Intercoastal nerve block. Clinical anatomy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
I now have comprehensive content from four authoritative textbooks. Let me compose the full response.
Intercostal Nerve Block - Clinical Anatomy
Overview of the Intercostal Nerves
The intercostal nerves are the anterior primary rami (ventral rami) of thoracic spinal nerves T1-T11. The 12th thoracic anterior ramus runs below the 12th rib as the subcostal nerve. Each nerve exits the spine through the intervertebral foramen, which lies midway between two adjacent ribs.
Upon exiting, each nerve immediately gives off:
- Posterior (dorsal) cutaneous branch - supplies the skin and muscles of the paraspinal area
- Lateral cutaneous branch - arises at the midaxillary line; supplies the anterior and posterior lateral chest wall
- Anterior cutaneous branch - the terminal branch
- Gray's Anatomy for Students, p. 197
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 675
Neurovascular Bundle - The Key Anatomical Relationship
Each intercostal nerve travels with its corresponding intercostal artery and vein within the subcostal groove - a channel on the ventral (inferior) surface of each rib. The arrangement within the groove, from superior to inferior, is:
| Position | Structure |
|---|---|
| Superior (most protected) | Intercostal Vein |
| Middle | Intercostal Artery |
| Inferior | Intercostal Nerve |
The mnemonic VAN (Vein, Artery, Nerve) describes this top-to-bottom order. The vein and artery lie above the nerve and are therefore somewhat protected by the rib during a nerve block - but the nerve itself is the most inferiorly exposed structure.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 675
Muscular Layers of the Intercostal Space
The intercostal space is bound by three muscular layers:
- External intercostal muscle - outermost; fibers run inferomedially
- Internal intercostal muscle - middle layer
- Innermost intercostal muscle - deepest; separated from the internal intercostal by the neurovascular bundle
The neurovascular bundle runs between the internal intercostal and innermost intercostal muscles, deep to the subcostal groove. The fasciae of the internal and external intercostal muscles form the walls of the intercostal groove.
From Miller's Anesthesia (10th ed.), the intercostal space is described as a triangular space with:
- Medial border: posterior intercostal and innermost intercostal muscles, endothoracic fascia, and parietal pleura
- Lateral border: internal and external intercostal muscles and intercostal membrane
- Base: the lower rib
Deep to the innermost intercostal muscle lies the endothoracic fascia and then the parietal pleura - this is the critical structure to avoid.
- Miller's Anesthesia, 10th ed., p. 11085
- Barash Clinical Anesthesia, 9th ed., p. 2920
Why Block Position Matters
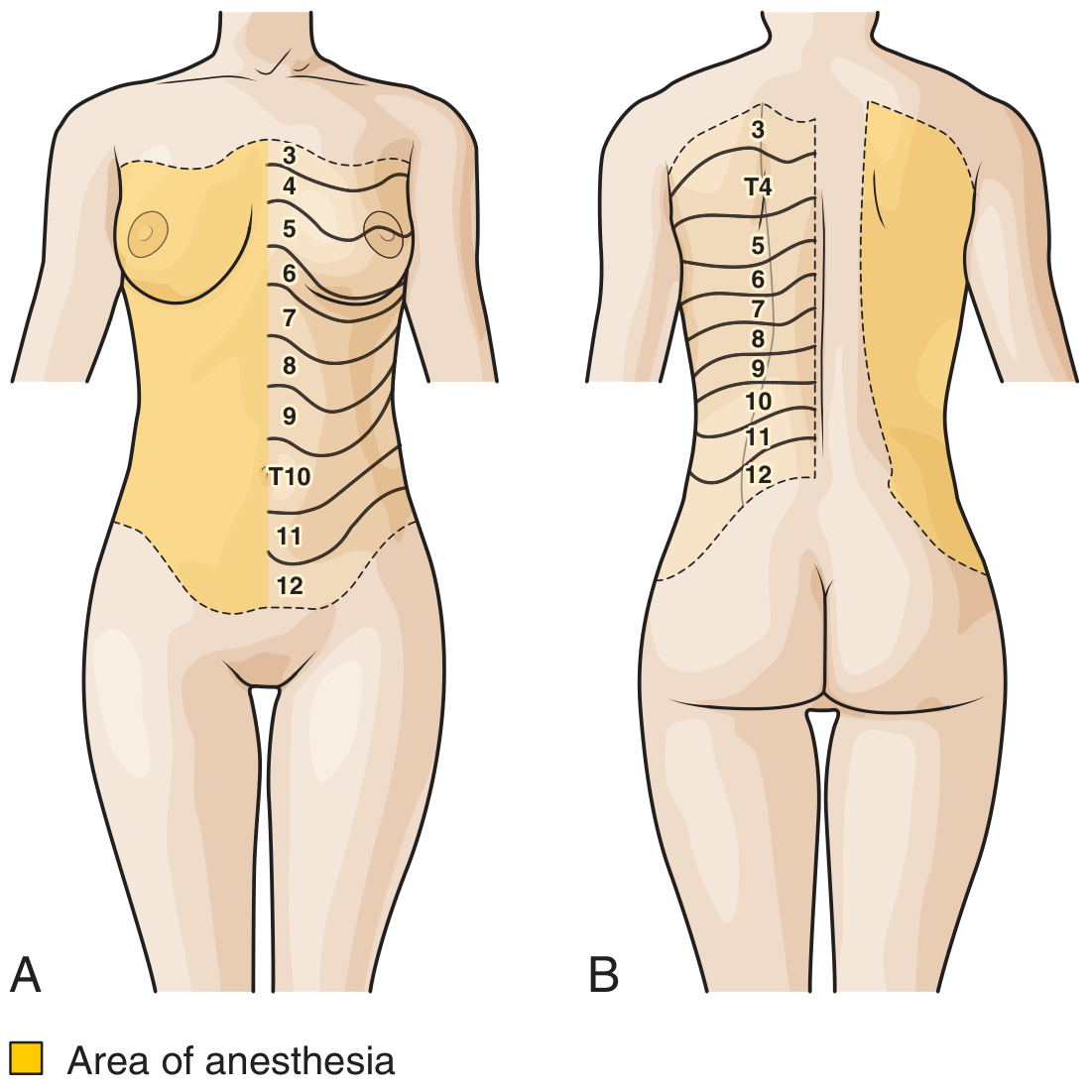
Cutaneous distribution of intercostal nerves T3-T12 - the shaded area shows the zone of anesthesia achieved (Roberts and Hedges)
The position of the block along the chest wall determines which branches are anesthetized:
| Block Location | Branches Blocked | Clinical Effect |
|---|---|---|
| Paravertebral / angle of rib (5-7 cm from midline) | All branches (posterior cutaneous + lateral cutaneous + anterior cutaneous) | Full dermatomal anesthesia |
| Posterior axillary line | Lateral cutaneous + anterior cutaneous | Adequate for rib fractures; most practical with buffer from internal intercostals |
| Midaxillary line | Anterior cutaneous only (lateral branch already given off) | Incomplete - misses lateral chest wall |
| Anterior chest wall | Anterior cutaneous only | Very limited coverage |
The nerve is blocked before the lateral cutaneous branch arises (i.e., proximal to the midaxillary line) to achieve complete dermatomal coverage. The posterior axillary line is the preferred site because the internal intercostal muscle here forms a buffer between the nerve and the pleura, reducing pneumothorax risk.
- Roberts and Hedges', p. 675
- Barash Clinical Anesthesia, 9th ed., p. 2990
Anatomical Changes Along the Rib
-
Posteriorly (near angle of rib, 5-7 cm from midline): The subcostal groove is well-defined and deep. The nerve is separated from the pleura only by the thin intercostal fascia here - careful technique required.
-
Anteriorly (beyond midaxillary line): The intercostal groove becomes progressively less well-defined. The nerves begin to move away from their protected position under the rib. This is why blocks are best performed posteriorly.
-
T1-T5 levels: These upper levels may be better approached via paravertebral block because the overlying scapula and bulky paraspinal musculature make intercostal access difficult.
-
Subcostal nerve (T12): Less closely associated with its rib, making it harder to identify and block with classic intercostal technique.
-
Barash Clinical Anesthesia, 9th ed., pp. 2990-2991
Ultrasound Anatomy
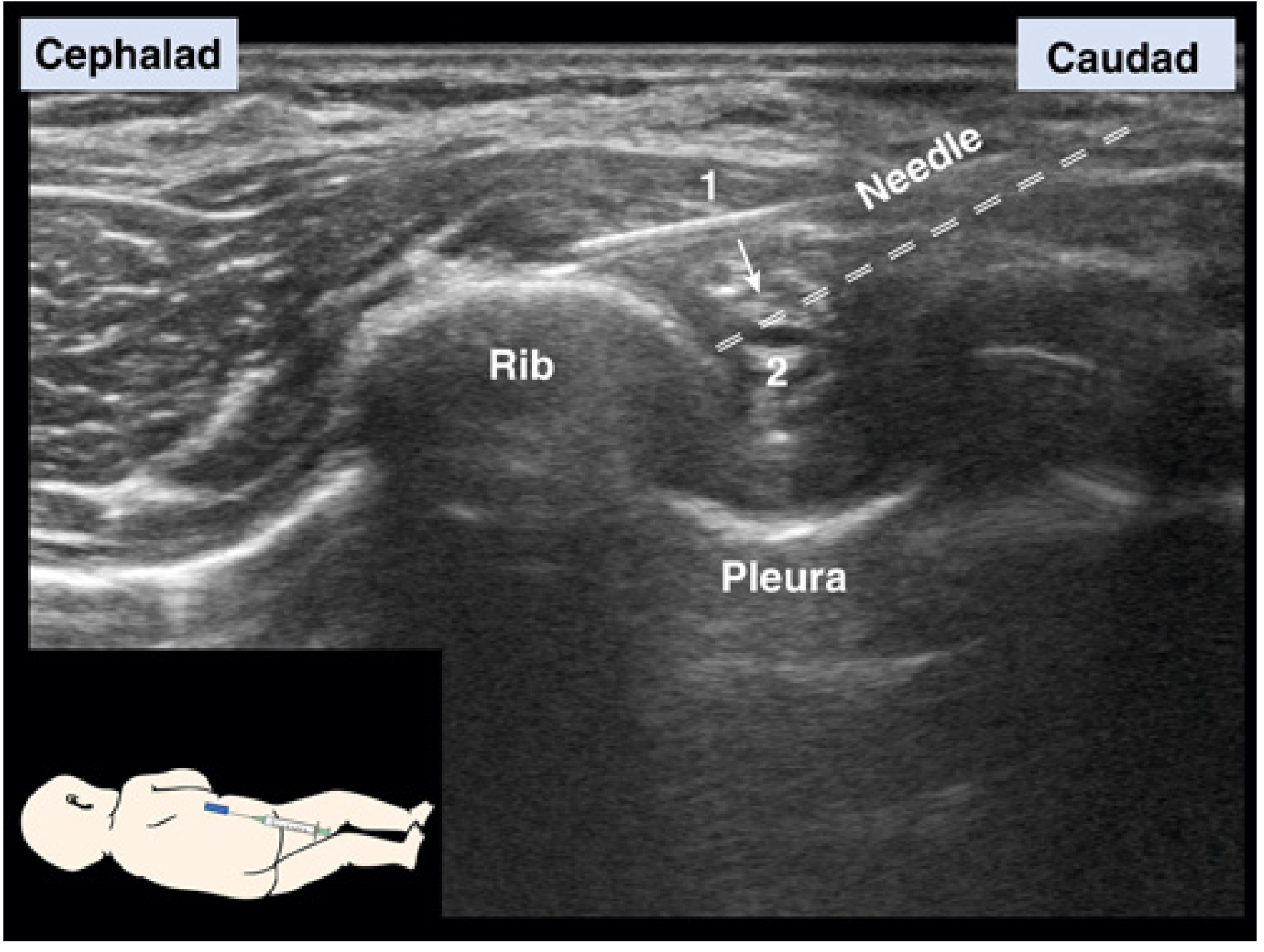
USG view: (1) needle contacts rib; (2) needle walks caudally off rib into the intercostal groove above the pleura (Miller's Anesthesia)
Under ultrasound, the key landmarks are:
- The rib (hyperechoic curved structure with posterior acoustic shadow)
- The parietal pleura (bright hyperechoic line below the rib, with sliding lung sign)
- The neurovascular bundle in the subcostal groove just inferior to the rib
Clinical Applications
| Indication | Levels Blocked |
|---|---|
| Rib fractures | Level of fractured rib ± 1-2 adjacent levels (for overlap) |
| Thoracotomy analgesia | Multiple levels covering incision |
| Cholecystectomy / upper abdominal surgery | T5-T12 (5-6 levels unilaterally) |
| Mastectomy | T2-T6 |
| Chest tube insertion | Level of tube insertion |
| Percutaneous biliary drainage | T6-T10 |
Because adjacent intercostal nerves overlap significantly, the rib of interest plus the two ribs above and below must be blocked for reliable analgesia.
Complications (Anatomically Explained)
-
Pneumothorax (most serious): Needle penetrates the parietal pleura, especially when blocking posteriorly where only thin intercostal fascia separates nerve from pleura. True incidence is low (<0.1% per Moore; ~1.4% per Shanti et al.)
-
Intravascular injection: The intercostal artery and vein lie immediately above the nerve in the groove. Intercostal vessels have high systemic uptake - highest of any peripheral block site - making local anesthetic toxicity a real concern
-
Hemothorax: Laceration of intercostal vessels
-
Incomplete block: Overlapping dermatomal supply from adjacent nerves, or block placed too anteriorly (distal to lateral cutaneous branch)
-
Roberts and Hedges', p. 675-676
-
Gray's Anatomy for Students, p. 197
Summary: The intercostal nerve block targets the anterior primary ramus of each thoracic spinal nerve as it travels in the costal groove between the internal and innermost intercostal muscles, accompanied by the intercostal artery (above) and vein (most superior). The ideal injection site is at the posterior angle of the rib (5-7 cm lateral to midline) or at the posterior axillary line, where the nerve has already given off the posterior cutaneous branch but not yet the lateral cutaneous branch, and where the internal intercostal muscle provides a safety buffer between needle and pleura.
anesthesia area and procedure
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Excellent - I have all the content and images needed. Here is the full, well-structured response.
Intercostal Nerve Block - Area of Anesthesia & Procedure
Area of Anesthesia
Blocking an intercostal nerve produces anesthesia in a band-like distribution around the thorax and upper abdomen corresponding to the dermatomal level blocked.
Area of anesthesia (shaded): Anterior and posterior views showing dermatomal coverage T3-T12 (Roberts and Hedges)
Dermatomal Map - Relevant Levels
| Level | Area Covered |
|---|---|
| T2-T3 | Upper chest, axilla, medial arm |
| T4 | Nipple line |
| T6 | Xiphoid |
| T10 | Umbilicus |
| T12 | Groin / inguinal ligament |
| T5-T12 (multiple) | Full abdominal wall from xiphoid to pubis - both sensory and motor |
Each block covers one dermatomal stripe. Because adjacent intercostal nerves overlap significantly, the target rib plus at least one rib above and one below must be blocked for reliable analgesia. For rib fractures, block the fractured level plus two adjacent ribs on each side.
Duration of Anesthesia
| Anesthetic Agent | Duration |
|---|---|
| Short-acting (lidocaine) | 1-3 hours |
| Long-acting (bupivacaine) alone | 6-8 hours |
| Long-acting + epinephrine | 8-12 hours (standard) |
| Partial/residual analgesia | Up to 3 days (possibly via reduced muscle spasm) |
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 675-676
Patient Positioning
Three positions are acceptable depending on context:
| Position | Best For |
|---|---|
| Prone (pillow under abdomen) | Operative anesthesia; allows access to both sides; arms draped over edge so scapula falls laterally |
| Lateral decubitus | Single-sided block; post-trauma patients who cannot lie flat |
| Sitting upright (arm raised, wrist rested on head) | Emergency department; rib fracture management; raises ipsilateral scapula off upper ribs |
- Barash Clinical Anesthesia, 9th ed., p. 2990
- Tintinalli's Emergency Medicine, p. 287
Landmark-Based Technique (Standard)
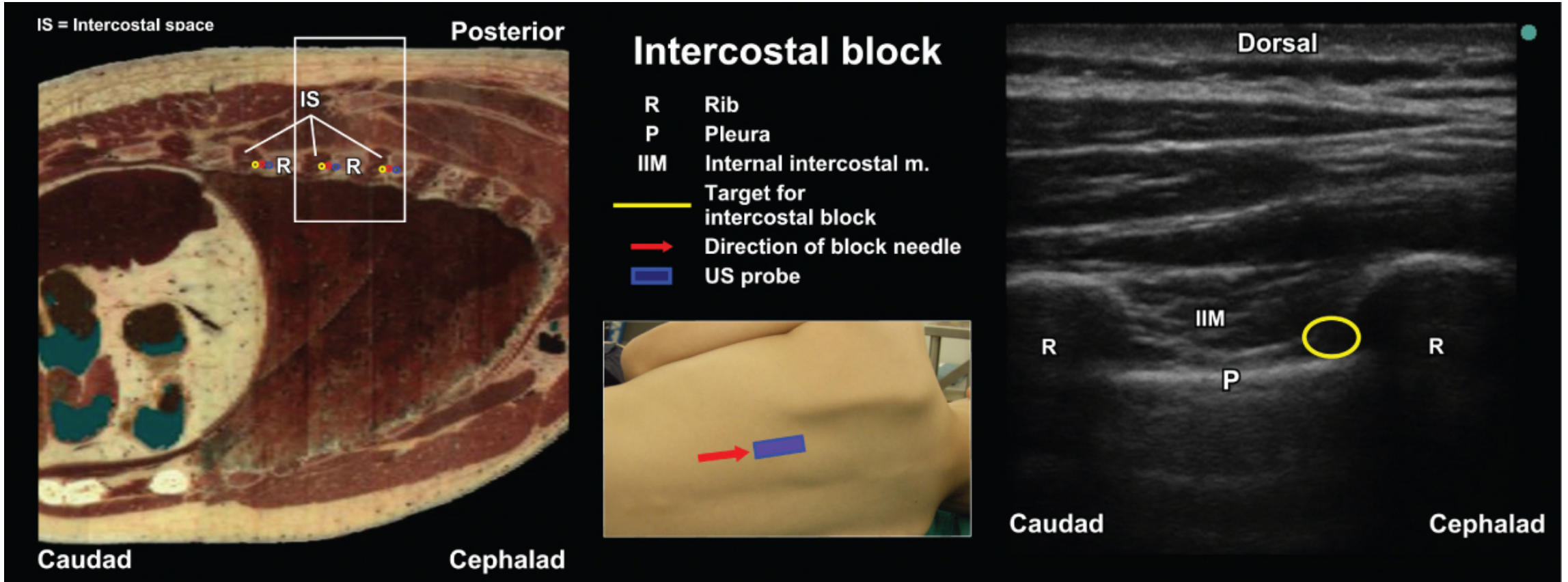
Left: Cross-sectional cadaveric anatomy showing intercostal spaces (IS) with neurovascular bundles (coloured dots) at rib inferior borders. Right: USG view - target zone (yellow circle) is between the internal intercostal muscle (IIM) and pleura (P), between two ribs (R). (Barash Clinical Anesthesia)
Step-by-Step
1. Mark the injection site
- Identify the target rib(s) at their angle of greatest posterior curvature, approximately 6-7 cm lateral to the midline (just lateral to the paraspinous muscles)
- For T1-T5: this region is obscured by the scapula; consider paravertebral block or use the posterior axillary line instead
- Mark the inferior border of each target rib
2. Set up
- Needle: 22-25 gauge, 3-4 cm (3.75 cm standard)
- Syringe: 5-10 mL
- Drug: 0.25-0.5% bupivacaine ± epinephrine, or 1-2% lidocaine
- Volume: 3-5 mL per level
- Aseptic technique; optional skin wheal of local anesthetic at each mark
3. Skin retraction (key step)
- Place the index finger of the non-injecting hand on the inferior border of the target rib
- Retract the overlying skin cephalad (upward) over the rib
4. Initial needle contact with rib
- Insert needle bevel-up at approximately 10-15° cephalad angulation
- Advance until the needle tip contacts the periosteum of the rib
- Rest the hand holding the syringe firmly on the chest wall for control
5. Walk the needle caudally off the rib
- Slowly release the skin retraction - this causes the shaft to shift and the tip moves toward the inferior rib margin
- Using the non-dominant hand to brace, gently "walk" the needle caudally until it slips off the inferior edge of the rib into the subcostal groove
- Advance only 3-4 mm beyond the rib edge - this places the tip between the internal intercostal and innermost intercostal muscles, at the neurovascular bundle
6. Aspiration and injection
-
Aspirate carefully - if blood returns, withdraw and reposition; if air returns, stop immediately (pleural entry)
-
If aspiration is negative: inject 3-5 mL of local anesthetic while gently moving the needle in and out 1 mm (to ensure compartment penetration and reduce risk of intravascular bolus)
-
Repeat for each level required
-
Roberts and Hedges', p. 675-676
-
Tintinalli's Emergency Medicine, p. 287
-
Barash Clinical Anesthesia, 9th ed., pp. 2990-2991
Ultrasound-Guided Technique
In-plane needle approach: (1) needle on rib, (2) needle walks into subcostal groove; pleura visible below (Miller's Anesthesia)
| Parameter | Value |
|---|---|
| Probe | High-frequency linear, 5-15 MHz |
| Orientation | Longitudinal (parasagittal) along the rib |
| Probe position | Posterior/lateral chest wall |
| Needle approach | In-plane (allows full needle visualization) |
USG landmarks to identify:
- Rib: hyperechoic curved line with posterior acoustic shadow (dark cone below)
- Pleura: bright hyperechoic line deep to the rib; shows dynamic sliding sign with respiration ("glittering")
- Internal intercostal membrane / muscle (IIM): hyperechoic layer immediately above the pleura
- Target injection zone: the space between the IIM and the pleura, just below the inferior rib border
Needle steps under USG:
- Advance in-plane until tip contacts the rib
- Tilt and redirect needle caudally, walking off the inferior rib border
- Stop when tip is in the intercostal groove, above the pleural line
- Confirm: local anesthetic spread appears as a hypoechoic fluid pocket pushing the pleura downward (away from the rib)
- Barash Clinical Anesthesia, 9th ed., p. 2992
Local Anesthetic Dosing Summary
| Agent | Concentration | Volume/Level | Onset | Duration |
|---|---|---|---|---|
| Lidocaine | 1-2% | 3-5 mL | Fast | 1-3 h |
| Bupivacaine | 0.25-0.5% | 3-5 mL | Slower | 6-12 h |
| Bupivacaine + epinephrine 1:200,000 | 0.25-0.5% | 3-5 mL | Moderate | 8-12 h |
| Ropivacaine | 0.5% | 3-5 mL | Moderate | 6-10 h |
Important: The intercostal space has the highest systemic absorption rate of any peripheral nerve block site. Calculate maximum total dose carefully - toxic serum levels can be reached rapidly, especially when blocking multiple levels.
Post-Procedure Monitoring
-
Observe for 30 minutes post-block
-
Routine chest radiograph is not indicated unless clinical signs appear
-
Bedside lung ultrasound (assess for absent sliding sign = pneumothorax) is preferred
-
Warning signs: cough, dyspnea, oxygen desaturation, chest pain → immediate evaluation
-
Tintinalli's Emergency Medicine, p. 287
-
Barash Clinical Anesthesia, 9th ed., p. 2993
Complications Summary
| Complication | Mechanism | Rate |
|---|---|---|
| Pneumothorax | Pleural puncture (especially posteriorly where only thin fascia separates nerve from pleura) | <0.1% (Moore); ~1.4% per level (Shanti) |
| Local anesthetic systemic toxicity (LAST) | High vascular uptake in intercostal space; cumulative dose across multiple levels | Dose-dependent |
| Intravascular injection | Needle in intercostal artery/vein (VAN relationship - artery just above nerve) | Prevented by aspiration |
| Hemothorax | Intercostal vessel laceration | Rare |
| Incomplete block | Block site too anterior (distal to lateral cutaneous branch), or inadequate dermatomal spread | Technique-dependent |
- Roberts and Hedges', p. 675-676
- Barash Clinical Anesthesia, 9th ed., p. 2993
This is a shared conversation. Sign in to Orris to start your own chat.