Obesity reference medicine textbook
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Now I have a complete picture of the library. Here is a full reference guide to the medical textbook library, organized by specialty, with obesity coverage noted where relevant.
Medical Textbook Library - Complete Reference
The library contains ~130+ medical textbooks spanning virtually every clinical specialty. Below is the full catalog organized by specialty.
Anatomy
| Title | ISBN |
|---|---|
| Color Atlas of Ultrasound Anatomy, 3e | 9783132422049 |
| Color Atlas of Human Anatomy Vol 2 - Internal Organs | 9783132424487 |
| Color Atlas of Human Anatomy Vol 1 | 9783132424432 |
| Color Atlas of Human Anatomy Vol 3 | 9783132424517 |
| General Anatomy and Musculoskeletal System (THIEME Atlas) | 9781626237186 |
| Gray's Anatomy for Students | 9780323934237 |
| Imaging Anatomy - Bones, Joints, Vessels and Nerves | 9781626239845 |
| Netter's Atlas of Human Anatomy | 9780323547048 |
Anesthesiology
| Title | ISBN |
|---|---|
| Barash, Cullen & Stoelting's Clinical Anesthesia, 9e | 9781975199074 |
| Miller's Anesthesia, 2-Volume Set, 10e | 9780323935920 |
| Morgan and Mikhail's Clinical Anesthesiology, 7e | 9781260473797 |
Biochemistry
| Title | ISBN |
|---|---|
| Basic Medical Biochemistry - A Clinical Approach, 6e | 9781975150143 |
| Biochemistry, 8th ed - Lippincott Illustrated Reviews | 9781975155063 |
| Harper's Illustrated Biochemistry, 32nd Ed | 9781260469943 |
Cardiology
| Title | ISBN |
|---|---|
| Braunwald's Heart Disease, 2 Vol Set | 9780323722193 |
| Fuster and Hurst's The Heart, 15th Edition | 9781264257560 |
| Textbook of Clinical Echocardiography | 9780323882088 |
Community Medicine / Preventive Medicine
| Title | ISBN |
|---|---|
| Park's Textbook of Preventive and Social Medicine | 9789382219163 |
Dermatology
| Title | ISBN |
|---|---|
| Andrews' Diseases of the Skin Clinical Atlas, 2e | 9780323790130 |
| Andrews' Diseases of the Skin - Clinical Dermatology | 9780323547536 |
| Dermatology, 2-Volume Set 5e | 9780702082252 |
| Fitzpatrick's Dermatology, Vol 1 & 2 | 9780071837781 |
Emergency Medicine
| Title | ISBN |
|---|---|
| ROSEN's Emergency Medicine - Concepts and Clinical Practice | 9780323757898 |
| Roberts and Hedges' Clinical Procedures in Emergency | 9780323354783 |
| Tintinalli's Emergency Medicine - A Comprehensive Study | 9781260019933 |
ENT / Otolaryngology
| Title | ISBN |
|---|---|
| Cummings Otolaryngology Head and Neck Surgery | 9780323612173 |
| K.J. Lee's Essential Otolaryngology | 9781260122237 |
| Scott-Brown's Otorhinolaryngology Head & Neck Surgery (3 vols) | 9781138094642 / 9781138094611 / 9781138094634 |
| Shambaugh Surgery of the Ear | 9781607950264 |
Embryology
| Title | ISBN |
|---|---|
| Langman's Medical Embryology | 9781496383907 |
| The Developing Human - Clinically Oriented Embryology | 9780323611541 |
Family Medicine
| Title | ISBN |
|---|---|
| Pfenninger and Fowler's Procedures for Primary Care, 3e | 9780323052672 |
| Swanson's Family Medicine Review | 9780323698115 |
| Textbook of Family Medicine, 9e | 9780323239905 |
Forensic Medicine
| Title | ISBN |
|---|---|
| Brogdon's Forensic Radiology | 9781420075632 |
| DiMaio's Forensic Pathology, 3rd Edition | 9780429318764 |
| Forensic Anthropology - A Comprehensive Introduction, 2e | 9781498736121 |
| P.C. Dikshit Textbook of Forensic Medicine and Toxicology | 9788188867967 |
| Parikh's Textbook of Medical Jurisprudence, Forensic Medicine and Toxicology | 9789388902267 |
| The Essentials of Forensic Medicine and Toxicology, 36th ed (2026) | 9789366165257 |
Gastroenterology / GI Surgery
| Title | ISBN |
|---|---|
| Clinical Gastrointestinal Endoscopy, Expert Consult 3e | 9780323415095 |
| Sleisenger and Fordtran's Gastrointestinal and Liver Disease | 9780323609623 |
| Yamada's Textbook of Gastroenterology, 3 Volume Set, 7e | 9781119600169 |
| Maingot's Abdominal Operations | 9780071639873 |
General Surgery
| Title | ISBN |
|---|---|
| 22nd Edition Pye's Surgical Handicraft | 0750613637 |
| Bailey and Love's Short Practice of Surgery, 28e | 9780367548117 |
| Current Surgical Therapy, 14e | 9780323796835 |
| Fischer's Mastery of Surgery, 8e | 9781975176433 |
| Mulholland and Greenfield's Surgery - Scientific Principles & Practice, 7e | 9781975143169 |
| S Das A Manual on Clinical Surgery, 13e | 9788190568104 |
| Schwartz's Principles of Surgery, 2-Volume Set, 11e | 9781259835346 |
| Sabiston Textbook of Surgery - Biological Basis of Modern Surgical Practice | 9780443124341 |
Genetics
| Title | ISBN |
|---|---|
| Emery's Elements of Medical Genetics and Genomics | 9780323702782* |
| Thompson & Thompson Genetics and Genomics in Medicine, 9e | 9780323547628 |
Histology
| Title | ISBN |
|---|---|
| Histology - A Text and Atlas With Correlated Cell and Molecular Biology | 9781975181512 |
| Junqueira's Basic Histology - Text and Atlas, 17e | 9781264930395 |
Immunology
| Title | ISBN |
|---|---|
| Cellular and Molecular Immunology | 9780323757485 |
| Janeway's Immunobiology, 10e | 9780393884876 |
| Roitt's Essential Immunology | 9781118415771 |
Internal Medicine
| Title | ISBN |
|---|---|
| Firestein & Kelley's Textbook of Rheumatology, 2-Volume Set | 9780323935364 |
| Frameworks for Internal Medicine | 9781496359308 |
| Goldman-Cecil Medicine, International Edition, 2 Volume Set | 9780323930345 |
| Harrison's Principles of Internal Medicine, 22nd Ed (2025) | 9781265977061 |
| Rheumatology, 2-Volume Set (2022, Elsevier) | 9780702081330 |
| Symptom to Diagnosis - An Evidence Based Guide, 4e | 9781260121117 |
| The Washington Manual of Medical Therapeutics | 9781975190620 |
Laboratory Medicine / Pathology
| Title | ISBN |
|---|---|
| Henry's Clinical Diagnosis and Management by Laboratory Methods | 9780323673204 |
| Quick Compendium of Clinical Pathology, 5e | 9780891896852 |
| Tietz Textbook of Laboratory Medicine, 7e | 9780323775724 |
Microbiology
| Title | ISBN |
|---|---|
| Jawetz, Melnick & Adelberg's Medical Microbiology, 28e | 9781260012026 |
| Medical Microbiology, 9e | 9780323673228 |
| Sherris & Ryan's Medical Microbiology, 8e | 9781260464283 |
Nephrology
| Title | ISBN |
|---|---|
| Brenner and Rector's The Kidney, 2-Volume Set | 9780323532655 |
| Comprehensive Clinical Nephrology, 7e | 9780323825924 |
| National Kidney Foundation Primer on Kidney Diseases, 8e | 9780323791229 |
Neurology
| Title | ISBN |
|---|---|
| Adams and Victor's Principles of Neurology, 12e | 9781264264520 |
| Bradley and Daroff's Neurology in Clinical Practice | 9780323642613 |
| Localization in Clinical Neurology, 8e | 9781975160241 |
| Plum and Posner's Diagnosis and Treatment of Stupor and Coma | 9780190208875 |
Neuroscience
| Title | ISBN |
|---|---|
| Eric Kandel - Principles of Neural Science, 6th Edition | 9781259642241 |
| Neuroanatomy Through Clinical Cases, 3e | 9781605359625 |
| Neuroscience - Exploring the Brain, 5e | 9781284286878 |
Obstetrics & Gynecology
| Title | ISBN |
|---|---|
| Berek & Novak's Gynecology | 9781496380357 |
| Creasy & Resnik's Maternal-Fetal Medicine - Principles and Practice | 9780323828499 |
Ophthalmology
| Title | ISBN |
|---|---|
| Kanski's Clinical Ophthalmology - A Systematic Approach, 10e | 9780443110993 |
| The Wills Eye Manual, 8e | 9781975160753 |
Orthopedics
| Title | ISBN |
|---|---|
| Campbell's Operative Orthopaedics, 15th Ed 2026 | 9780443117633 |
| Miller's Review of Orthopaedics, 9th Edition | 9780443112140 |
| Rockwood and Green's Fractures in Adults, 10th Ed 2025 | 9781975211608 |
Pathology
| Title | ISBN |
|---|---|
| Robbins & Kumar Basic Pathology | 9780323790185 |
| Robbins, Cotran & Kumar Pathologic Basis of Disease | 9780443264528 |
Pediatrics
| Title | ISBN |
|---|---|
| Red Book 2021 - Report of the Committee on Infectious Diseases | 9781610025218 |
| The Harriet Lane Handbook - Johns Hopkins Hospital, 23e | 9780323876988 |
Pharmacology
| Title | ISBN |
|---|---|
| Goodman & Gilman's The Pharmacological Basis of Therapeutics | 9781264258079 |
| Katzung's Basic and Clinical Pharmacology, 16e | 9781260463309 |
| Lippincott Illustrated Reviews: Pharmacology | 9781975170561 |
Physiology
| Title | ISBN |
|---|---|
| Costanzo Physiology, 7th Edition | 9780323793339 |
| Ganong's Review of Medical Physiology, 26th Edition | 9781260122404 |
| Guyton and Hall Textbook of Medical Physiology | 9780443111013 |
| Medical Physiology (Boron & Boulpaep) | 9780323319737 |
Psychiatry
| Title | ISBN |
|---|---|
| Kaplan & Sadock's Comprehensive Textbook of Psychiatry | 9781975145569* |
| Kaplan and Sadock's Synopsis of Psychiatry | 9781975145569 |
| Stahl's Essential Psychopharmacology - Neuroscientific Basis | 9781108838573 |
| The Clozapine Handbook | 9781108447461 |
| The Maudsley Deprescribing Guidelines | 9781119823025 |
| The Maudsley Prescribing Guidelines in Psychiatry, 15e | 9781394238767 |
Pulmonology / Respiratory Medicine
| Title | ISBN |
|---|---|
| Fishman's Pulmonary Diseases and Disorders, 2-Volume Set | 9781260473940 |
| Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume | 9780323655873 |
Radiology
| Title | ISBN |
|---|---|
| Grainger & Allison's Diagnostic Radiology | 9780323760751 |
Urology
| Title | ISBN |
|---|---|
| Campbell Walsh Wein Urology, 3-Volume Set | 9780323546423 |
| Hinman's Atlas of Urologic Surgery | 9780128016480 |
| Smith and Tanagho's General Urology, 19e | 9781259834332 |
Obesity Coverage in the Library
Based on dedicated "Obesity" section headings found across the library, the following books contain substantial obesity-specific content:
| Book | Specialty | Notes |
|---|---|---|
| Sleisenger and Fordtran's GI and Liver Disease | Gastroenterology | Major dedicated obesity chapter (block 1, ~6 subsections) |
| Cummings Otolaryngology | ENT | Obesity section (sleep apnea, upper airway context) |
| Murray & Nadel's Respiratory Medicine | Pulmonology | Obesity-related lung disease sections |
| Brenner and Rector's The Kidney | Nephrology | Obesity & kidney disease (3 dedicated sections) |
| Textbook of Family Medicine 9e | Family Medicine | Obesity management in primary care |
| Campbell Walsh Wein Urology | Urology | Obesity effects on urologic conditions |
| Fitzpatrick's Dermatology | Dermatology | Obesity-related skin conditions |
| Harrison's Internal Medicine 22e (2025) | Internal Medicine | Comprehensive coverage expected |
| Goldman-Cecil Medicine | Internal Medicine | Comprehensive coverage |
| Fishman's Pulmonary Diseases | Pulmonology | Obesity-hypoventilation/respiratory |
| Braunwald's Heart Disease | Cardiology | Obesity & cardiovascular disease |
| Bailey and Love's Surgery / Schwartz's Surgery | General Surgery | Bariatric surgery sections |
The library does not contain a standalone "Obesity Medicine" textbook (such as a dedicated obesity medicine reference like Handbook of Obesity by Bray & Bouchard, or Practical Manual of Clinical Obesity). However, obesity is covered as a major topic across at least a dozen of the reference works above - most comprehensively in Harrison's, Goldman-Cecil, Sleisenger & Fordtran's, and the respiratory medicine texts.
If you want me to pull the full obesity chapter from any specific book, just let me know which one interests you (e.g., Harrison's 22e, Sleisenger & Fordtran's, or another title).
Provide everything about obesity
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Reading File
Obesity - Comprehensive Medical Reference
Primary sources: Harrison's Principles of Internal Medicine 22E (2025), Goldman-Cecil Medicine, Sleisenger & Fordtran's GI and Liver Disease
1. DEFINITION AND CLASSIFICATION
Obesity is defined as a state of excess adipose tissue mass that adversely affects health. Because direct measurement of fat mass is impractical in routine clinical settings, the body mass index (BMI) - calculated as weight (kg) / height (m²) - is used as a proxy measure.
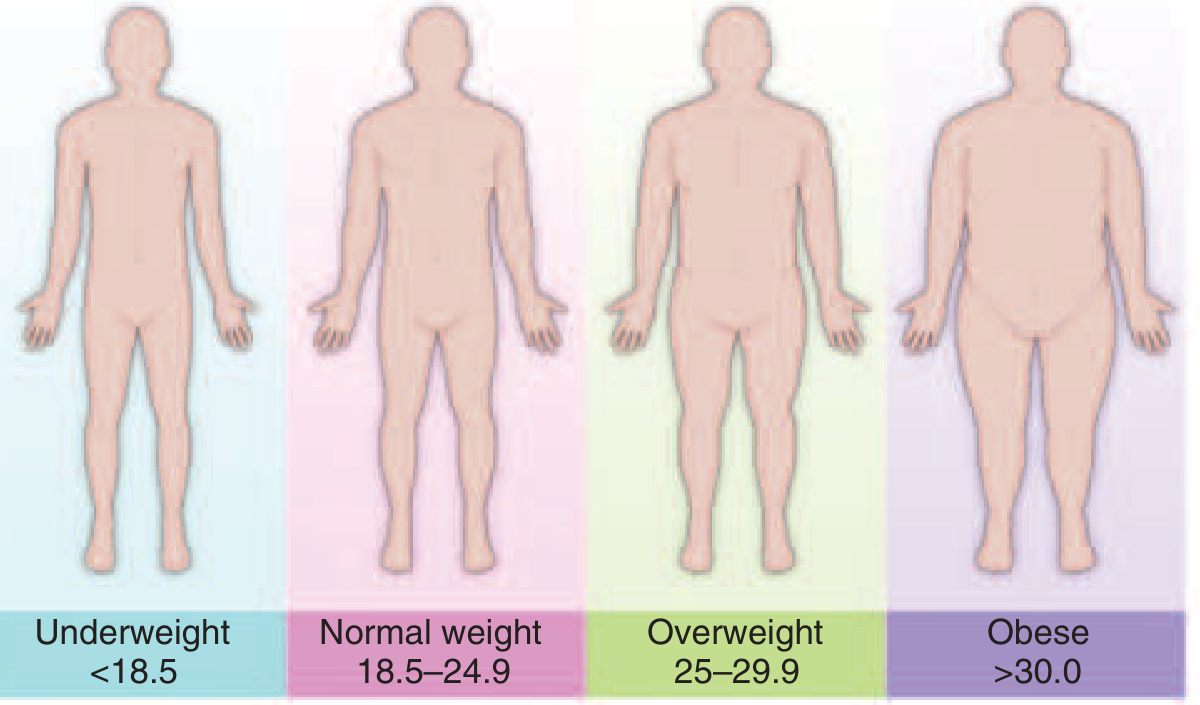
FIGURE 413-1 (Harrison's 22e) - WHO BMI-based classification of weight status
BMI Classification Table (WHO)
| Classification | BMI (kg/m²) | Obesity Class | Disease Risk |
|---|---|---|---|
| Underweight | <18.5 | - | - |
| Healthy weight | 18.5-24.9 | - | - |
| Overweight | 25.0-29.9 | - | Increased |
| Obesity | 30.0-34.9 | I | High |
| Obesity | 35.0-39.9 | II | Very high |
| Extreme obesity | ≥40 | III | Extremely high |
Important caveats:
- For very muscular individuals, BMI may overestimate body fat
- For any given BMI, women have a higher percentage of body fat than men
- Asian populations have worse health outcomes at lower BMI thresholds - lower cutoffs are proposed for the Asia-Pacific region
- BMI-based definitions were established largely in predominantly white, Western populations
Fat Distribution: Waist-to-Hip Ratio
Independent of the degree of obesity, a waist-to-hip ratio >0.9 in women and >1.0 in men is associated with adverse outcomes (type 2 diabetes, dyslipidemia). Females store more fat subcutaneously (buttocks, thighs, upper arms); men are more prone to intraabdominal and truncal subcutaneous fat deposition.
2. EPIDEMIOLOGY
- United States (2017-2018): 42.4% of U.S. adults aged ≥20 had obesity - nearly a 3-fold increase since 1976-1980 (when prevalence was 14.5%)
- Racial disparities (US): Non-Hispanic Black people 49.6% > Hispanic 44.8% > non-Hispanic White 42.2% > non-Hispanic Asian 17.4%
- Sex: Prevalence slightly higher in women overall; Black women have the highest prevalence at 56.9%
- Global (WHO, 2016): >1.9 billion adults overweight; >650 million obese; 39% of adults overweight, 13% obese. Obesity has nearly tripled worldwide since 1975
- Children: In 2016, 340 million children and adolescents aged 5-19 were overweight or obese. 38 million children under age 5 were overweight or obese in 2019
- Most of the world's population now lives in countries where overweight and obesity kills more people than underweight
3. PATHOBIOLOGY AND ETIOLOGY
3.1 Energy Balance
Obesity develops when energy intake chronically exceeds energy expenditure. Even a surplus as small as 7 kcal/day is sufficient to produce obesity over years. Adipose tissue evolved as a solution to the intermittent availability of food - excess calories are converted to triglycerides stored in unilocular lipid droplets of fat cells.
3.2 Genetic Factors
Genetic factors play a major role in predisposing individuals to a range of adiposity. Evidence from twin studies is compelling - identical twins raised apart have similar adiposity to each other but not to their adoptive siblings. Key genetic insights include:
- Leptin/leptin receptor (LEP/LEPR) mutations: Rare, cause severe early-onset obesity with hyperphagia; leptin-deficient patients respond dramatically to leptin replacement
- MC4R (melanocortin 4 receptor) mutations: ~5% of patients with severe, early-onset obesity have heterozygous loss-of-function MC4R mutations; features include hyperphagia, hyperinsulinemia, and increased linear growth
- POMC (proopiomelanocortin) mutations: Homozygous/compound heterozygous mutations cause hyperphagia, early-onset obesity, isolated ACTH deficiency, and hypopigmentation
- Prohormone convertase 1 (PC1) deficiency: Severe early-onset obesity and ACTH deficiency due to impaired POMC processing
- Common variants (GWAS): The genetic predisposition to obesity is largely mediated through the brain's control of food intake - individuals carrying obesity-predisposing genetic variants tend to eat more and be less readily satiated
3.3 Why Doesn't Leptin Prevent Obesity?
Leptin, produced by adipose tissue, signals satiety to the hypothalamus. In common obesity, leptin levels are actually high (proportional to fat mass), but central leptin resistance develops. Thus common obesity is a state of leptin excess with resistance, not deficiency.
3.4 Environmental Factors (Obesogenic Environment)
The marked increase in obesity prevalence over recent decades cannot be explained by genetics alone. Environmental contributors include:
| Dietary Factors | Activity Factors |
|---|---|
| ↑ Energy density of foods | ↑ Sedentary behavior |
| ↑ Portion size | ↓ Activities of daily living |
| ↑ Variety (sweets, snacks, entrees) | ↓ Employment-related physical activity |
| ↑ Palatability | |
| ↑ Availability | |
| ↓ Cost | |
| ↑ Sugar-sweetened beverages |
Adults tend to respond to food volume rather than energy content, which is why energy-dense, high-fat foods promote weight gain. Sugar-sweetened beverages do not trigger compensatory reductions in food intake.
3.5 Constitutional and Epigenetic Influences
- Undernutrition in first two trimesters of pregnancy → increased probability of adult obesity in offspring
- Undernutrition in last trimester / early postnatal period → decreased risk of adult obesity, but increased risk of hypertension, abnormal glucose tolerance, and cardiovascular disease
- Infants of diabetic mothers tend to be fatter; their children have greater obesity prevalence aged 5-19
- Intrauterine exposure to diabetic environment → increased risk of diabetes and obesity in offspring
3.6 Secondary Causes of Obesity
Although most obesity is driven by biopsychosocial and behavioral factors, secondary causes should be considered:
- Polycystic ovarian syndrome (PCOS)
- Hypothyroidism
- Cushing's syndrome
- Hypothalamic disease
Drug-induced weight gain is common. Culprit medications include:
- Diabetes medications: insulin, sulfonylureas, thiazolidinediones
- Steroid hormones
- Antipsychotics: clozapine, olanzapine, risperidone
- Mood stabilizers: lithium
- Antidepressants: TCAs, MAOIs, paroxetine, mirtazapine
- Antiepileptics: valproate, gabapentin, carbamazepine
(Note: NSAIDs and calcium channel blockers may cause peripheral edema but do NOT increase body fat)
4. PHYSIOLOGIC REGULATION OF ENERGY BALANCE
Central Regulation
The hypothalamus is the primary center for integrating energy balance signals. Key circuits:
- Arcuate nucleus (ARC): Contains two opposing populations - AgRP/NPY neurons (appetite-stimulating) and POMC/CART neurons (appetite-suppressing)
- Leptin (from adipocytes): acts on ARC to suppress AgRP/NPY and stimulate POMC/CART → decreases appetite
- Insulin (from pancreas): also acts centrally to suppress food intake
- Ghrelin (from stomach): rises before meals, stimulates appetite; falls postprandially
- GLP-1, PYY, CCK (gut hormones): released postprandially, signal satiety
Peripheral Regulation
- Resting energy expenditure increases (not decreases) with obesity
- When obese patients lose weight by dieting, they tend to be more "energy efficient" than persons who were never obese - particularly in how many calories they burn during defined activity bouts
5. ADVERSE CONSEQUENCES OF OBESITY
5.1 Metabolic Complications
Type 2 Diabetes Mellitus
- Obesity is the single most important modifiable risk factor for T2DM
- Visceral adiposity drives insulin resistance through multiple mechanisms: elevated free fatty acids, adipokine dysregulation (↑ TNF-α, IL-6, resistin; ↓ adiponectin), ectopic fat deposition in liver and muscle
- ADA recommends screening individuals at an earlier age if they are overweight with one additional risk factor
Dyslipidemia
- Upper body/visceral obesity is associated with: ↑ triglycerides, ↓ HDL cholesterol, ↑ proportion of small dense LDL particles
- Mechanism: increased hepatic VLDL secretion driven by increased delivery of free fatty acids from visceral fat; reduced HDL and increased small dense LDL are indirect consequences of elevated triglyceride-rich VLDL
- Genetic polymorphisms in apolipoprotein E, lipoprotein lipase, apo B-100, and apo A-II modulate expression of these lipid abnormalities
Metabolic Syndrome
- Cluster of: central obesity + hypertriglyceridemia + low HDL + hypertension + elevated fasting glucose
5.2 Cardiovascular Complications
- Obesity is an independent risk factor for coronary artery disease, heart failure, and stroke
- Hypertension: obesity increases plasma volume and cardiac output, activates the renin-angiotensin-aldosterone system, and increases sympathetic nervous system activity
- Obesity cardiomyopathy: eccentric left ventricular hypertrophy from increased cardiac output demands
- Obstructive sleep apnea (see below) - a major driver of cardiovascular risk in obesity
5.3 Pulmonary Complications
Obesity Hypoventilation Syndrome (Pickwickian Syndrome)
- Defined as BMI ≥30 + chronic daytime hypercapnia (PaCO₂ >45 mmHg) in the absence of other causes
- Mechanism: reduced respiratory system compliance, decreased functional residual capacity, increased work of breathing
- Treatment: weight loss, positive airway pressure (CPAP or BiPAP), supplemental oxygen
Obstructive Sleep Apnea (OSA)
- Caused by enlargement of upper airway soft tissue → collapse of upper airways during inspiration during sleep
- More prevalent in men and women with upper body/visceral obesity
- Obstruction leads to: apneas, hypoxemia, hypercarbia, elevated catecholamines and endothelins
- Frequent arousals → poor sleep quality
- Associated with increased risk of hypertension; severe OSA can lead to right-sided heart failure and sudden death
- Goldman-Cecil notes: pulmonary function testing in obese patients shows reduced lung volumes (restrictive pattern)
5.4 Gastrointestinal Complications
- NAFLD/NASH (now MASLD/MASH): Strongly associated with obesity and metabolic syndrome; can progress to cirrhosis
- Gastroesophageal reflux disease (GERD): Increased intraabdominal pressure drives reflux
- Gallstones: Obesity promotes cholelithiasis through supersaturation of bile with cholesterol
- Colorectal polyps and cancer: Insulin resistance and hyperinsulinemia promote colonic epithelial proliferation
5.5 Endocrine Complications
- PCOS: Insulin resistance associated with obesity may trigger development of PCOS in susceptible women; characterized by hirsutism, irregular menses, anovulation
- Male hypogonadism: Obese men may suffer mild to severe hypothalamic hypogonadism (improving with weight loss)
- Elevated conversion of androgens to estrogens in adipose tissue
5.6 Musculoskeletal and Other Systemic Complications
- Osteoarthritis: Excess body weight increases prevalence of lower extremity degenerative joint disease
- Venous stasis: Occasionally aggravated by right-sided heart failure in severely obese patients
- Pseudotumor cerebri (idiopathic intracranial hypertension): Associated with obesity, especially in young women
- Gout: Hyperuricemia driven by insulin resistance and renal urate retention
5.7 Cancer Risk
Obesity is associated with an increased risk of at least 13 cancers:
- Breast, esophageal, liver, gallbladder, stomach, pancreatic, colorectal, ovarian, uterine/endometrial, renal cell, thyroid, meningioma, and multiple myeloma
- Likely mechanisms: higher insulin-like growth factor (IGF-1) levels, elevated estrogens from peripheral aromatization, chronic inflammation
5.8 Psychosocial Consequences
- Serious social, economic, and medical discrimination
- Depression and anxiety
- Impaired quality of life
- People with obesity may become socially and economically disadvantaged
6. EVALUATION AND DIAGNOSIS
Clinical Assessment
Three key anthropometric measurements:
- Weight
- Height (to calculate BMI)
- Waist circumference
Waist circumference thresholds for metabolic risk:
- Men: >102 cm (>40 in) - high risk
- Women: >88 cm (>35 in) - high risk
History
Key questions in the clinical evaluation:
- Age of onset and course of weight gain
- Dietary habits and physical activity patterns
- Review of medications (secondary causes)
- Sleep history (regularity, duration, efficiency, satisfaction)
- Psychosocial stressors - sleep deprivation is associated with metabolic alterations in appetite regulation, sympathetic overactivity, reduced insulin sensitivity, and circadian rhythm changes
- Stress contributes to obesity in part via adrenal cortical axis activation and elevated cortisol
- Family history (genetic predisposition)
- Patient's motivation for weight management
Physical Examination
- Blood pressure
- Signs of secondary causes (e.g., cushingoid features, thyroid abnormalities)
- Acanthosis nigricans (insulin resistance marker)
- Signs of complications (edema, hepatomegaly)
Laboratory Evaluation
- Fasting glucose and HbA1c
- Fasting lipid panel
- Liver function tests / hepatic imaging for NAFLD
- TSH (exclude hypothyroidism)
- If Cushing's suspected: overnight dexamethasone suppression test or 24-hr urinary free cortisol
7. TREATMENT
Treatment of obesity is multifactorial and should be individualized. Goals are:
- Sustained weight reduction
- Improvement or prevention of comorbidities
- Improved quality of life
A 5-10% reduction in body weight produces clinically significant improvements in most comorbidities.
7.1 Lifestyle Modification (Foundation of All Treatment)
Diet:
- Caloric restriction (typically 500-1000 kcal/day deficit) targeting 0.5-1 kg/week weight loss
- Any dietary pattern achieving caloric deficit can be effective (low-fat, low-carbohydrate, Mediterranean, etc.)
- Reducing energy-dense foods, sugar-sweetened beverages, and large portion sizes
Physical Activity:
- Physical fitness is an important predictor of all-cause mortality independent of BMI
- Aerobic exercise, resistance training, or both
- Sedentary behavior is independently associated with adverse metabolic outcomes
- Exercise preserves lean mass during weight loss
Behavioral Interventions:
- Cognitive behavioral therapy (CBT)
- Motivational interviewing
- Self-monitoring (food diaries, step counters)
- Regular follow-up and support groups
7.2 Pharmacological Treatment
Medications are indicated when BMI ≥30 kg/m², or BMI ≥27 kg/m² with at least one obesity-related comorbidity, after inadequate response to lifestyle modification.
| Drug Class | Examples | Mechanism | Expected Weight Loss |
|---|---|---|---|
| GLP-1 receptor agonists | Semaglutide (Wegovy), Liraglutide (Saxenda) | Hypothalamic appetite suppression, delayed gastric emptying | 10-15% (semaglutide up to 15-17%) |
| GIP/GLP-1 dual agonist | Tirzepatide (Zepbound) | Dual incretin receptor agonism | Up to 20-22% |
| Phentermine/topiramate ER | Qsymia | Sympathomimetic + anticonvulsant | ~8-10% |
| Naltrexone/bupropion ER | Contrave | Opioid antagonist + dopamine/NE reuptake inhibitor | ~4-6% |
| Orlistat | Xenical | Pancreatic lipase inhibitor, reduces fat absorption | ~3-5% |
Drug-induced weight gain (from other medications used for comorbidities) should always be addressed - switching to weight-neutral or weight-negative alternatives when possible
7.3 Surgical Treatment (Bariatric Surgery)
Indications:
- BMI ≥40 kg/m² without comorbidities, OR
- BMI ≥35 kg/m² with significant obesity-related comorbidities (T2DM, hypertension, OSA, etc.)
- Failure of prior nonsurgical attempts
Procedures and Outcomes:
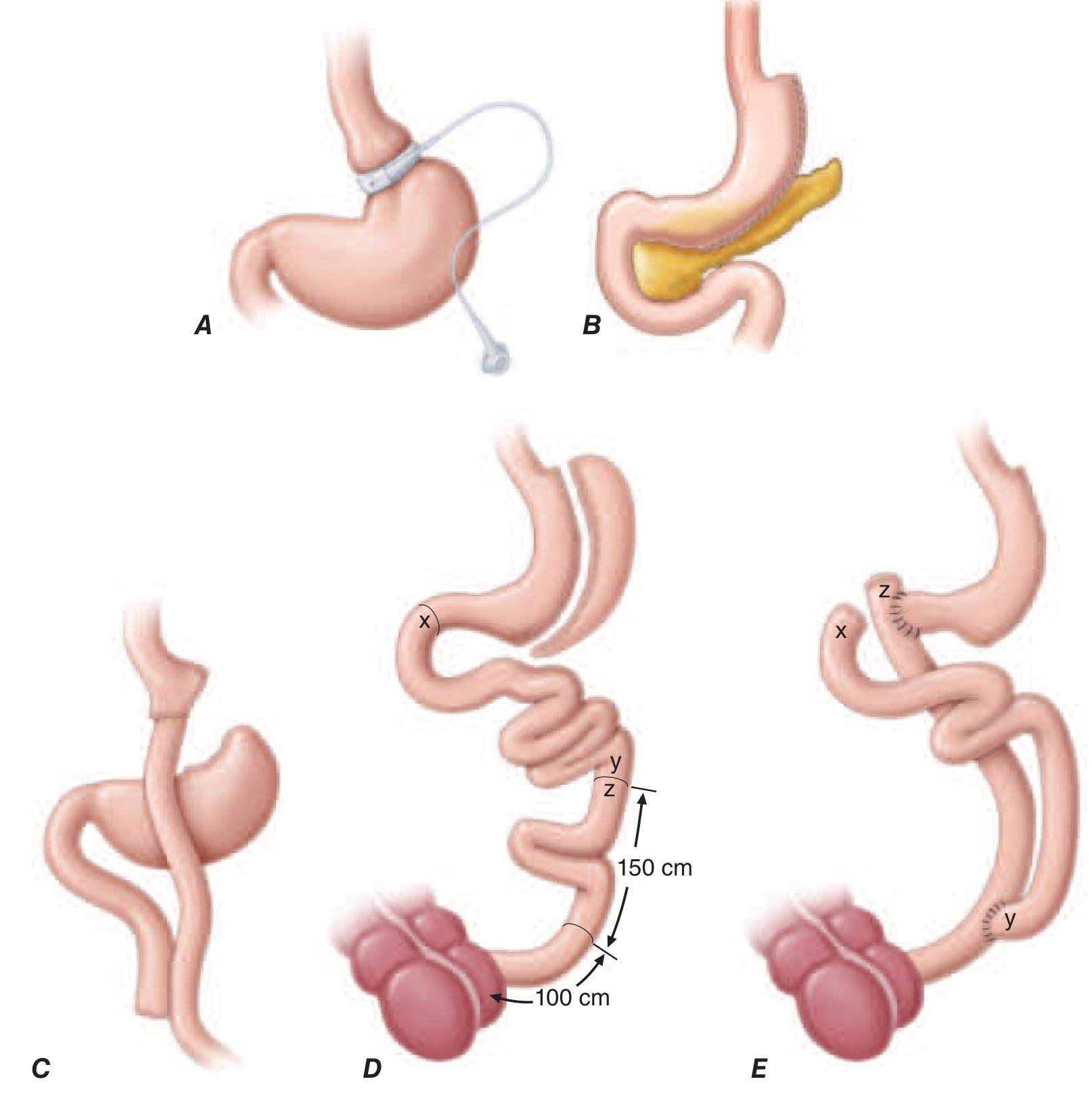
FIGURE 414-3 (Harrison's 22e) - Bariatric surgical procedures
| Procedure | Mechanism | Expected Weight Loss |
|---|---|---|
| Laparoscopic sleeve gastrectomy (LSG) | Restrictive - removes ~80% of stomach | 20-25% total body weight |
| Roux-en-Y gastric bypass (RYGB) | Restrictive + malabsorptive | 28-33% total body weight |
| Adjustable gastric banding | Restrictive only | 15-20% total body weight |
| Biliopancreatic diversion with duodenal switch (BPD/DS) | Primarily malabsorptive | 30-40% total body weight |
Outcomes of bariatric surgery:
- 28-33% average total body weight loss at 12-18 months (RYGB/sleeve)
- Significant improvement in T2DM, hypertension, dyslipidemia, OSA, and quality of life
- Meta-analysis: surgery associated with reduced mortality (OR = 0.55 cardiovascular death, OR = 0.70 all-cause mortality) vs. no surgery
- Swedish Obese Subjects Study (15-year data): 78% reduction in incidence of T2DM development in surgically treated patients
- 68.2% of patients with T2DM experienced complete remission within 5 years; however, one-third redeveloped T2DM within 5 years
- Mortality rate from bariatric surgery: generally <1%, varies with procedure, patient age, comorbidities, and surgical team experience
Complications:
- RYGB: Stromal stenosis or marginal ulcers (5-15%); treated with endoscopic balloon dilation and acid suppression
- Adjustable banding: Minimal absorptive abnormalities; micronutrient deficiencies uncommon if diet balanced
- Restrictive-malabsorptive procedures: Risk of micronutrient deficiencies - vitamin B₁₂, iron, folate, calcium, vitamin D - require lifelong supplementation
Factors predicting better T2DM remission after bariatric surgery:
- Not yet requiring insulin
- Shorter duration of disease
- Lower HbA1c at baseline
- Earlier-stage T2DM
7.4 Non-Surgical Endoscopic Techniques
Endoscopic approaches offer reversible, minimally invasive methods:
-
Intraluminal gastric balloons - space-occupying devices limiting gastric volume, decreasing hunger. Must be removed after 6 months. Weight loss: 6-12% at device removal. Adverse effects: nausea, vomiting, abdominal pain.
-
Endoscopic sleeve gastroplasty (ESG) - suturing reduces gastric volume, induces early satiety. More durable than balloons.
-
Aspiration therapy - endoscopic tube placed in stomach allowing aspiration of portion of meal after eating.
8. SPECIAL POPULATIONS AND CONSIDERATIONS
Sleep and Obesity
- Sleep deprivation is associated with metabolic alterations in appetite regulation (↑ ghrelin, ↓ leptin), sympathetic nervous system overactivity, reduced insulin sensitivity, and circadian rhythm disturbances
- OSA must be identified and treated - CPAP therapy can improve metabolic parameters
Obesity in Pregnancy
- Maternal obesity increases risks of gestational diabetes, pre-eclampsia, stillbirth, macrosomia, and cesarean delivery
- Intrauterine exposure to diabetic/obese environment increases offspring's risk of obesity and T2DM
Childhood Obesity
- Using age- and sex-specific BMI cutoffs: overweight ≥91st percentile; obesity ≥99th percentile
- Childhood obesity tracks strongly to adult obesity and metabolic disease
Medications to Prefer/Avoid in Obese Patients
Weight-promoting medications to consider switching (Goldman-Cecil):
- Antihypertensives: beta-blockers (especially older agents), alpha-blockers
- Alternatives: ACE inhibitors, ARBs, calcium channel blockers, diuretics
9. PROGNOSIS
- Even modest weight loss (5-10% of body weight) produces clinically meaningful improvements in blood pressure, glycemia, lipids, and sleep apnea
- Weight regain is common after non-surgical interventions; obesity is a chronic, relapsing disease requiring long-term management
- Bariatric surgery produces the most durable weight loss outcomes
- Physical fitness independently predicts mortality regardless of BMI - improving cardiorespiratory fitness even without weight loss has substantial health benefits
Summary
| Domain | Key Points |
|---|---|
| Definition | BMI ≥30 kg/m² (WHO); Extreme obesity ≥40 kg/m² |
| Prevalence | 42.4% US adults; tripled globally since 1975 |
| Etiology | Gene-environment interaction; leptin/MC4R pathways; obesogenic environment |
| Complications | T2DM, CVD, dyslipidemia, OSA, NAFLD, cancer (≥13 types), PCOS, OA |
| Diagnosis | BMI + waist circumference + metabolic labs |
| Lifestyle Rx | Diet + exercise + behavioral therapy (foundation) |
| Pharmacotherapy | GLP-1 agonists (semaglutide/tirzepatide) most effective; orlistat least effective |
| Surgery | RYGB gold standard; 28-33% weight loss; <1% mortality |
| Endoscopy | Gastric balloons (6-12% loss); ESG (more durable) |
| Prognosis | Chronic relapsing disease; 5-10% loss clinically meaningful |
Sources: Harrison's Principles of Internal Medicine 22E (2025), p. 3227-3292 (Chapters 413-414); Goldman-Cecil Medicine, Ch. 201; Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Ch. 7
This is a shared conversation. Sign in to Orris to start your own chat.