Bleeding in early pregnancy
Reading File
Finding Sources
Finding Sources
Searching PubMed
"early pregnancy bleeding" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed to write a thorough, well-organized answer. Here is the complete response:
Bleeding in Early Pregnancy
Bleeding in early pregnancy (before 20 weeks' gestation) is common, affecting up to 20% of all pregnancies. Approximately 50% of women who bleed in early pregnancy will go on to miscarry. The priority in assessment is always to exclude ectopic pregnancy, which is the leading cause of first-trimester maternal death.
Causes
| Cause | Notes |
|---|---|
| Threatened miscarriage | Most common cause; closed cervical os |
| Inevitable / incomplete / complete miscarriage | Varying degrees of cervical dilatation and tissue passage |
| Ectopic pregnancy | ~10% of ED patients presenting with 1st-trimester pain or bleeding |
| Implantation bleeding | Minor bleeding at time of blastocyst implantation |
| Molar pregnancy (GTD) | Often late 1st / early 2nd trimester |
| Ruptured corpus luteum cyst | Can mimic ectopic |
| Cervical or vaginal lesions | Trauma, polyps, cervicitis, ectropion |
| Subchorionic haemorrhage | Seen on ultrasound |
- ROSEN's Emergency Medicine, p. 333
Miscarriage - Classification
1. Clinical classification (history + exam):
| Type | Features |
|---|---|
| Threatened | Vaginal bleeding ± cramping; cervical os closed; pregnancy still viable |
| Inevitable | Cervical os open, no tissue passed yet |
| Incomplete | Os open; some products of conception (POC) passed, some retained |
| Complete | All POC expelled; os closed; uterus contracted |
| Missed (anembryonic/delayed) | Fetal demise with no uterine activity; no expulsion |
| Septic | Miscarriage complicated by intrauterine infection (fever, uterine tenderness) |
| Recurrent | Three or more consecutive pregnancy losses |
2. Ultrasound-based classification:
- Embryonic/fetal demise: CRL 5-40 mm, no cardiac activity
- Anembryonic pregnancy (blighted ovum): Gestational sac mean diameter 16-45 mm, no fetal pole
- Swanson's Family Medicine Review, p. 434
Ectopic Pregnancy
Critical points:
- Implants most commonly in the fallopian tube; accounts for ~1-2% of all pregnancies
- Prevalence in ED patients with 1st-trimester bleeding or pain: up to 10-16%
- Half of women with ectopic pregnancy have no identifiable risk factors
Risk factors:
- Pelvic inflammatory disease (PID) - raises risk 3-fold
- Prior ectopic pregnancy (subsequent risk up to 22%)
- Previous tubal surgery or sterilization
- Intrauterine device (IUD) in situ
- Assisted reproductive technologies (especially IVF with multiple embryo transfer - also raises risk of heterotopic pregnancy)
- Smoking, infertility, advanced age
Clinical presentation: Range from mild unilateral pelvic pain and spotting to haemorrhagic shock. An ectopic pregnancy can mimic a threatened miscarriage and should NEVER be excluded based on symptoms alone.
- ROSEN's Emergency Medicine, p. 3350
Investigation
1. Urine / serum beta-hCG
- Confirm pregnancy first in any woman of reproductive age
- Serial quantitative beta-hCG: In a normal IUP, hCG doubles approximately every 48 hours in early pregnancy; a failing or ectopic pregnancy typically shows a slower rise or plateau
- A single hCG level cannot diagnose viability or location - serial measurements are needed
- There is no hCG level at which ectopic pregnancy can be completely excluded
2. Transvaginal Ultrasound (TVUS) - First-line imaging
Landmarks on TVUS:
| Finding | Weeks from LMP | beta-hCG (mIU/mL) |
|---|---|---|
| Gestational sac | 5 | ~1,000 |
| Yolk sac (first definitive IUP sign) | 6 | ~2,000 |
| Fetal pole | 7 | ~5,700 |
| Fetal heart motion | 6-7 | ~7,000 |
- Discriminatory zone: Traditionally 2,000 IU/mL, but ACOG now recommends using 3,500 IU/mL to avoid inadvertently disrupting a viable IUP
- Pregnancy of Unknown Location (PUL): Positive pregnancy test with neither IUP nor ectopic seen on USS - requires serial hCG + repeat TVUS in 48 hours
3. Other bloods (in haemodynamically unstable patients)
- Full blood count
- Blood group and Rh status
- Crossmatch
- Coagulation screen
Diagnostic Algorithm
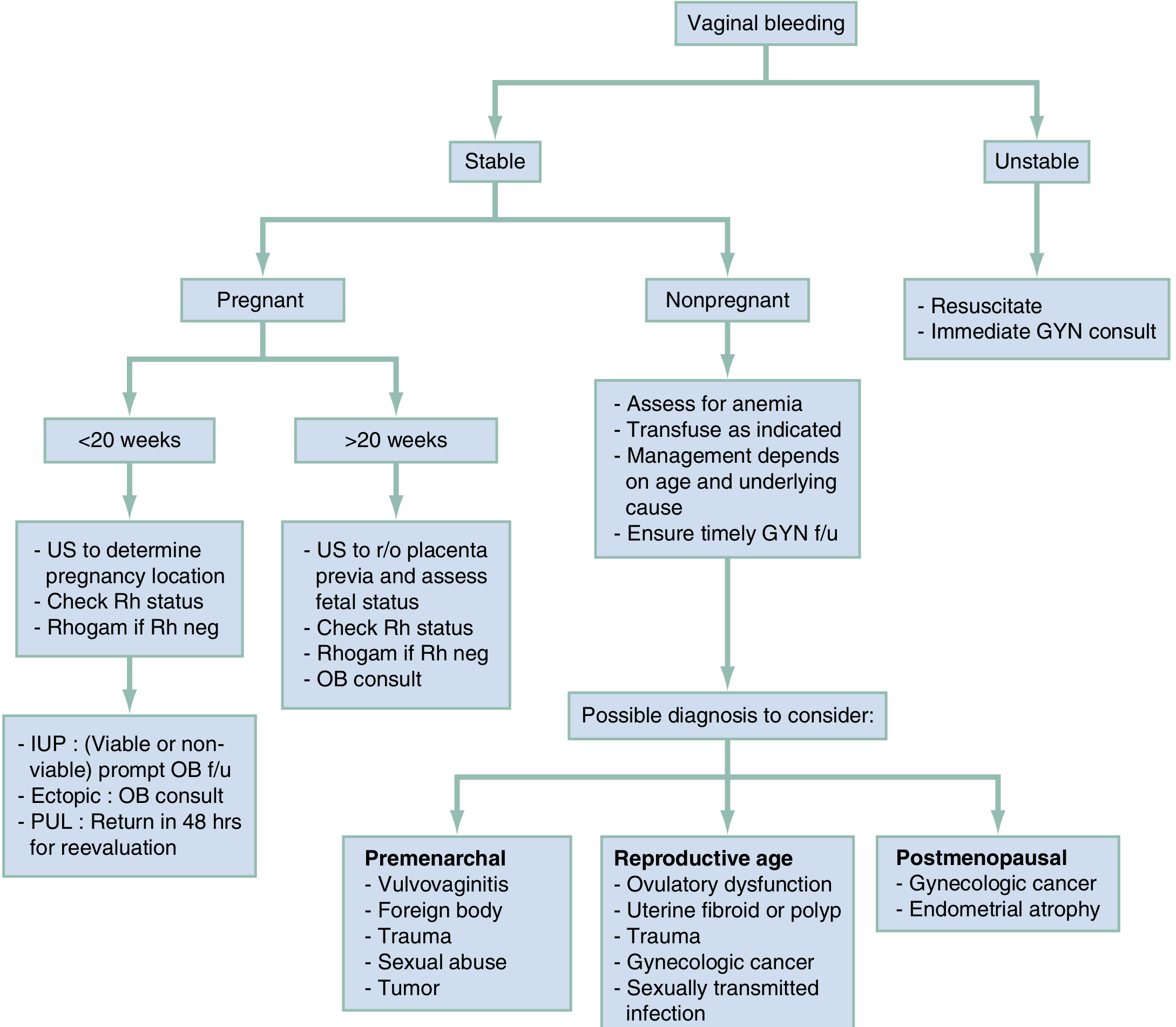
Adapted from ROSEN's Emergency Medicine - Diagnostic Algorithm for Vaginal Bleeding
Management
Haemodynamically unstable patient
- Immediate resuscitation: IV access, crystalloid, then blood (use Rh-negative blood if Rh status unknown)
- Urgent obstetric/gynaecology consultation
- If confirmed or suspected ectopic or IUP with haemorrhage: operative management
Miscarriage - Stable patient
Three options: Expectant, Medical, or Surgical
| Option | Details |
|---|---|
| Expectant | Monitor with clinical symptoms, serial hCG, and serial USS. Appropriate for motivated patients with complete or threatened miscarriage |
| Medical | Misoprostol (prostaglandin E1 analogue) given intravaginally - most effective for incomplete or inevitable miscarriage; less effective for anembryonic pregnancy or fetal demise |
| Surgical | Uterine aspiration by manual vacuum aspiration (60 mL syringe) or electric vacuum; can be done safely under local anaesthesia as an outpatient; D&C in theatre for failed medical/expectant management |
Ectopic Pregnancy - Stable patient
- Medical: Methotrexate (folic acid antagonist) - suitable for haemodynamically stable, unruptured ectopic with hCG typically <5,000 IU/mL, no fetal cardiac activity on USS
- Surgical: Salpingostomy or salpingectomy (laparoscopic preferred); mandatory for ruptured ectopic or failed methotrexate
Rh-negative patients
- Anti-D (RhoGAM 50 mcg) should be given to all Rh-negative women with early pregnancy bleeding to prevent Rh sensitisation
- Swanson's Family Medicine Review, p. 434
Key Points to Remember
- Pregnancy status is the single most important determination in any woman of reproductive age presenting with vaginal bleeding.
- Ectopic pregnancy must be actively excluded in every case - it can present identically to threatened miscarriage.
- A single beta-hCG level cannot confirm or exclude ectopic pregnancy or viability; serial measurements + USS are required.
- When fetal cardiac activity is confirmed on TVUS, the subsequent miscarriage risk drops to only 3-6%, though bleeding remains a high-risk indicator.
- Women who bleed but do not miscarry are still at increased risk for preterm PROM, abruption, previa, stillbirth, and congenital abnormalities.
- All Rh-negative women with any early pregnancy bleeding should receive anti-D prophylaxis.
- Patients with PUL (no pregnancy visible on USS) should return in 48 hours for repeat TVUS and hCG.
Sources: ROSEN's Emergency Medicine (9th ed.), pp. 333, 3348-3351 | Roberts and Hedges' Clinical Procedures in Emergency Medicine | Swanson's Family Medicine Review, p. 434
I want conditions in which early pregnancy bleeding occurs
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I have all the content needed. Here is the comprehensive, condition-by-condition breakdown:
Conditions Causing Bleeding in Early Pregnancy
Bleeding before 20 weeks affects up to 20% of pregnancies. The conditions are best grouped by origin - obstetric (arising from the pregnancy itself) vs. non-obstetric (arising from the genital tract).
A. Obstetric Causes
1. Miscarriage (Spontaneous Abortion)
The most common cause. Defined as pregnancy loss before 20 weeks. Approximately 50% of women who bleed in early pregnancy will miscarry.
| Type | Cervical Os | Key Feature |
|---|---|---|
| Threatened | Closed | Bleeding ± cramping; viable pregnancy still present |
| Inevitable | Open | Bleeding + cramping; no tissue passed yet |
| Incomplete | Open | Some products of conception (POC) passed, some retained |
| Complete | Closed | All POC expelled; uterus contracted |
| Missed (delayed) | Closed | Fetal demise; no expulsion; discovered on USS |
| Septic | Variable | Miscarriage + intrauterine infection (fever, uterine tenderness) |
| Recurrent | - | Three or more consecutive losses |
Pathophysiology:
- 80% of miscarriages occur in the first trimester
- Most are caused by chromosomal abnormalities or uterine malformations
- Fetal death often precedes clinical symptoms by several weeks
- Symptoms most common 8-12 weeks; USS shows death usually before 8 weeks
Risk factors: Advanced maternal/paternal age, prior miscarriage, smoking, alcohol, caffeine, poorly controlled diabetes or thyroid disease, obesity, uterine anomalies, leiomyomas
- ROSEN's Emergency Medicine, p. 3348-3350
2. Ectopic Pregnancy
The most dangerous cause. Must always be excluded. Responsible for ~4-10% of first-trimester maternal deaths.
Definition: Implantation of the fertilized ovum outside the uterine corpus.
Sites of implantation:
- Fallopian tube (most common - ~90%): ampulla > isthmus > fimbrial end
- Ovary
- Abdominal cavity (peritoneal implantation after fimbrial expulsion)
- Cornual/interstitial (uterine horn) - particularly dangerous; can grow to 10-14 weeks before rupture
- Cervix (rare)
Pathophysiology: The growing pregnancy burrows through the tubal wall, causing intratubal haematoma (haematosalpinx) and then intraperitoneal haemorrhage. Blood leaks intermittently through the tubal wall into the peritoneal cavity.
Three possible outcomes:
- Spontaneous involution
- Tubal abortion (expulsion into peritoneal cavity or vagina)
- Rupture - catastrophic, sudden severe abdominal pain, haemorrhagic shock
Clinical features:
- Classic triad: amenorrhoea + abdominal pain + vaginal bleeding
- BUT: 15-20% have no missed period; bleeding may be mild; pain is variable
- Adnexal mass palpable in only 10-20%
- Cervical motion tenderness if peritoneal irritation
- Half of patients have no identifiable risk factors
Risk factors:
- Pelvic inflammatory disease (raises risk ~3-fold; 50% of cases)
- Prior ectopic pregnancy (subsequent risk up to 22%)
- Tubal surgery (sterilization or prior ectopic)
- Intrauterine device (IUD)
- Assisted reproduction / IVF
- Smoking, advanced age, infertility
Heterotopic pregnancy: Simultaneous IUP + ectopic - rare (~1:4000) but significantly more common in IVF patients.
- Robbins & Kumar Basic Pathology, p. 703 | ROSEN's Emergency Medicine, p. 3350
3. Implantation Bleeding
- Occurs at the time of blastocyst implantation into the endometrium (~6-12 days post-conception)
- Can also occur at the time of the first missed menstrual period
- Typically light spotting, self-limiting
- Diagnosis of exclusion - all serious causes must be ruled out
4. Subchorionic Haemorrhage (SCH)
- Blood collects between the chorion and the uterine wall
- Occurs in the first half of pregnancy (1st/early 2nd trimester)
- Incidence: approximately 1.7% of pregnancies
- Presents with vaginal bleeding only (not the dramatic presentation of abruption)
- Diagnosed by TVUS (retroplacental blood clot visible)
- Most SCHs resolve and result in a healthy infant
- Associated with slightly increased risk of: miscarriage (OR 2.18), abruption (OR 5.71), preterm delivery, PPROM

- Creasy & Resnik's Maternal-Fetal Medicine, p. 3465-3474
5. Molar Pregnancy (Gestational Trophoblastic Disease - GTD)
Definition: Abnormal proliferation of placental trophoblastic tissue due to an excess of paternal genetic material.
Types:
| Feature | Complete Mole | Partial Mole |
|---|---|---|
| Karyotype | Diploid (46,XX or 46,XY) - all paternal | Triploid (69,XXY) - 2 paternal + 1 maternal |
| Villous oedema | All villi | Some villi |
| Trophoblast proliferation | Diffuse, circumferential | Focal, slight |
| Fetal parts | Absent (rarely) | Present (sometimes) |
| Serum hCG | Markedly elevated (>100,000 IU/L) | Less elevated |
| Risk of choriocarcinoma | 2.5% | Rare |
Origin:
- Complete mole: empty ovum fertilized by one sperm that duplicates, or by two sperm (dispermy)
- Partial mole: normal ovum fertilized by two sperm
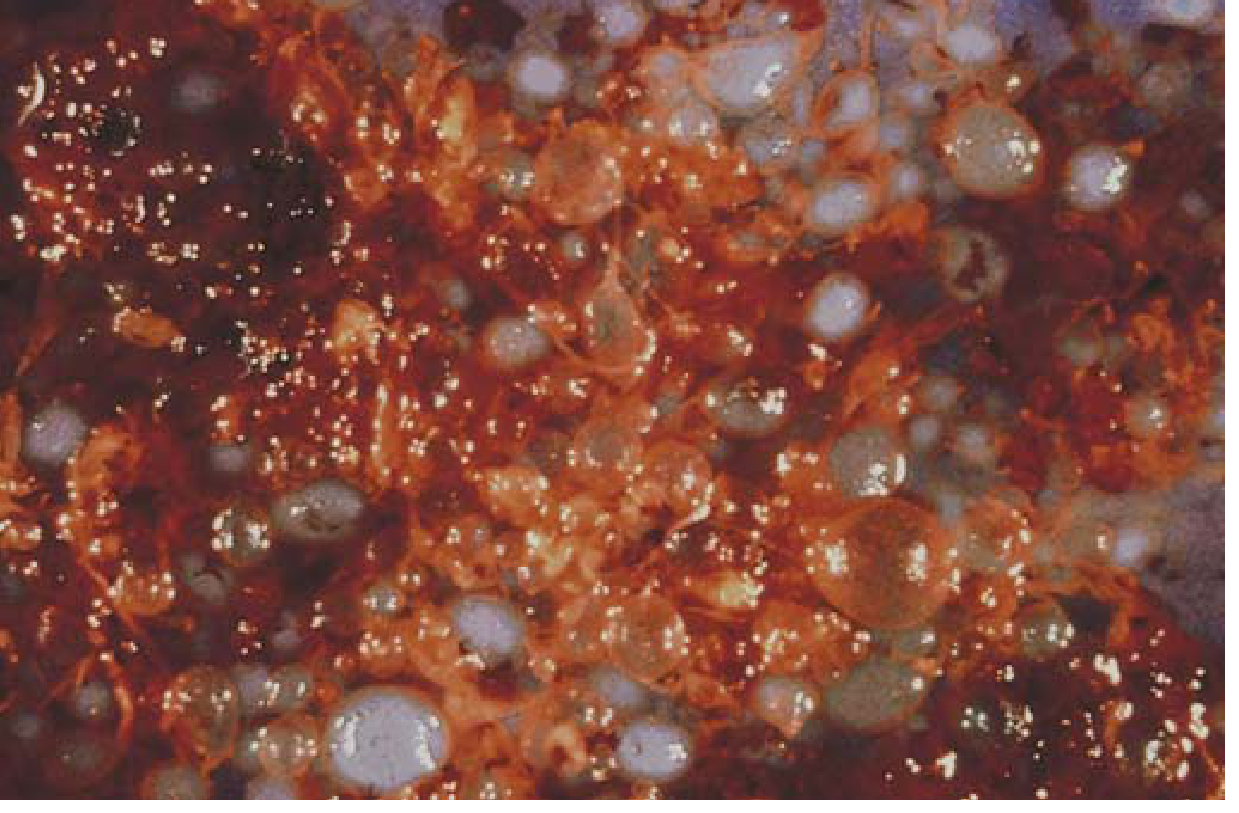
Clinical presentation:
- Vaginal bleeding (usually late 1st / early 2nd trimester)
- Uterus "large for dates"
- Markedly elevated hCG
- No fetal heart sounds
- "Snowstorm" appearance on USS (complete mole)
- May pass grape-like vesicles per vaginum
Malignant forms of GTD (also cause bleeding):
-
Invasive mole: locally aggressive, penetrates uterine wall, risk of life-threatening haemorrhage
-
Choriocarcinoma: highly invasive, frequently metastatic; highly responsive to chemotherapy
-
Placental site trophoblastic tumour (PSTT): produces HPL rather than hCG; treated surgically
-
Robbins & Kumar Basic Pathology, p. 703-704
6. Corpus Luteum Cyst Rupture
- The corpus luteum (formed from the ruptured follicle after ovulation) becomes cystic and can rupture or bleed
- Causes intraperitoneal haemorrhage + vaginal bleeding
- Can mimic ectopic pregnancy clinically
- Diagnosed by USS; managed conservatively in most cases
B. Non-Obstetric Causes
These arise from the genital tract rather than the pregnancy itself, but coincide with early pregnancy.
7. Cervical Lesions
- Cervical ectropion (erosion): Columnar epithelium everts onto the ectocervix; highly vascular in pregnancy due to increased oestrogen and blood flow; bleeds easily on contact (postcoital bleeding common)
- Cervical polyps: Benign pedunculated lesions; bleed easily, especially in pregnancy
- Cervicitis / STI: Chlamydia, gonorrhoea cause friable, inflamed cervix with contact bleeding
- Cervical carcinoma: Rare but must be excluded; typically presents with painless contact bleeding
8. Vaginal Lesions / Trauma
- Vaginal lacerations (most common mechanism: coitus)
- Foreign bodies
- Trauma (falls, interpersonal violence) - particularly dangerous in pregnancy due to fetal/placental risk
9. Lower Genital Tract Infection / Vaginitis
- Inflamed vaginal mucosa can bleed
- Associated with discharge, odour, dyspareunia
Summary Table
| Condition | Typical Gestation | Pain | Cervical Os | hCG | USS Finding |
|---|---|---|---|---|---|
| Implantation bleeding | ~4-5 weeks | None | Closed | Rising | Normal |
| Threatened miscarriage | Any (<20 wk) | ± Mild cramps | Closed | Normal/low | IUP ± cardiac activity |
| Inevitable/incomplete miscarriage | Any (<20 wk) | Cramps | Open | Falling | POC in os/cavity |
| Missed miscarriage | 6-12 weeks | None | Closed | Low/static | No cardiac activity |
| Ectopic pregnancy | 6-8 weeks | Unilateral pelvic pain | Closed | Low/plateau | No IUP; adnexal mass |
| Subchorionic haemorrhage | 1st/early 2nd trimester | None | Closed | Normal | Retroplacental clot |
| Molar pregnancy | 9-14 weeks | None | Closed | Very high | Snowstorm pattern |
| Corpus luteum cyst rupture | 6-12 weeks | Acute pelvic pain | Closed | Normal | Free fluid; cyst |
| Cervical/vaginal lesion | Any | None | Closed | Normal | Normal |
Sources: ROSEN's Emergency Medicine (9th ed.) | Robbins & Kumar Basic Pathology | Creasy & Resnik's Maternal-Fetal Medicine | Swanson's Family Medicine Review
This is a shared conversation. Sign in to Orris to start your own chat.