No thrombosis.', true),
h3('Prescription: Conservative Only'),
makeTable(
['Treatment', 'Dose / Application', 'Frequency', 'Duration'],
[
['Psyllium husk', '5–10 g in water', 'Daily', 'Ongoing'],
['Docusate sodium', '100 mg', 'Twice daily', '2–4 weeks'],
['Pramoxine 1% cream', 'Apply to anal area', '3–4 times daily', 'Max 14 days'],
['Witch hazel pads', 'Apply to perianal area', 'After each stool', 'As needed'],
['Hydrocortisone 1%', 'Thin layer', 'Twice daily', 'Max 7 days for pruritus'],
['Warm sitz baths', '10–15 min warm water', '2–3 times daily', 'Ongoing'],
],
[2500, 2500, 1800, 2200]
),
p('Skin tag removal is an ELECTIVE, cosmetic procedure. Not routinely recommended unless causing significant hygiene disturbance. Performed under local anesthesia outpatient.'),
new Paragraph({ spacing: { after: 120 } }),
h2('CASE TYPE 6: Thrombosed External Hemorrhoid (TEH) — ACUTE'),
p('Presentation: Sudden onset severe perianal pain; firm, tense, blue-purple perianal lump; typically onset within last 48–72 hours.', true),
warning('TIME-SENSITIVE DECISION: Act within 72 hours of onset for best outcomes.'),
h3('Decision Tree: Surgical vs Conservative'),
makeTable(
['Presentation', 'Treatment Decision', 'Rationale'],
[
['< 72 hours onset + severe pain or enlarging', 'SURGICAL EXCISION under local anesthesia', 'Faster resolution, lower recurrence, longer remission'],
['> 72 hours onset OR pain improving / tolerable', 'CONSERVATIVE MANAGEMENT', 'Thrombus organizes; surgical risk > benefit after 72 hrs'],
],
[2500, 3000, 3500]
),
h3('A. Surgical Excision Protocol (within 72 hours)'),
p('Excision of thrombus WITH overlying skin (not simple drainage — prevents recurrence)'),
makeTable(
['Drug', 'Dose', 'Route', 'Notes'],
[
['Lidocaine 1–2% + epinephrine 1:200,000', '3–5 mL', 'Subcutaneous perianal infiltration', 'Local anesthetic of choice'],
['Bupivacaine 0.25–0.5%', '3–5 mL', 'Subcutaneous perianal infiltration', 'Long-acting alternative (8–12 hr duration)'],
],
[2800, 1200, 2800, 2200]
),
h3('Post-Excision Prescription'),
makeTable(
['Drug', 'Dose', 'Frequency', 'Duration'],
[
['Paracetamol 500–1000 mg', '500–1000 mg', 'Every 6–8 hours PRN', '3–5 days'],
['Ibuprofen 400 mg', '400 mg with food', 'Every 8 hours', '3–5 days'],
['Docusate sodium', '100 mg', 'Twice daily', '1–2 weeks'],
['Sitz baths', 'Warm water 10–15 min', '2–3 times daily', '1–2 weeks'],
],
[2500, 2000, 2500, 2000]
),
h3('B. Conservative Management (beyond 72 hours, or improving symptoms)'),
makeTable(
['Drug/Measure', 'Dose', 'Frequency', 'Duration'],
[
['Warm sitz baths', '10–15 min warm water', '2–3 times daily', '1–2 weeks until resolution'],
['Ibuprofen 400 mg', '400 mg with food', 'Every 8 hours', '5–7 days (anti-inflammatory)'],
['Docusate sodium 100 mg', '100 mg', 'Twice daily', '2 weeks'],
['Topical lidocaine 5% ointment', 'Apply to lump', '3–4 times daily', 'Until pain resolves'],
['Witch hazel pads', 'Apply to perianal area', 'After each stool', 'Until resolution'],
['MPFF (Daflon) 500 mg', '500 mg', 'Twice daily', '7–10 day acute course'],
['Psyllium husk', '5–10 g in water', 'Daily', 'Ongoing to prevent recurrence'],
],
[2500, 1800, 1800, 1900]
),
p('Most thrombosed external hemorrhoids RESOLVE within 48–72 hours on conservative management without intervention.'),
new Paragraph({ children: [new PageBreak()] }),
// ══════════════════════════════════════════════
// SECTION 5: SPECIAL POPULATIONS
// ══════════════════════════════════════════════
h1('SECTION 5: SPECIAL POPULATIONS — PRESCRIPTION ADAPTATIONS'),
h2('CASE TYPE 7: Hemorrhoids in Pregnancy'),
p('Common in 2nd–3rd trimester and postpartum. Mostly Grades I–III. Office procedures contraindicated during pregnancy and ≤ 8 weeks postpartum.', true),
warning('ALL invasive procedures (RBL, sclerotherapy, IRC) are CONTRAINDICATED during pregnancy and for 8 weeks postpartum.'),
makeTable(
['Drug', 'Dose', 'Frequency', 'Duration', 'Safety Profile'],
[
['Psyllium husk', '5–10 g in water', 'Daily', 'Ongoing — safest option', 'Safe in all trimesters'],
['Lactulose', '15–30 mL', 'Once or twice daily', 'As needed', 'Safe in pregnancy'],
['Docusate sodium 100 mg', '100 mg', 'Twice daily', 'Short-term', 'Generally considered safe'],
['Pramoxine 1% cream', 'Apply topically', '3–4 times daily', 'Short-term', 'Minimal systemic absorption; preferred over lidocaine'],
['Witch hazel pads', 'Topical application', 'After each stool', 'As needed', 'Safe topically'],
['Warm sitz baths', '10–15 min warm water', '2–3 times daily', 'As needed', 'Safe and beneficial'],
['MPFF (Daflon)', '500 mg', 'Twice daily', 'Short-term acute only; AVOID 1st trimester', 'Limited data; use if benefit > risk in 2nd–3rd trimester'],
['Hydrocortisone 1%', 'Thin layer sparingly', 'Twice daily', 'Max 5–7 days only', 'Avoid prolonged use; low-potency only'],
],
[2000, 1400, 1800, 2200, 1600]
),
bullet('AVOID: NSAIDs in 3rd trimester (risk of premature ductus arteriosus closure)'),
bullet('AVOID: Castor oil laxatives — uterotonic effect'),
bullet('AVOID: Oral phlebotonics in 1st trimester'),
new Paragraph({ spacing: { after: 120 } }),
h2('CASE TYPE 8: Hemorrhoids on Anticoagulation (Warfarin, NOACs, Antiplatelet)'),
warning('RBL is RELATIVELY CONTRAINDICATED in anticoagulated patients — risk of delayed hemorrhage at band slough (day 7–14).'),
makeTable(
['Procedure', 'Safety', 'Recommendation'],
[
['Sclerotherapy (5% phenol)', 'SAFE', 'PREFERRED office procedure; digital pressure controls needle site bleeding'],
['Infrared Coagulation (IRC)', 'Acceptable', 'Less bleeding risk than RBL'],
['Rubber Band Ligation (RBL)', 'Relatively contraindicated', 'Only if anticoagulation can be held 7 days before and 7 days after'],
['Surgical hemorrhoidectomy', 'Higher risk', 'Requires hematology bridging consultation'],
],
[2500, 1600, 4900]
),
p('Drug Management: Hold aspirin-containing products 7 days pre- and post-procedure if possible. For warfarin: INR should be in therapeutic range before any procedure. Continue fiber and stool softeners as standard.'),
new Paragraph({ spacing: { after: 120 } }),
h2('CASE TYPE 9: Hemorrhoids with Portal Hypertension / Anorectal Varices'),
warning('RBL is ABSOLUTELY CONTRAINDICATED in portal hypertension — risk of massive, life-threatening delayed hemorrhage.'),
p('Distinguish hemorrhoids from anorectal varices: varices are compressible, refill rapidly, extend across dentate line into rectum.'),
makeTable(
['Scenario', 'Treatment'],
[
['Hemorrhoids in portal hypertension (confirmed, not varices)', 'Sclerotherapy preferred; aggressive conservative management'],
['Anorectal varices with bleeding', 'Underrunning with absorbable suture; inferior mesenteric vein embolization; TIPS if needed'],
['Portal hypertension + hemorrhoids (mild)', 'Manage portal hypertension (propranolol/carvedilol) first; avoid interventional procedures if possible'],
],
[3000, 6000]
),
new Paragraph({ spacing: { after: 120 } }),
h2('CASE TYPE 10: Immunocompromised Patients (HIV/AIDS, Active Chemotherapy)'),
warning('RBL is CONTRAINDICATED in immunocompromised patients — risk of life-threatening pelvic sepsis.'),
makeTable(
['Treatment', 'Recommendation'],
[
['Conservative medical management', 'FIRST-LINE; preferred indefinitely until immune status improves'],
['Sclerotherapy', 'Better-studied and preferred over IRC in this population'],
['Rubber Band Ligation', 'CONTRAINDICATED — high infection and sepsis risk'],
['Surgery', 'High risk; delay until CD4 > 200 cells/µL or remission achieved'],
],
[3500, 5500]
),
new Paragraph({ children: [new PageBreak()] }),
// ══════════════════════════════════════════════
// SECTION 6: MIXED & ACUTE HEMORRHOIDAL CRISIS
// ══════════════════════════════════════════════
h1('SECTION 6: MIXED HEMORRHOIDS & ACUTE HEMORRHOIDAL CRISIS'),
h2('CASE TYPE 11: Mixed Internal + External Hemorrhoids'),
p('Presentation: Combination of internal Grade II–III and external hemorrhoids; prolapse with painful external component.', true),
p('Office procedures do NOT address the external component. Conventional excisional hemorrhoidectomy is the definitive treatment for symptomatic mixed disease.'),
makeTable(
['Step', 'Treatment', 'Notes'],
[
['Medical bridge (mild–moderate)', 'MPFF 500 mg BD + fiber + stool softeners', 'As bridge to definitive procedure'],
['Definitive', 'Conventional hemorrhoidectomy (Milligan-Morgan or Ferguson)', 'Addresses both internal and external components'],
['Alternative (minimal external)', 'RBL for internal + conservative for external', 'Only if external component is minor/non-symptomatic'],
],
[1400, 3500, 4100]
),
new Paragraph({ spacing: { after: 120 } }),
h2('CASE TYPE 12: Acute Hemorrhoidal Crisis / Mass Prolapse'),
p('Presentation: All three hemorrhoidal columns prolapsed, edematous, irreducible; severe pain; unable to sit.', true),
warning('Mass prolapse = surgical emergency. Urgent colorectal surgery consultation required.'),
makeTable(
['Drug', 'Dose', 'Route', 'Frequency', 'Duration'],
[
['Morphine 2–4 mg', '2–4 mg', 'IV/IM', 'Every 2–4 hours PRN', 'Acute admission'],
['MPFF (Daflon) — Acute Protocol', '1500 mg Days 1–4; 1000 mg Days 5–7', 'Oral', 'Daily', '7 days'],
['Ice packs to perineum', 'As tolerated', 'Topical', 'Every 2 hours for first 24 hrs', 'First 24–48 hrs only'],
['Diclofenac sodium 75 mg', '75 mg', 'IM/IV', 'Every 12 hours', '24–48 hrs acute phase'],
['Broad-spectrum antibiotics if infected', 'Piperacillin/tazobactam 4.5 g', 'IV', 'Every 8 hours', '5–7 days'],
],
[2200, 1800, 1200, 1800, 2000]
),
new Paragraph({ children: [new PageBreak()] }),
// ══════════════════════════════════════════════
// SECTION 7: QUICK REFERENCE MASTER TABLE
// ══════════════════════════════════════════════
h1('SECTION 7: MASTER QUICK-REFERENCE PRESCRIPTION TABLE'),
makeTable(
['Drug Class', 'Drug', 'Dose', 'Frequency', 'Duration', 'Grade Indication'],
[
['Fiber supplement', 'Psyllium husk (Ispaghula)', '5–10 g in 240 mL water', '1–3x daily', 'Long-term', 'ALL grades'],
['Stool softener', 'Docusate sodium', '100 mg', 'Twice daily', '2–4 weeks', 'ALL grades'],
['Osmotic laxative', 'Lactulose', '15–30 mL', 'Once–twice daily', 'Short–medium term', 'ALL grades, post-op'],
['Osmotic laxative', 'Polyethylene glycol 3350', '17 g in water', 'Once daily', 'Short–medium term', 'Constipation-predominant'],
['Topical anesthetic', 'Lidocaine 5% ointment', 'Apply topically', '3–4x daily', 'Max 14 days', 'External/symptomatic I–II'],
['Topical anesthetic', 'Pramoxine 1% cream', 'Apply topically', '3–4x daily', 'Max 14 days', 'External/symptomatic; pregnancy safe'],
['Topical anesthetic', 'Dibucaine 0.5–1%', 'Apply topically', '3x daily', 'Max 14 days', 'External/symptomatic'],
['Topical steroid', 'Hydrocortisone 1–2.5%', 'Thin layer', 'Twice daily', 'MAX 7 days', 'Pruritus short-term only'],
['Phlebotonic', 'MPFF / Daflon 500 mg', '500 mg', 'Twice daily', 'Acute 2–3 months; short courses only', 'Grade I–III; Grade A evidence'],
['Phlebotonic', 'Diosmin 600 mg', '600 mg', 'Twice daily', 'Short-term acute', 'Grade I–III'],
['Phlebotonic', 'Calcium dobesilate', '500 mg', 'Three times daily', 'Short-term ONLY', 'Caution: agranulocytosis risk'],
['Analgesic', 'Paracetamol', '500–1000 mg', 'Every 6–8 hours PRN', '3–7 days', 'Post-procedure/surgery pain'],
['Analgesic', 'Paracetamol + Codeine 30 mg', '500/30 mg', 'Every 4–6 hours PRN', '5–7 days', 'Post-hemorrhoidectomy'],
['NSAID', 'Ibuprofen', '400 mg with food', 'Every 8 hours', '3–7 days', 'TEH, post-procedure, post-op'],
['NSAID', 'Diclofenac sodium', '50–75 mg with food/IM', 'Every 8–12 hours', '3–5 days', 'Moderate–severe pain; acute crisis'],
['Antibiotic', 'Metronidazole 400 mg', '400 mg', 'Three times daily', '7–10 days', 'Post-hemorrhoidectomy pain reduction'],
['Antibiotic', 'Ceftriaxone 1–2 g', '1–2 g', 'Once daily IV', '5–7 days', 'Perianal/pelvic sepsis cover'],
['Antibiotic', 'Pip/Taz 4.5 g', '4.5 g', 'Every 8 hours IV', '5–7 days', 'Emergency gangrenous hemorrhoids'],
['Topical post-op', 'GTN 0.2–0.4% ointment', 'Thin perianal layer', '2–3x daily', '4–8 weeks', 'Post-hemorrhoidectomy pain + healing'],
['Topical post-op', 'Lidocaine 2% gel', 'Apply to wound', '3–4x daily', '1–2 weeks', 'Post-op wound analgesia'],
['Sclerosant', '5% phenol in oil', '2–3 mL per column', 'Single session (repeat 4–6 wk)', 'As needed', 'Grade I–II; anticoagulated patients'],
['Local anesthetic', 'Lidocaine 1–2% + epinephrine 1:200,000', '3–5 mL perianal', 'Single use', 'Procedure only', 'TEH excision; perianal block'],
['Local anesthetic', 'Bupivacaine 0.25–0.5%', '3–5 mL perianal', 'Single use', 'Procedure only (8–12 hr action)', 'Long-acting alternative for excision'],
['Opioid', 'Morphine sulfate', '2–4 mg', 'Every 2–4 hours PRN IV', 'Acute admission', 'Grade IV incarcerated; acute crisis'],
],
[1500, 2000, 1500, 1500, 1700, 1800]
),
new Paragraph({ spacing: { after: 200 } }),
// ─── SOURCES ─────────────────────────────────
h2('Sources'),
bullet('Pfenninger and Fowler\'s Procedures for Primary Care, 3rd Edition'),
bullet('Sleisenger and Fordtran\'s Gastrointestinal and Liver Disease, 11th Edition'),
bullet('Yamada\'s Textbook of Gastroenterology, 7th Edition'),
bullet('Sabiston Textbook of Surgery, 21st Edition'),
bullet('Current Surgical Therapy, 14th Edition'),
bullet('ASCRS Clinical Practice Guidelines for Hemorrhoids Management, May 2024'),
bullet('Saudi IDF/SFDA Hemorrhoids Indication Update (CHI CPG)'),
bullet('ACG Clinical Guidelines: Management of Benign Anorectal Disorders (2021)'),
bullet('PMID 40596934 — Meta-analysis: surgical vs conservative hemorrhoid treatment (2025)'),
bullet('PMID 40576944 — Systematic review: operative vs nonoperative thrombosed external hemorrhoids (2026)'),
new Paragraph({ spacing: { after: 100 } }),
new Paragraph({
children: [new TextRun({ text: 'Generated by Orris Medical AI | June 2026 | For educational and clinical reference use only. Always verify doses against current local formulary.', size: 18, color: '7F8C8D', italics: true })],
alignment: AlignmentType.CENTER,
}),
],
},
],
});
Packer.toBuffer(doc).then((buffer) => {
fs.writeFileSync('/home/daytona/workspace/piles-treatment/Piles_Hemorrhoids_Treatment_Guide.docx', buffer);
console.log('SUCCESS: Document written');
}).catch(err => {
console.error('ERROR:', err);
process.exit(1);
});