Venous hyperemia Definition, Etiology, pathogenesis clinical features and treatment
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
I now have excellent material from both editions of Robbins Pathology. Let me compile a comprehensive answer.
Venous Hyperemia (Passive Hyperemia / Chronic Passive Congestion)
Definition
Venous hyperemia - also called passive hyperemia or congestion - refers to an increase in blood volume within a tissue resulting from impaired venous outflow. It is a passive process, meaning the blood accumulates because it cannot drain away, not because inflow is increased. This distinguishes it fundamentally from active hyperemia, which results from arteriolar dilation and increased inflow (e.g., at sites of inflammation).
"Congestion is a passive process resulting from impaired outflow of venous blood from a tissue." - Robbins & Kumar Basic Pathology, p. 77
Etiology
Venous hyperemia can occur systemically or locally:
Systemic Causes
- Congestive heart failure (CHF) - the most important systemic cause
- Left heart failure: causes pulmonary venous congestion
- Right heart failure: causes systemic venous congestion (liver, spleen, peripheral tissues)
- Constrictive pericarditis
- Cor pulmonale
Local Causes
- Venous obstruction - thrombosis (DVT), external compression by tumor, lymph node, pregnancy
- Venous valvular insufficiency (varicose veins, lower limb)
- Portal hypertension - hepatic cirrhosis causing splanchnic congestion
- Budd-Chiari syndrome - hepatic vein obstruction
Pathogenesis
The underlying mechanism is straightforward: obstruction or failure of venous drainage raises intravascular hydrostatic pressure upstream of the obstruction. This elevated pressure drives a sequence of events:
- Blood stagnates in venules and capillaries - reduced velocity allows more oxygen extraction, causing hemoglobin to become deoxygenated
- Cyanosis - deoxygenated hemoglobin imparts a blue-red discoloration to the affected tissues
- Elevated capillary hydrostatic pressure forces fluid into the interstitium → edema
- Chronic hypoxia - persistent low-oxygen delivery causes ischemic injury to parenchymal cells
- Capillary rupture - elevated pressure can rupture small vessels, producing focal hemorrhages; red cells are phagocytosed by macrophages, which then become laden with hemosiderin (a telltale sign of old hemorrhage)
- Fibrosis - chronic ischemic injury and cell death trigger reactive scarring
"In long-standing chronic congestion, inadequate tissue perfusion and persistent hypoxia may lead to parenchymal cell death and secondary tissue fibrosis, and elevated intravascular pressures may cause edema or rupture capillaries, producing focal hemorrhages." - Robbins & Kumar Basic Pathology, p. 77
Clinical Features
General Signs
- Cyanosis (blue-red discoloration) of affected tissues - due to deoxygenated hemoglobin
- Edema - pitting edema in lower limbs (systemic), pulmonary crackles (pulmonary)
- Organ enlargement - hepatomegaly, splenomegaly
- Tenderness over engorged organs
Organ-Specific Features
Lungs (Pulmonary Congestion - Left Heart Failure)
- Dyspnea, orthopnea, paroxysmal nocturnal dyspnea
- Fine crepitations (rales) at lung bases
- Acute: blood-engorged alveolar capillaries, alveolar septal edema, intraalveolar hemorrhage
- Chronic: septa become thickened and fibrotic; alveoli contain hemosiderin-laden macrophages ("heart failure cells"); may progress to "brown induration" of the lung
Liver (Hepatic Congestion - Right Heart Failure)
- Hepatomegaly with tenderness (stretching of Glisson's capsule)
- Jaundice (mild, due to centrilobular hepatocyte necrosis)
- Elevated liver enzymes (AST, ALT)
- Acute: central vein and sinusoids are distended; centrilobular hepatocyte necrosis
- Chronic: the classic "nutmeg liver" - centrilobular areas appear red-brown and slightly depressed surrounded by tan, sometimes fatty, periportal hepatocytes; in severe cases → cardiac cirrhosis ("cardiac fibrosis")
Lower Limbs (Peripheral Venous Congestion)
- Pitting edema, varicosities
- Stasis dermatitis, skin pigmentation (hemosiderin deposition)
- Venous ulcers (especially above medial malleolus)
Morphology Summary
| Setting | Acute | Chronic |
|---|---|---|
| Lung | Engorged capillaries, septal edema, alveolar hemorrhage | Septal fibrosis, "heart failure cells" (hemosiderin macrophages), brown induration |
| Liver | Dilated central veins and sinusoids, centrilobular necrosis | "Nutmeg liver," centrilobular hemorrhage, hemosiderin macrophages, cardiac cirrhosis |
| Lower limbs | Edema, varicosities | Stasis dermatitis, ulcers, skin pigmentation |
Pathological Image
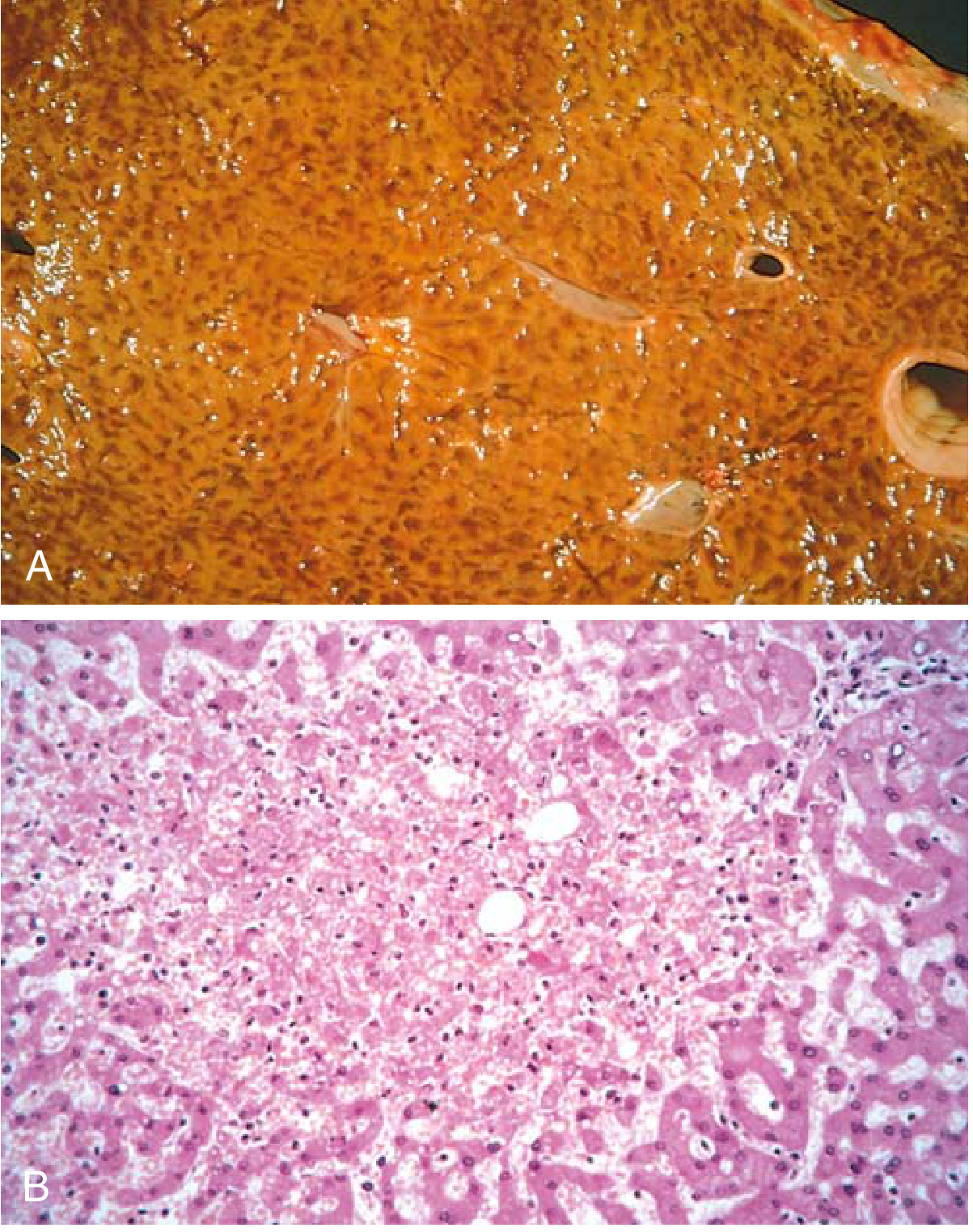
Fig. A (Gross): "Nutmeg liver" - centrilobular areas appear red-brown and depressed against tan periportal parenchyma.
Fig. B (Microscopic): Centrilobular congestion, hemorrhage, and hepatocyte necrosis.
(From Robbins & Kumar Basic Pathology)
Treatment
Treatment is directed at the underlying cause of impaired venous outflow:
Systemic Venous Congestion (Heart Failure)
- Diuretics (furosemide, spironolactone) - reduce fluid overload and venous pressure - this is the cornerstone
- ACE inhibitors / ARBs / ARNIs (sacubitril-valsartan) - reduce afterload and preload, slow cardiac remodeling
- Beta-blockers - reduce heart rate and improve cardiac output
- Digitalis - positive inotrope in selected patients
- Sodium and fluid restriction
- Treat the precipitating cause (ischemia, hypertension, valvular disease)
Pulmonary Congestion (Acute)
- Supplemental oxygen
- Upright positioning (orthopnea posture)
- IV furosemide (rapid venodilation + diuresis)
- Morphine (venodilation, reduces anxiety) - used cautiously
- Nitrates (IV nitroglycerin) - venodilation, reduces preload
Local Venous Congestion (Venous Insufficiency/DVT)
- Compression stockings - reduce lower limb venous pressure
- Elevation of affected limb
- Anticoagulation for DVT (heparin, then warfarin or DOACs)
- Surgical/interventional: venous valve repair, stenting of obstructed veins, varicose vein stripping or sclerotherapy
- For venous malformations: head/neck elevation, sclerotherapy, surgical excision
Prevention of Complications
- Wound care for stasis ulcers
- Monitoring and managing cardiac cirrhosis (treat right heart failure to prevent progression)
Sources: Robbins & Kumar Basic Pathology, p. 77; Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 57, 102, 119
This is a shared conversation. Sign in to Orris to start your own chat.