HLA B27
HLA B27 clinical significance spondyloarthropathy 2025
"HLA-B27" AND spondyloarthritis
HLA-B27
What It Is
Epidemiology
| Population | HLA-B27 prevalence |
|---|---|
| White Europeans | ~8-9% |
| Inuit / Indigenous circumpolar | up to 25-40% |
| African / Sub-Saharan | <1% |
| East Asians | ~4-8% |
Associated Diseases (HLA-B27 Syndromes)
| Disease | HLA-B27 positivity |
|---|---|
| Ankylosing spondylitis (r-axSpA) | 85-95% |
| Non-radiographic axial SpA | 50-90% |
| Reactive arthritis | ~50-80% |
| Psoriatic arthritis (with axial involvement) | ~50% |
| Uveitis (anterior, acute) | ~50-60% |
| IBD-associated arthropathy | <50% |
| Undifferentiated SpA | ~70% |
- HLA-B27 confers an odds ratio >50 for AS in White Europeans.
- Only a minority (~1-5%) of HLA-B27 carriers ever develop AS, so population screening is not indicated.
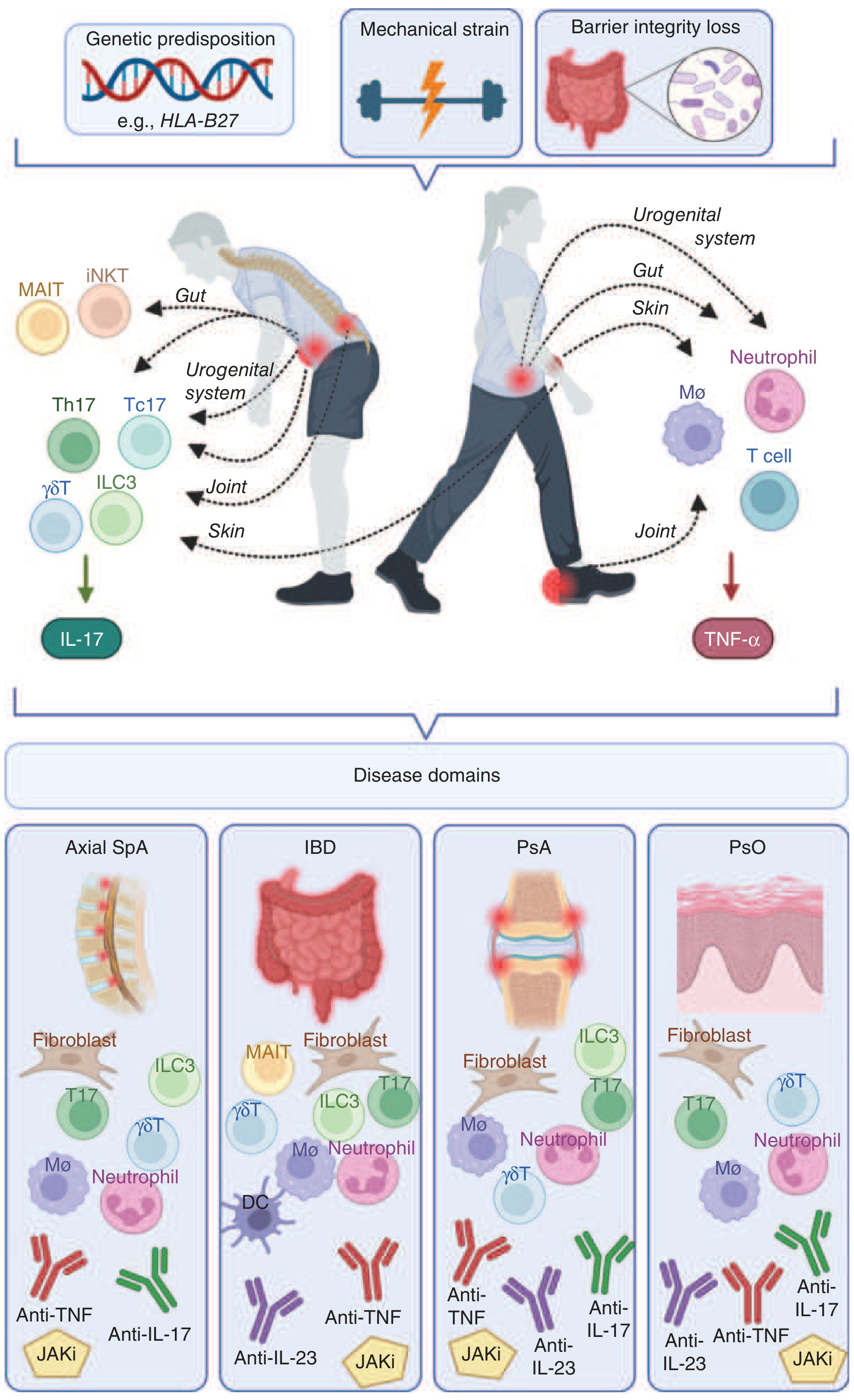
Pathogenic Mechanisms (Three Competing Theories)
1. Arthritogenic Peptide Theory (Classic)
- HLA-B27 presents specific microbial or self-peptides to CD8+ T cells
- Molecular mimicry between microbial antigens and self-peptides drives autoimmune joint inflammation
- Supported by: HLA-B27-restricted CD8+ T cells found in synovial fluid of AS patients
- Weakened by: disease in B27-transgenic rats is independent of CD8+ T cells
2. Unfolded Protein Response (UPR) / ER Stress Theory
- HLA-B27 assembles more slowly in the endoplasmic reticulum than any other HLA molecule
- Misfolded/slow-folding heavy chains accumulate, triggering ER stress
- ER stress activates NF-κB and promotes IL-23 secretion from macrophages
- IL-23 then drives the IL-23/IL-17 axis central to SpA pathogenesis
- Supported in B27-transgenic rats and AS synovium; less evidence in circulating cells
3. Heavy Chain Homodimer (Free Heavy Chain) Theory
- β2-microglobulin can dissociate from surface HLA-B27, leaving free heavy chains
- Free heavy chains dimerize to form B27 homodimers on the cell surface
- Recognized by KIR3DL2 on subsets of T cells and NK cells
- May activate innate and adaptive immune responses independent of classical peptide presentation
SpA Pathogenesis Diagram
Genetic Context: HLA-B27 Is Not the Whole Story
- IL23R - IL-23 receptor variants (most replicated non-MHC association; protective allele reduces IL-23 signaling)
- ERAP1 - aminopeptidase that trims peptides before loading onto HLA molecules; interacts epistatically with HLA-B27
- STAT3, JAK2, TYK2 - IL-23/IL-17 signaling pathway genes
- CARD9, IL12B, IL1R1/R2, IL6R, IL7R - innate immunity and cytokine signaling
- Other MHC alleles: HLA-B*51, HLA-B*40, HLA-B*13 also confer risk
Diagnostic Use
- Testing indication: Useful in patients with inflammatory back pain (morning stiffness >30 min, improves with exercise, nocturnal pain), uveitis, or peripheral arthritis suspected to be SpA
- Positive predictive value depends heavily on pre-test probability - in a low-risk general population, HLA-B27 positivity alone is not diagnostic
- A 2025 clinical practice analysis (J Rheumatol, 2025) found the most common testing indications were peripheral arthritis (33%), uveitis (22%), and back pain (17%); reactive arthritis had the highest positive test rate (~50%); ophthalmology had the highest overall HLA-B27 positivity rate (15.4%)
- HLA-B27 is commonly co-tested with ANA and RF, though this practice may not always be clinically appropriate
HLA-B27 and Uveitis
- HLA-B27 is the most common identifiable cause of acute anterior uveitis (AAU)
- Over half of HLA-B27-positive patients presenting with uveitis will have an underlying SpA diagnosis - The Wills Eye Manual
- Features: unilateral, recurrent, acute onset, intense flare in anterior chamber
Recent Evidence (2024-2026)
- A 2024 systematic review and meta-analysis (PMID 38305346) confirmed HLA-B27 as one of the strongest individual diagnostic features for SpA across clinical, lab, and imaging parameters.
- HLA-B27 predicts progression from subclinical inflammation to overt axial SpA in first-degree relatives of SpA patients (independent of baseline inflammation levels).
- HLA-B27 is being explored as a potential therapeutic target in axSpA, with research into gene silencing and allele-specific approaches (ScienceDirect, 2025).
There is any cure if the cure will come Which year
HLA-B27 cure gene therapy research 2025 2026
"HLA-B27" AND ("gene therapy" OR "gene silencing" OR cure)
PMID: 40674836
https://www.rheumagen.com/news-events/rheumagen-presents-hla…
Is There a Cure for HLA-B27-Associated Disease?
Current Reality (2026)
| Treatment type | Examples | What they do |
|---|---|---|
| NSAIDs | Naproxen, diclofenac | Reduce pain and stiffness |
| Anti-TNF biologics | Adalimumab, etanercept | Block TNF-driven inflammation |
| Anti-IL-17 biologics | Secukinumab, ixekizumab | Block IL-17 axis |
| JAK inhibitors | Tofacitinib, upadacitinib | Block intracellular cytokine signaling |
| Anti-IL-23 | Risankizumab | Newer option, especially for IBD overlap |
What Research Is Happening Toward a Cure?
1. Gene Editing (CRISPR/Cas9 and similar tools)
- The idea: edit the HLA-B27 gene itself in immune or stem cells so it no longer triggers disease
- RheumaGen Inc. (a US biotech) presented preclinical data at ACR Convergence 2025 showing that editing a single amino acid at position 82 of an HLA molecule blocks the binding of disease-causing peptides to T cells
- This "anchor-position editing" could potentially be a one-time therapy
- Currently: preclinical only (animal/cell models, not yet in humans)
2. RNA Interference (RNAi) / Gene Silencing
- Small interfering RNA (siRNA) molecules designed to silence HLA-B27 expression specifically in inflamed tissue
- Theoretical advantage: reversible, does not permanently alter the genome
- Currently: early experimental stage
3. Viral Vector Gene Delivery
- Using modified viruses to deliver corrective genetic material
- Still conceptual for HLA-B27 diseases specifically
When Might a Cure Come?
| Stage | Estimated timeline |
|---|---|
| Preclinical (animal/cell studies) | Now (2025-2026) |
| Phase 1 human safety trials | Possibly 2027-2030 |
| Phase 2/3 efficacy trials | 2030-2035 |
| Regulatory approval (if successful) | 2035 or later |
- HLA-B27 is expressed on ALL nucleated cells - editing it safely without off-target effects is very challenging
- Even if HLA-B27 is silenced, disease may already be established in joints and may not fully reverse
- Most people with HLA-B27 never get sick - so a "cure" really targets the minority who develop SpA
- Regulatory and safety hurdles for gene editing in non-fatal diseases are very high
Bottom Line
See a person, 18 years old, he have hla b 27 positive what is the common disease for this? He have symptoms, both knee pain, ankle pain, hip pain, no spine, involvement right now diagnose the situation and suggest long-term medicines because he’s 18 years old and which blood test he need to repeat every month.
"peripheral spondyloarthritis" AND management AND "HLA-B27"
spondyloarthritis young onset treatment guidelines biologics
peripheral spondyloarthritis 18 year old HLA-B27 treatment NSAID sulfasalazine monitoring blood tests 2025
ASAS EULAR guidelines peripheral spondyloarthritis treatment stepwise sulfasalazine TNF inhibitor monitoring 2024 2025
https://rheumnow.com/news/2026-guidelines-treatment-axial-sp…
Important disclaimer: This is educational information based on medical textbooks and guidelines. All treatment decisions for a real patient must be made by a qualified rheumatologist. An 18-year-old with active joint disease needs formal specialist care.
Clinical Assessment: 18-Year-Old, HLA-B27 Positive
Step 1: Diagnosis
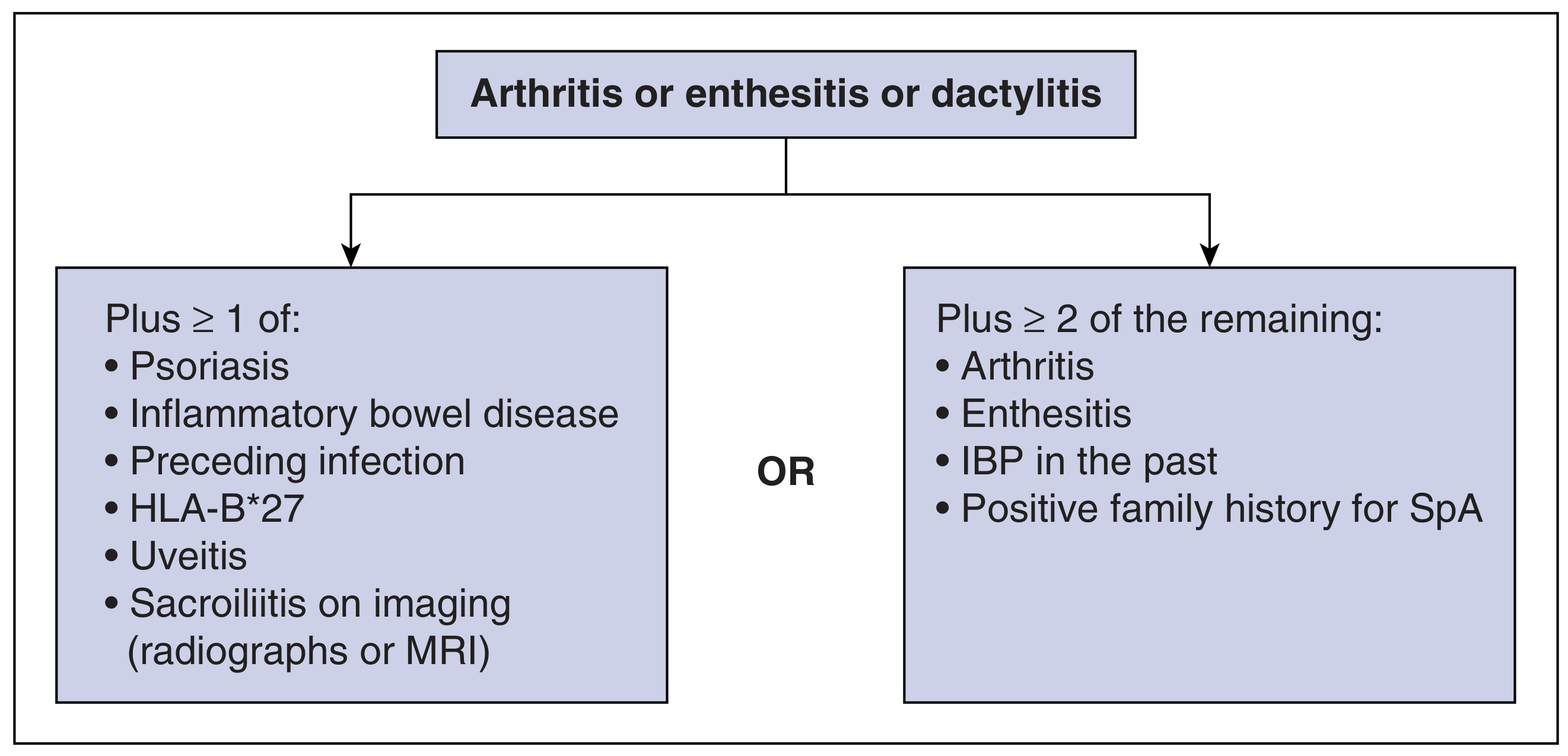
Most Likely: Peripheral Spondyloarthritis (pSpA)
Differential Diagnoses to Rule Out
| Diagnosis | Why it fits | How to differentiate |
|---|---|---|
| Peripheral SpA / undifferentiated SpA | Most likely - HLA-B27 +, lower limb arthritis, young age | MRI sacroiliac joints (may show early sacroiliitis not visible on X-ray) |
| Reactive arthritis (ReA) | HLA-B27 +, asymmetric lower limb arthritis, young male | Ask about preceding infection (throat, GI, urogenital 2-6 weeks prior) |
| Juvenile Spondyloarthritis | Age 18, HLA-B27 +, peripheral arthritis at presentation | Overlaps with pSpA; same workup |
| Early ankylosing spondylitis | Spinal involvement may come later; hips are commonly affected in early AS | MRI SI joints, look for morning stiffness >30 min |
| Enthesitis-related arthritis (ERA) | JIA subtype in HLA-B27 + young patients | Enthesitis at heel/patellar tendon insertion |
Key Clinical Questions to Ask This Patient
- Was there a preceding infection 2-6 weeks ago (throat infection, diarrhea, urinary symptoms)? - points to reactive arthritis
- Any eye redness/pain (uveitis)?
- Any skin rash or psoriasis in family?
- Any bowel symptoms (IBD)?
- Morning stiffness - how long? Does it improve with movement?
- Night pain that improves after getting up?
- Any heel pain (enthesitis at Achilles insertion)?
- Family history of AS, psoriasis, IBD?
Step 2: Investigations Needed Now (Baseline)
Imaging
| Test | Purpose |
|---|---|
| X-ray pelvis (SI joints) | Look for sacroiliitis (grade 1-4) |
| MRI sacroiliac joints | Detect early bone marrow edema before X-ray changes appear - preferred in young patients per 2026 guidelines |
| X-ray both knees, ankles, hips | Assess joint damage, rule out other pathology |
Blood Tests (Baseline Before Starting Treatment)
| Test | Purpose |
|---|---|
| CBC (Complete Blood Count) | Baseline; detect anemia of inflammation |
| ESR (Erythrocyte Sedimentation Rate) | Inflammation marker |
| CRP (C-Reactive Protein) | More sensitive acute inflammation marker |
| LFT (Liver Function Tests) | Baseline before NSAIDs/sulfasalazine |
| Renal function (creatinine, urea) | Baseline before NSAIDs |
| Urine routine examination | Baseline; NSAIDs affect kidneys |
| HLA-B27 | Already positive - confirmed |
| RF (Rheumatoid Factor) | Should be negative in SpA (seronegative) |
| Anti-CCP antibodies | Should be negative - rule out RA |
| ANA | Rule out SLE, especially at this age |
| Blood culture / stool culture / urine culture | If reactive arthritis suspected |
| Throat swab / ASOT | If recent infection history |
| Uric acid | Rule out gout (less likely at 18 but worth checking) |
Step 3: Long-Term Treatment Plan
Treatment Ladder (Per ASAS-EULAR 2022 + 2026 Guidelines)
STEP 1: NSAIDs (First Line - Start Here)
↓ [If inadequate response after 2-4 weeks per NSAID × 2 trials]
STEP 2: Sulfasalazine (for peripheral arthritis specifically)
↓ [If inadequate response after 3 months]
STEP 3: Biologic DMARD (TNF inhibitor or IL-17 inhibitor)
STEP 1 - NSAIDs (Start Immediately)
Per 2026 guidelines: NSAIDs are first-line therapy for all SpA patients
| Drug | Dose | Notes |
|---|---|---|
| Naproxen | 500 mg twice daily | Preferred NSAID in young patients - better GI profile |
| Diclofenac | 75 mg twice daily | Alternative; good anti-inflammatory |
| Indomethacin | 25-50 mg three times daily | More potent but more GI side effects |
STEP 2 - Sulfasalazine (For Peripheral Joint Disease)
Per ASAS-EULAR: "Sulfasalazine may be considered in patients with peripheral arthritis" - this patient has peripheral arthritis, so sulfasalazine is appropriate if NSAIDs alone are insufficient.
| Drug | Dose | Titration |
|---|---|---|
| Sulfasalazine | Start: 500 mg/day | Increase by 500 mg/week up to 2000-3000 mg/day in divided doses |
- Takes 6-12 weeks to show full effect
- Safe in young adults; widely used in JIA/ERA/SpA
STEP 3 - Biologics (If Steps 1-2 Fail)
Per 2026 guidelines: TNF inhibitors and IL-17 inhibitors are equally recommended as initial biologic DMARDs
| Drug Class | Examples | Notes |
|---|---|---|
| Anti-TNF | Adalimumab (Humira), Etanercept, Golimumab | Approved for peripheral SpA; very effective |
| Anti-IL-17 | Secukinumab (Cosentyx), Ixekizumab | Especially good if psoriasis present |
| JAK inhibitors | Tofacitinib, Upadacitinib | Second-line biologics per 2026 guidelines |
Note for 18-year-old: All these biologics have been studied and used in adolescents. Etanercept and adalimumab have the most pediatric/young adult data. However, screening for TB, hepatitis B, varicella is mandatory before starting any biologic.
Non-Pharmacological (Equally Important)
- Physiotherapy: Daily stretching exercises, especially hip flexors, quadriceps
- Swimming / hydrotherapy: Low-impact, excellent for SpA
- Avoid prolonged sitting: Get up and move every 30-60 minutes
- No smoking: Smoking worsens SpA outcomes significantly
- Weight control: Reduces joint load
Step 4: Monthly Blood Test Monitoring
If on NSAIDs Only
| Test | Frequency | Why |
|---|---|---|
| CBC | Every 3 months | Detect GI blood loss (chronic NSAID use can cause occult GI bleeding) |
| Renal function (creatinine, urea) | Every 3 months | NSAIDs reduce renal blood flow long-term |
| LFT | Every 3 months | NSAID-related hepatotoxicity (rare but possible) |
| ESR + CRP | Monthly initially, then every 3 months | Track disease activity/inflammation |
If on Sulfasalazine (Monthly Monitoring Required)
| Test | Frequency | Why |
|---|---|---|
| CBC with differential | Every month for 3 months, then every 3 months | Sulfasalazine can cause leukopenia, thrombocytopenia, megaloblastic anemia |
| LFT (ALT, AST, bilirubin) | Every month for 3 months, then every 3 months | Hepatotoxicity risk |
| Renal function | Every 3 months | Sulfasalazine can rarely affect kidneys |
| ESR + CRP | Monthly initially | Track response |
| Urine routine | Monthly | Crystalluria with sulfasalazine |
If on Biologics (Anti-TNF / Anti-IL-17)
| Test | Frequency | Why |
|---|---|---|
| CBC | Every 3 months | Biologics can cause cytopenia |
| LFT | Every 3 months | Hepatotoxicity especially with anti-TNF |
| ESR + CRP | Every 3 months | Disease activity monitoring |
| TB screening (IGRA/Mantoux) | Annually | Anti-TNF reactivates latent TB |
| Hepatitis B serology | Before starting, then as needed | Reactivation risk |
| Lipid profile | Every 6 months (especially JAKi) | JAK inhibitors raise LDL |
Summary Card for This Patient
| Diagnosis | Peripheral SpA (most likely) - confirm with MRI SI joints |
| Start now | Naproxen 500 mg twice daily + Omeprazole 20 mg once daily |
| Add if NSAIDs fail | Sulfasalazine 2000-3000 mg/day (titrate up over 4-6 weeks) |
| Escalate to biologic if | Still active after 3-6 months on sulfasalazine + NSAIDs |
| Monthly blood tests | CBC, LFT, renal function, ESR, CRP, urine routine (monthly for first 3 months on sulfasalazine, then every 3 months) |
| Watch for | Uveitis, back pain onset (may develop axial involvement over years) |
| Urgent referral to | Rheumatologist - this patient needs specialist-supervised care |
The spine is not involved now, but ~30-40% of peripheral SpA patients develop axial involvement over time. Annual monitoring with clinical assessment and MRI if new back symptoms appear is recommended. - Harrison's Principles of Internal Medicine 22E; Rheumatology 2-Volume Set (Elsevier 2022); 2026 ACR/EULAR SpA Guidelines