VT with pulse with hypercalcemia
Reading File
Finding Sources
Finding Sources
Searching PubMed
ventricular tachycardia hypercalcemia treatment
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have all the material needed for a thorough, well-sourced answer.
VT with Pulse in the Setting of Hypercalcemia
Why Hypercalcemia Causes VT
Calcium plays a central role in cardiac myocyte action potential phase 2 (the plateau phase). Excess extracellular calcium shortens the plateau and action potential duration, which is why the classic ECG finding is a shortened QT interval. In severe hypercalcemia (>14 mg/dL), the membrane becomes increasingly unstable and can generate malignant ventricular arrhythmias. Other ECG findings in hypercalcemia include:
- Short QT (most recognized sign, though not always reliable)
- ST segment elevation (can mimic STEMI - an important pitfall)
- U waves despite normokalemia
- Osborn waves despite normothermia
- Bradydysrhythmias (most common cardiac finding overall)
- Sinus arrest, high-degree AV block
- Atrial fibrillation, and at the extreme end - ventricular tachycardia and ventricular fibrillation
ECG from a patient with multiple myeloma and Ca²⁺ of 14.2 mg/dL showing short QT (arrow):
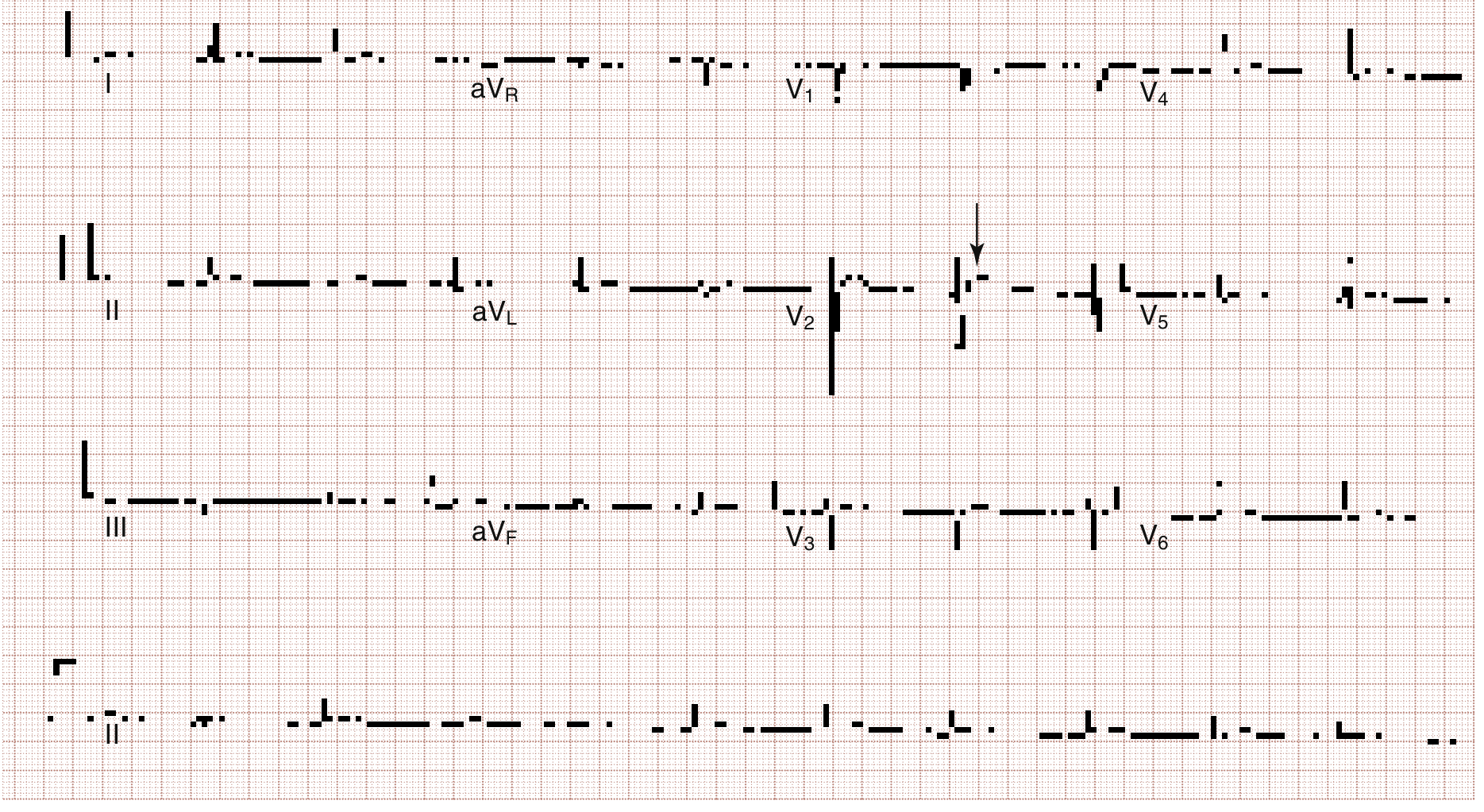
Fig. 114.6 - Rosen's Emergency Medicine
Step 1: Assess Hemodynamic Stability
VT with a pulse must first be classified by hemodynamic status, because this drives everything:
| Status | Definition | Immediate Action |
|---|---|---|
| Unstable | Hypotension, altered consciousness, chest pain, pulmonary edema | Immediate synchronized cardioversion |
| Stable | Adequate BP, alert, tolerating the rhythm | Pharmacologic cardioversion first |
Step 2: Treat the Underlying Cause - Hypercalcemia
This is the cornerstone. Antiarrhythmics alone will not provide durable termination if the metabolic trigger persists. Treat aggressively and simultaneously:
Aggressive IV Saline (First and Most Important)
- Normal saline "wide open" until BP and perfusion normalize
- Then 200-300 mL/hr adjusted to patient's renal and cardiac function
- Target urine output: ~2 L/day
- Saline works by inhibiting proximal tubular reabsorption of calcium
Loop Diuretics
- Not routine - furosemide is no longer recommended as standard treatment
- Reserve only for volume overload prevention once the patient is volume-replete
- Giving furosemide to a volume-depleted patient worsens hypercalcemia
Bisphosphonates (for severe/malignancy-related cases)
- Zoledronic acid is the bisphosphonate of choice
- Used when Ca²⁺ >15 mg/dL with rapid CNS, cardiac, GI, or renal deterioration
- Infusion over 15 minutes; sustained calcium-lowering effect
- Mechanism: inhibits osteoclast function and survival
Denosumab
- Option for hypercalcemia of malignancy refractory to bisphosphonates
Calcitonin, Glucocorticoids, Mithramycin
- Additional osteoclast-inhibiting agents; consult with oncology/endocrinology
Hemodialysis
- For life-threatening hypercalcemic arrhythmias or heart block when other measures fail
- This is the definitive intervention for refractory cases with cardiac compromise
Treat Electrolyte Co-Disturbances
- Monitor potassium closely during saline diuresis - hypokalemia can compound arrhythmia risk
- Check and correct magnesium
Step 3: Antiarrhythmic Management of the VT Itself
If Unstable (any sign of hemodynamic compromise):
- Immediate synchronized cardioversion (25-50 J for monomorphic VT, higher energy if ineffective)
- Airway management and sedation if clinical status allows
If Stable:
Pharmacologic cardioversion is first-line. Per Tintinalli's:
- Procainamide - Superior to amiodarone or lidocaine for converting stable VT. Disadvantage: slow infusion required to avoid hypotension
- Amiodarone - Commonly used for stable VT; especially for slower, hemodynamically stable VT
- Lidocaine - Alternative agent; also consider for post-ROSC maintenance if used for pulseless VT
- Magnesium - If hypomagnesemia, polymorphic VT, or QT prolongation is a concern
If the patient deteriorates during pharmacologic treatment, escalate immediately to synchronized cardioversion.
Important Caveats Specific to Hypercalcemia-Induced VT:
- Avoid calcium channel blockers (verapamil, diltiazem) - these are not indicated and calcium is already elevated
- Avoid agents that prolong QT - though hypercalcemia shortens QT, concomitant electrolyte disturbances (hypokalemia, hypomagnesemia) may coexist
- Hemodialysis should be considered early if the VT is refractory and hypercalcemia is severe
- Cardiology consult for stable VT refractory to standard pharmacologic therapy - unusual forms may require electrophysiologic evaluation
Disposition
Patients with arrhythmias from hypercalcemia require admission to a monitored ICU-level setting. Involve hematology/oncology and palliative care early if the underlying cause is malignancy.
Summary Algorithm
VT with Pulse + Hypercalcemia
|
Hemodynamically stable?
/ \
YES NO
| |
Pharmacologic Rx Immediate Synchronized
(Procainamide 1st, Cardioversion
Amiodarone, Lido)
|
SIMULTANEOUS:
- IV NS wide open → 200-300 mL/hr
- Monitor K+, Mg²⁺
- Bisphosphonate if Ca²⁺ >15 mg/dL
- Hemodialysis if life-threatening/refractory
- Treat underlying cause
Sources: Rosen's Emergency Medicine (9780323757898), Tintinalli's Emergency Medicine (9781260019933), Goldman-Cecil Medicine (9780323930345), Sabiston Textbook of Surgery (9780443124341)
This is a shared conversation. Sign in to Orris to start your own chat.