Nasal septum
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Here is a comprehensive overview of the nasal septum, drawn from Scott-Brown's Otorhinolaryngology, Cummings Otolaryngology, Color Atlas of Human Anatomy, and K.J. Lee's Essential Otolaryngology.
Nasal Septum
Structure
The nasal septum is the midline partition that divides the nasal cavity into right and left nasal passages. It has three components:
1. Bony Portion
- Perpendicular plate of the ethmoid - forms the upper one-third; continuous superiorly with the cribriform plate and crista galli; posteriorly articulates with the sphenoid crest and posteroinferiorly with the vomer
- Vomer - forms the posterior and inferior septum; its two alae articulate with the sphenoid rostrum, creating the vomerovaginal canals (transmitting pharyngeal branches of the maxillary artery); its inferior border sits on the nasal crest of the maxilla and palatine bones
- Maxillary crest and palatine bone - contribute to the inferior nasal crest
2. Cartilaginous Portion
- Quadrilateral (septal) cartilage - bound by collagenous fibers to the nasal bones, perpendicular plate of ethmoid, and vomer; continuous with the upper lateral cartilages at the nasal bridge
- The sphenoidal process (septal tail) extends posteriorly between the vomer and perpendicular plate, and is a useful source of graft cartilage in revision rhinoplasty
- The inferior attachment to the maxillary crest is through looser connective tissue forming a pseudoarthrosis - this joint allows mobility during trauma, reducing fracture risk
3. Membranous Portion
- A segment of connective tissue between the caudal septal cartilage and the columella
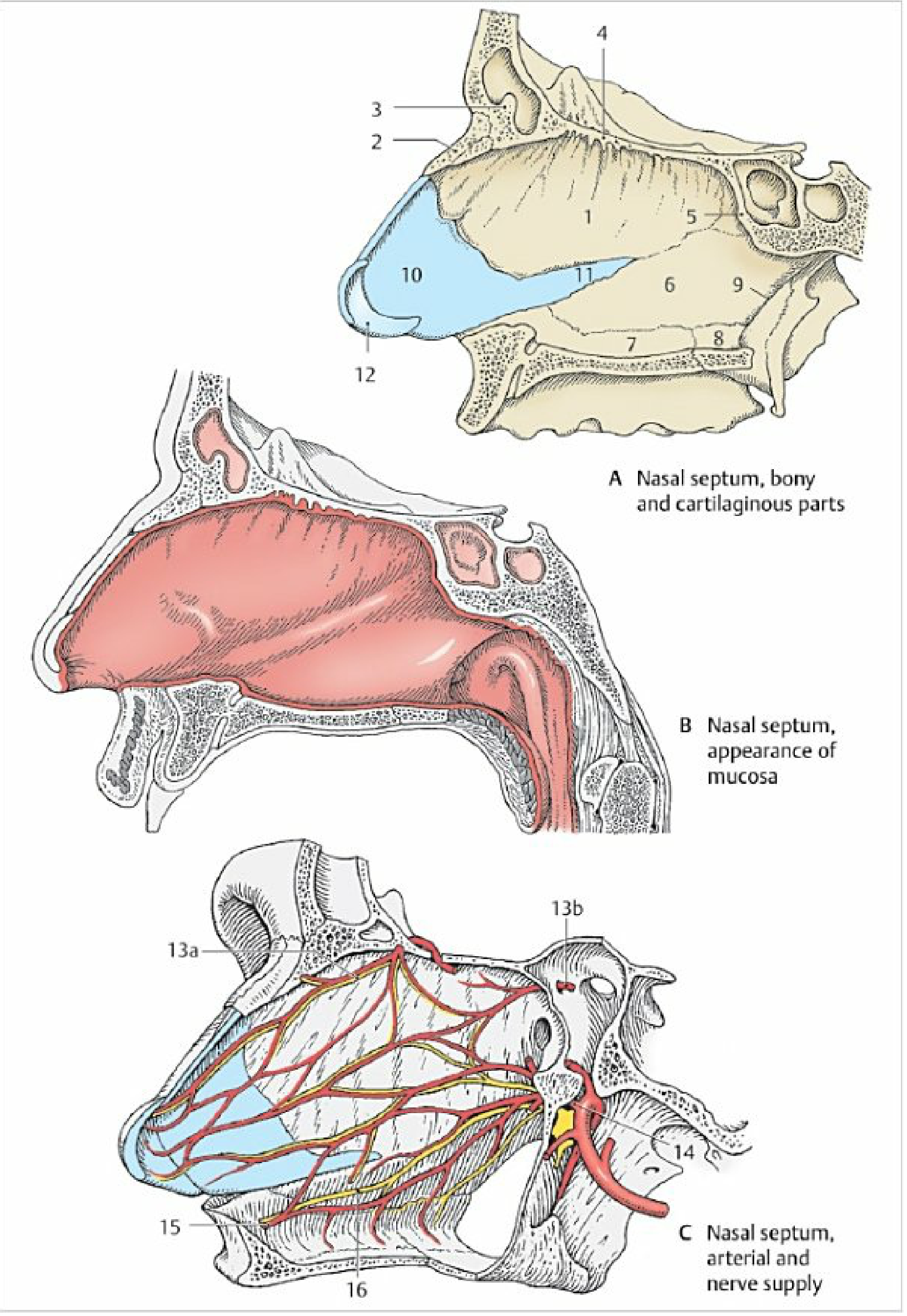
Fig. Nasal septum: (A) bony and cartilaginous parts, (B) appearance of mucosa, (C) arterial and nerve supply - Color Atlas of Human Anatomy
Functions
- Separates the nasal airway into two distinct chambers
- Supports the nasal dorsum
- Maintains shape of the columella and nasal tip
- Forms part of the nasal valves
- Contributes to humidification, filtration, and olfaction
Blood Supply
The nasal septum receives a dual supply from both the internal carotid (via ophthalmic artery) and external carotid (via maxillary and facial arteries):
| Region | Arteries |
|---|---|
| Anterior/superior | Anterior and posterior ethmoidal arteries (from ophthalmic artery) |
| Posterior | Sphenopalatine artery (from maxillary artery), passing through the sphenopalatine foramen |
| Inferior | Greater palatine artery; anastomoses via the incisive canal |
| Anterior inferior | Superior labial artery (from facial artery) |
Kiesselbach's Plexus (Little's Area)
- Located at the anteroinferior nasal septum (approximately 1.5 mm wide)
- Formed by anastomoses of: posterior septal branch of sphenopalatine artery + anterior and posterior ethmoidal arteries + greater palatine artery + superior labial artery
- The most common site of anterior epistaxis, particularly in young patients
Woodruff's Plexus
- Located in the posterior inferior meatus
- Now known to be venous in nature (not arterial as once thought)
- Site of posterior epistaxis, especially in elderly patients
Nerve Supply
- Anterior/superior septum: branches of the ophthalmic nerve (CN V1) - anterior ethmoidal nerve
- Posterior septum: branches of the maxillary nerve (CN V2), including the nasopalatine nerve, which passes through the incisive canal to supply the hard palate
Mucosa
- Respiratory region: pseudostratified ciliated columnar epithelium with goblet cells; cilia beat toward the pharynx; contains a well-developed cavernous venous plexus - the thickened anterior part of this plexus is the most frequent site of epistaxis
- Olfactory region: located on the upper part of the septum where it meets the cribriform plate; contains olfactory cells, supporting cells, and basal cells (400-500 µm thick)
Development (Embryology)
- The nasal septum develops as a downgrowth from the merged medial nasal processes and nasofrontal process, defining the right and left nasal cavities
- Fusion with the palatine processes begins anteriorly at week 9 and is completed posteriorly by week 12
- Vomeronasal organs (Jacobson's organs): form as epithelial diverticula on each side of the septum in late embryonic period; begin to regress before birth, leaving the vomeronasal cartilages as adult remnants (useful as cartilage grafts)
Venous Drainage
- Anterior and posterior ethmoid veins → superior ophthalmic vein → cavernous sinus
- Sphenopalatine vein → pterygoid plexus
- Diploic veins of Breschet (frontal sinuses)
This is a valveless venous system, creating potential for retrograde spread of infection intracranially (especially to the cavernous sinus).
Lymphatic Drainage
- Anterior nose: submandibular lymph nodes + superficial cervical nodes
- Posterior nose: retropharyngeal and deep cervical lymph nodes
Clinical Relevance
Deviated Nasal Septum (DNS)
- Very common; adults almost always show some deviation, typically at the junction between the cartilaginous and bony parts (where the vomeronasal cartilage lies)
- Causes: trauma (birth trauma, childhood microfractures), developmental asymmetry
- Consequences: unilateral nasal obstruction, paradoxical nasal obstruction (patient feels obstruction on the contralateral - less deviated - side due to turbinate enlargement), impaired olfaction, dry mucosa, epistaxis from septal varices, and potentially chronic sinusitis
- L-strut: at least 1 cm of dorsal septum and 1 cm of caudal septum is preserved during surgery to maintain nasal support
Septoplasty
- Surgery to straighten the deviated septum; performed through an intranasal incision with elevation of bilateral mucoperichondrial flaps
- ~20-30% of patients do not have full symptom resolution; this can be under 10% with optimal technique
- Key complications: septal perforation (bilateral mucosal tears without repair), loss of dorsal/tip support
Septal Perforation
- Can follow septoplasty, trauma, cocaine use, Wegener's granulomatosis, or syphilis
- Presents with crusting, whistling, epistaxis, or saddle-nose deformity
- Bilateral mucosal tears during surgery should be repaired and an interposition graft placed
Epistaxis (Nosebleed)
- Anterior (most common, >90%): from Kiesselbach's plexus - young patients, nose picking, hypertension, anticoagulants
- Posterior: from Woodruff's plexus - elderly patients, more severe
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1 | Cummings Otolaryngology Head and Neck Surgery | Color Atlas of Human Anatomy Vol. 2 | K.J. Lee's Essential Otolaryngology
This is a shared conversation. Sign in to Orris to start your own chat.