Oxygen Dissociation Curve - MD ANAESTHESIA PG EXAM - 30 marks major answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
I now have all the content needed to write a comprehensive 30-mark major answer. Let me compose it.
Oxygen Dissociation Curve - MD Anaesthesia PG Exam (30 Marks)
1. Introduction
The Oxygen Dissociation Curve (ODC), also called the Oxygen-Haemoglobin Dissociation Curve, is a graphical representation of the relationship between the partial pressure of oxygen (PO2) in blood and the percentage saturation of haemoglobin (Hb) with oxygen (or, alternatively, total O2 content per 100 mL of blood). It is one of the most fundamental concepts in respiratory physiology and has direct, daily relevance in anaesthesia practice.
Standard conditions for the normal ODC: pH 7.40, temperature 37°C, PCO2 40 mmHg, PO2 100 mmHg.
2. The Curve - Description and Shape
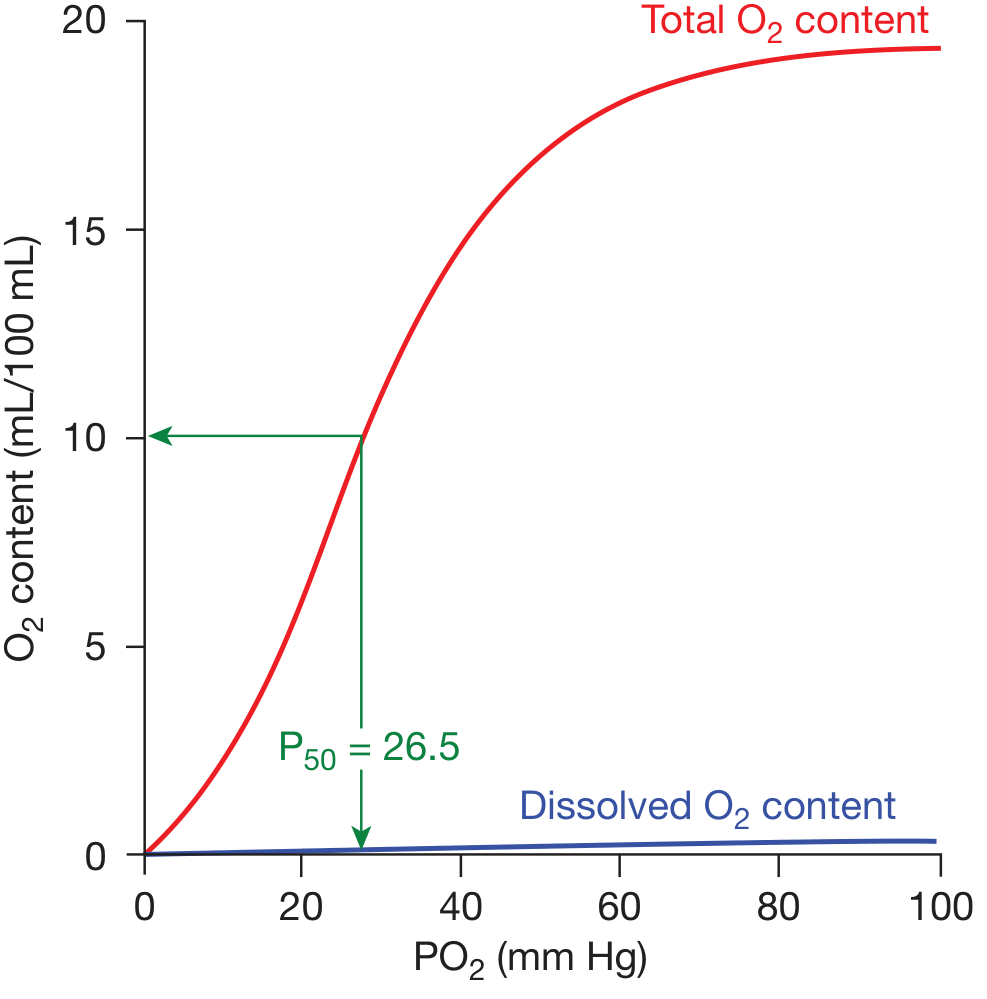
Figure: ODC - Total O2 content (red) and dissolved O2 (blue) versus PO2. P50 = 26.5 mmHg. (Fishman's Pulmonary Diseases)
The ODC is sigmoid (S-shaped), not hyperbolic, and this shape is physiologically critical. The curve has three functional zones:
| Zone | PO2 Range | Functional Significance |
|---|---|---|
| Upper flat portion | 60-100 mmHg | Loading zone (lungs) - Hb stays 90-100% saturated despite large drops in PO2 |
| Steep middle portion | 20-60 mmHg | Tissue unloading zone - small drop in PO2 releases large amounts of O2 |
| Lower flat portion | 0-20 mmHg | Reserve zone - myoglobin takes over at very low PO2 |
Key values on the normal ODC:
- At PO2 = 100 mmHg (arterial): SaO2 ≈ 97.5%, CaO2 ≈ 20 mL/dL
- At PO2 = 40 mmHg (mixed venous): SvO2 ≈ 75%, CvO2 ≈ 15 mL/dL
- At PO2 = 60 mmHg: SaO2 ≈ 90% (critical clinical threshold)
- P50 = 26.5 mmHg (PO2 at 50% saturation at standard conditions)
Oxygen content formula:
CaO2 = (1.34 × Hb × SaO2) + (0.003 × PaO2) (Normal ≈ 20 mL/dL; dissolved O2 contributes only ~0.3 mL/dL)
3. Molecular Basis of the Sigmoid Shape
The sigmoid shape results from cooperative binding (positive cooperativity) - a property unique to the tetrameric haemoglobin molecule:
- Haemoglobin exists in two conformations: T-state (tense/deoxy) with low O2 affinity, and R-state (relaxed/oxy) with ~300× higher O2 affinity.
- Binding of the first O2 molecule to one haem group induces a conformational change (T→R transition) that increases affinity of remaining haem groups for O2.
- Each successive O2 molecule binds with progressively higher affinity.
- This cooperativity produces the S-shape, contrasted with myoglobin (a monomer) which has a hyperbolic curve and cannot release O2 efficiently at tissue PO2 levels.
"The net effect of this cooperativity is that the affinity of hemoglobin for the last oxygen molecule bound is ~300 times greater than its affinity for the first oxygen molecule bound." - Lippincott's Biochemistry, 8th Ed.
4. P50 - Definition and Clinical Importance
P50 is the partial pressure of O2 at which haemoglobin is 50% saturated with O2 at standard conditions (pH 7.4, 37°C, PCO2 40 mmHg).
- Normal P50 = 26.5 mmHg
- A higher P50 (rightward shift) = decreased O2 affinity = more O2 released to tissues
- A lower P50 (leftward shift) = increased O2 affinity = O2 held tighter, less released to tissues
P50 is the single quantitative index of haemoglobin-O2 affinity.
5. Factors Shifting the ODC
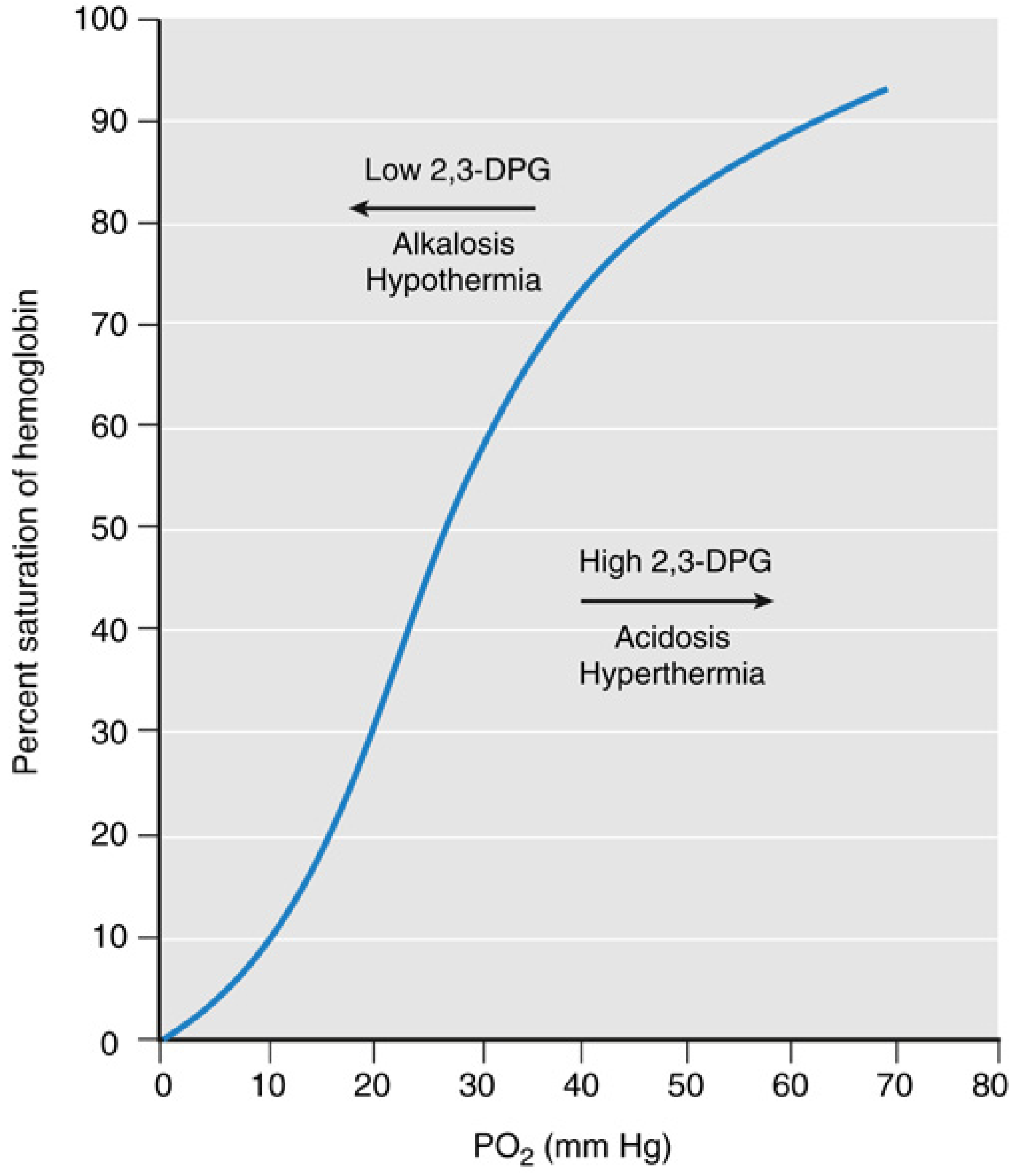
Figure: Factors shifting the ODC. (Miller's Anesthesia, 10e)
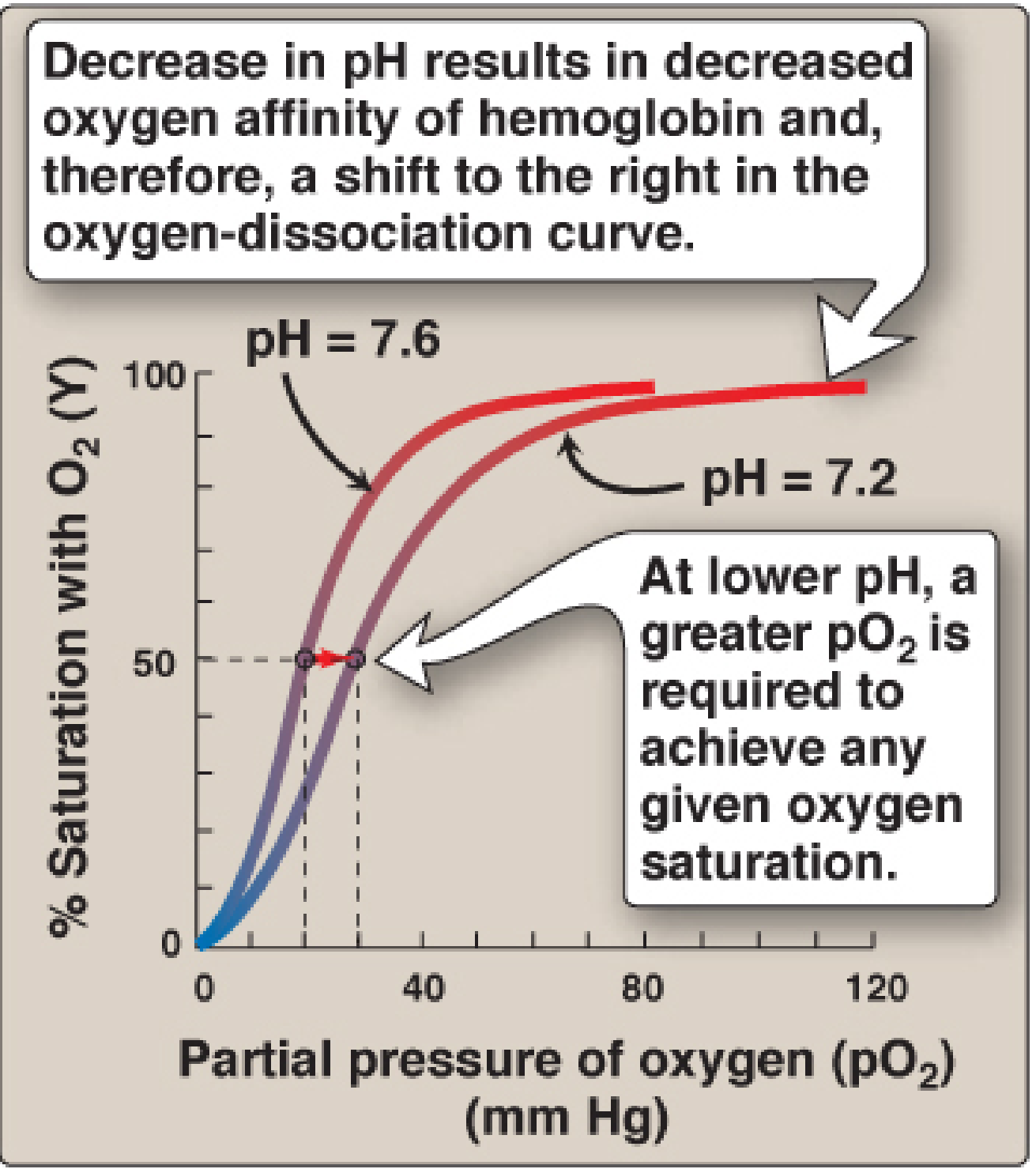
Figure: Effect of pH on ODC - Bohr effect. (Lippincott's Biochemistry, 8th Ed)
Mnemonic: "CADET, face Right!"
CO2 ↑, Acid (↓pH), DPG (2,3-DPG ↑), Exercise/Elevated temperature → Right shift
Opposite → Left shift
5A. Right Shift (Increased P50 - More O2 Released)
| Factor | Mechanism |
|---|---|
| ↑ Temperature | Directly weakens Hb-O2 bond |
| ↓ pH (acidosis) | Bohr effect - H+ stabilizes T-state |
| ↑ PCO2 | Direct carbamino binding + Bohr effect |
| ↑ 2,3-DPG | Binds deoxy-Hb β-chains, stabilizes T-state |
| Exercise | All four factors above simultaneously |
5B. Left Shift (Decreased P50 - O2 Held Tighter)
| Factor | Mechanism / Clinical Setting |
|---|---|
| ↓ Temperature / Hypothermia | Intraoperative cooling, CPB, hypothermic cardiac arrest |
| ↑ pH (alkalosis) | Hyperventilation, sodium bicarbonate administration |
| ↓ PCO2 | Iatrogenic hyperventilation |
| ↓ 2,3-DPG | Stored blood (within 24-48h), hypothyroidism, hexokinase deficiency |
| Fetal Hb (HbF) | γ-chains don't bind 2,3-DPG |
| Methaemoglobinaemia | Oxidised Fe3+ - non-functional |
| CO poisoning | Carboxyhaemoglobin + left shift of residual Hb |
| Myoglobin | Intrinsically hyperbolic, extremely left-shifted |
6. The Bohr Effect
Discovered by Christian Bohr (1904), this effect describes how increased H+ and CO2 cause a rightward shift of the ODC, facilitating O2 unloading in the tissues:
- In metabolically active tissues: CO2 ↑ → H2CO3 → H+ ↑ → pH ↓ → ODC shifts right → O2 unloads
- In the lungs: CO2 diffuses out → pH ↑ → ODC shifts left → Hb loads with O2
Mechanism: H+ ions bind to His residues (particularly His HC3 β-146) on deoxyhaemoglobin, forming salt bridges (ionic bonds) that stabilise the T-state. This causes H+ to be an allosteric effector. The Bohr effect can be summarised:
HbO2 + H⁺ ⇌ HbH⁺ + O2
At rest, the Bohr effect contributes an estimated 2-3% augmentation in O2 release due to the small arteriovenous pH difference (~0.03 units). Its effect is amplified during exercise.
7. 2,3-Diphosphoglycerate (2,3-DPG)
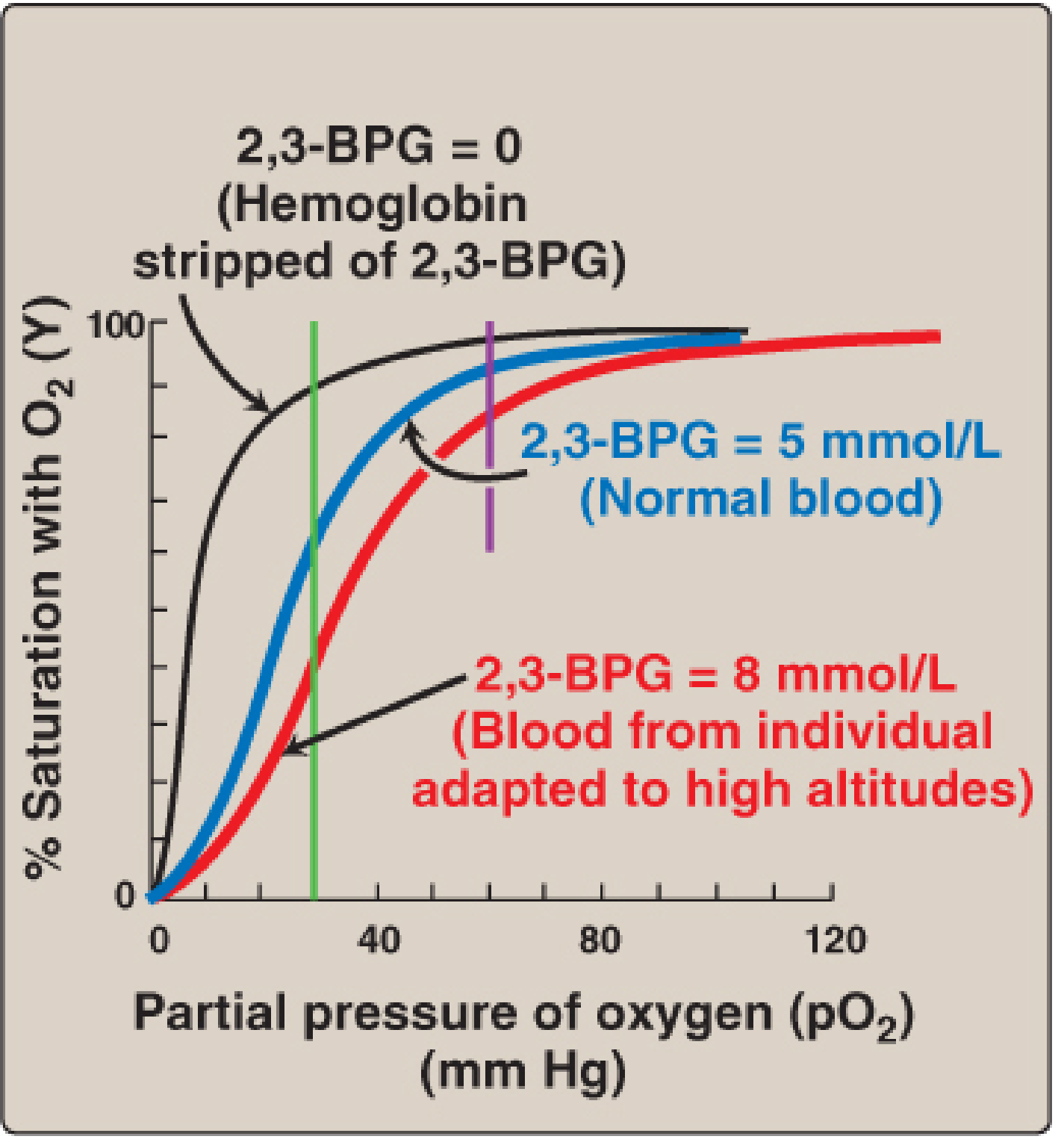
Figure: Effect of 2,3-BPG concentration on ODC. (Lippincott's Biochemistry, 8th Ed)
- Synthesised from 1,3-bisphosphoglycerate in the Luebering-Rapoport shunt of glycolysis (within RBCs)
- Normal concentration: ~5 mmol/L in erythrocytes
- Binds exclusively to deoxy-Hb in the central cavity formed by two β-chains, stabilising the T-state
- One molecule of 2,3-DPG binds to four positively-charged amino acids in the β-chain pocket
2,3-DPG increases in:
- Anaemia (compensatory)
- Hypoxia/high altitude
- Thyroid hormone excess
- Growth hormone excess
- Pyruvate kinase deficiency
2,3-DPG decreases in:
- Stored blood (major anaesthetic concern - falls within 24-48h)
- Hexokinase deficiency
- Hypothyroidism
- Acidosis (paradox: acidosis right-shifts acutely, but chronically suppresses 2,3-DPG synthesis)
8. Factors Affecting the ODC - Complete Summary Table
| Factor | Direction | P50 Change | Clinical Example in Anaesthesia |
|---|---|---|---|
| Acidosis (↓pH) | Right | ↑ | Sepsis, trauma, metabolic acidosis |
| Alkalosis (↑pH) | Left | ↓ | Hyperventilation, NaHCO3 |
| ↑ CO2 | Right | ↑ | Rebreathing, hypoventilation |
| ↓ CO2 | Left | ↓ | Mechanical hyperventilation |
| ↑ Temperature | Right | ↑ | Malignant hyperthermia, fever |
| ↓ Temperature | Left | ↓ | CPB, deliberate hypothermia |
| ↑ 2,3-DPG | Right | ↑ | Altitude, anaemia, hypoxia |
| ↓ 2,3-DPG | Left | ↓ | Stored blood, bank blood transfusion |
| CO poisoning | Left | ↓ (+ functional anaemia) | Fire victims, CO exposure |
| Methaemoglobinaemia | Left | ↓ | Prilocaine, nitrites, dapsone |
| HbF | Left | ↓ | Neonates, HDFN |
| HbS (sickle) | Right | ↑ | Sickle cell anaemia |
9. Carbon Monoxide and the ODC
CO binds Hb with 240 times greater affinity than O2. Its effects are twofold:
- Functional anaemia - CO occupies haem sites, reducing O2-carrying capacity (major effect)
- Left shift of ODC - remaining oxy-Hb molecules have increased O2 affinity and release O2 poorly to tissues
This combination makes CO poisoning particularly lethal - the patient may have an apparently normal PaO2 on ABG (dissolved O2 unaffected) while being profoundly hypoxic at the tissue level. Pulse oximetry cannot distinguish HbO2 from HbCO, giving falsely normal SpO2.
Treatment: 100% O2 (displaces CO from Hb) or hyperbaric O2.
10. Fetal Haemoglobin (HbF) and the ODC
- HbF has γ-chains instead of β-chains
- γ-chains do not bind 2,3-DPG (or bind it very poorly)
- Therefore HbF has a left-shifted ODC with P50 ~18-20 mmHg vs adult's 26.5 mmHg
- This left shift is physiologically advantageous: allows the fetus to extract O2 from maternal blood across the placenta
- After birth, HbF is replaced by HbA, with 2,3-DPG binding restoring normal P50
11. Anaesthesia-Specific Clinical Applications
A. Stored Blood and Transfusion
- 2,3-DPG falls rapidly in stored blood: by 50% at 1 week, nearly depleted by 3 weeks
- Left-shifted ODC in stored blood → O2 "stuck" to Hb → poor O2 delivery to tissues post-transfusion
- 2,3-DPG levels restore within 24-72 hours post-transfusion
- Anaesthetic implication: massive transfusion in acute haemorrhage may paradoxically worsen tissue O2 delivery transiently
B. Cardiopulmonary Bypass (CPB)
- Hypothermia during CPB causes a marked left shift
- Alkalosis from hyperventilation also left-shifts the curve
- Both impair O2 unloading at tissue level, but hypothermia also reduces metabolic demand
- pH-stat vs alpha-stat management strategies address this
C. Hyperventilation in Anaesthesia
- Mechanical hyperventilation → ↓PaCO2 → respiratory alkalosis → left shift
- Can reduce O2 release to tissues; particularly relevant during one-lung ventilation and neuro-anaesthesia
D. Malignant Hyperthermia (MH)
- Hyperthermia + acidosis + ↑CO2 → right shift
- O2 consumption increases dramatically; increases in O2 delivery are physiologically compensated by ODC shift
E. The "60-90 Rule" in Anaesthesia
- PaO2 of 60 mmHg corresponds to SaO2 ≈ 90% (on the shoulder of the curve)
- Below this, the curve enters the steep portion: a small fall in PaO2 causes a rapid, large fall in SaO2
- This is why 90% is the accepted minimum acceptable SpO2 threshold during anaesthesia
F. Pulse Oximetry and the ODC
- Pulse oximetry measures functional saturation (SpO2), not PaO2
- The shape of the ODC explains why SpO2 can be near-normal at PaO2 as low as 60 mmHg
- SpO2 > 95% does not guarantee adequate PaO2 (especially in high FiO2 situations)
12. Comparison: Myoglobin vs Haemoglobin vs HbF
| Property | Myoglobin | HbA (Adult) | HbF (Fetal) |
|---|---|---|---|
| Structure | Monomer | Tetramer (2α2β) | Tetramer (2α2γ) |
| Curve Shape | Hyperbolic | Sigmoid | Sigmoid |
| P50 (mmHg) | ~1-5 | 26.5 | ~18-20 |
| 2,3-DPG binding | None | Yes (β-chains) | Minimal (γ-chains) |
| Function | Intracellular O2 storage (muscle) | O2 transport in blood | O2 extraction from maternal blood |
13. Hill's Equation and Hill Coefficient
The sigmoid nature of the ODC is mathematically expressed by the Hill equation:
Y = PO2ⁿ / (P50ⁿ + PO2ⁿ)
Where Y = fractional saturation and n = Hill coefficient (cooperativity index)
- For Hb: n ≈ 2.7-3 (cooperativity)
- For myoglobin: n = 1 (no cooperativity - hyperbolic)
- A higher Hill coefficient = steeper sigmoid = more cooperative
14. Oxygen Delivery (DO2) and Extraction
Understanding the ODC is incomplete without relating it to O2 delivery and consumption:
DO2 = CO × CaO2 = CO × (1.34 × Hb × SaO2 + 0.003 × PaO2) (Normal ~1000 mL/min)
VO2 (O2 consumption) = Normal ~250 mL/min
O2 Extraction Ratio (OER) = VO2/DO2 ≈ 25% at rest
When DO2 falls (haemorrhage, low cardiac output, hypoxia), tissues compensate by extracting more O2 (OER increases), which is reflected in a decrease in mixed venous PO2 - moving the venous point down the steep part of the ODC.
Critical DO2 threshold: ~3-3.5 g/dL Hb equivalent - below which O2 supply fails to meet demand.
15. Summary Table - Left vs Right Shift
| Feature | Left Shift | Right Shift |
|---|---|---|
| O2 Affinity | Increased | Decreased |
| P50 | < 26.5 mmHg | > 26.5 mmHg |
| O2 Loading (lungs) | Better | Slightly reduced |
| O2 Unloading (tissues) | Worse | Better |
| Bohr effect direction | Alkalosis, ↓CO2 | Acidosis, ↑CO2 |
| Key anaesthetic causes | CPB hypothermia, hyperventilation, stored blood | Fever, acidosis, exercise, high altitude adaptation |
16. Conclusion
The Oxygen Dissociation Curve is not merely an academic concept - it is the physiological framework through which the anaesthetist understands oxygen transport, guides ventilatory management, interprets pulse oximetry, manages transfusions, and anticipates tissue oxygenation in every critically ill or peri-operative patient. The sigmoid shape, the P50, the Bohr effect, 2,3-DPG, and the effects of temperature and pH are all clinically actionable knowledge that directly influence anaesthesia and critical care decisions.
Key exam points:
- Normal P50 = 26.5 mmHg (pH 7.4, 37°C, PCO2 40 mmHg)
- PaO2 60 mmHg → SaO2 90% (critical threshold)
- Factors shifting right: "CADET" - CO2↑, Acidosis, DPG↑, Exercise, Temperature↑
- Stored blood is left-shifted (low 2,3-DPG) - impairs tissue O2 release post-transfusion
- CO causes left shift + functional anaemia; pulse ox reads falsely high
- HbF is left-shifted (γ-chains don't bind 2,3-DPG) - enables placental O2 transfer
- Hypothermia in CPB causes left shift - reduced O2 unloading (partly compensated by ↓metabolic demand)
Sources: Fishman's Pulmonary Diseases & Disorders | Miller's Anesthesia 10e | Guyton & Hall Medical Physiology | Lippincott's Biochemistry 8e | Barash Clinical Anesthesia 9e
This is a shared conversation. Sign in to Orris to start your own chat.