Explain Winging of Scapula
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the complete answer.
Winging of the Scapula
Definition
Winging of the scapula (also called scapula alata) is a condition in which the medial border and/or inferior angle of the scapula protrudes posteriorly away from the thoracic wall, producing a "wing-like" appearance. The direction of the winging depends on which nerve and muscle are affected. - Gray's Anatomy for Students, p. 847
Anatomy: Why the Scapula Wings
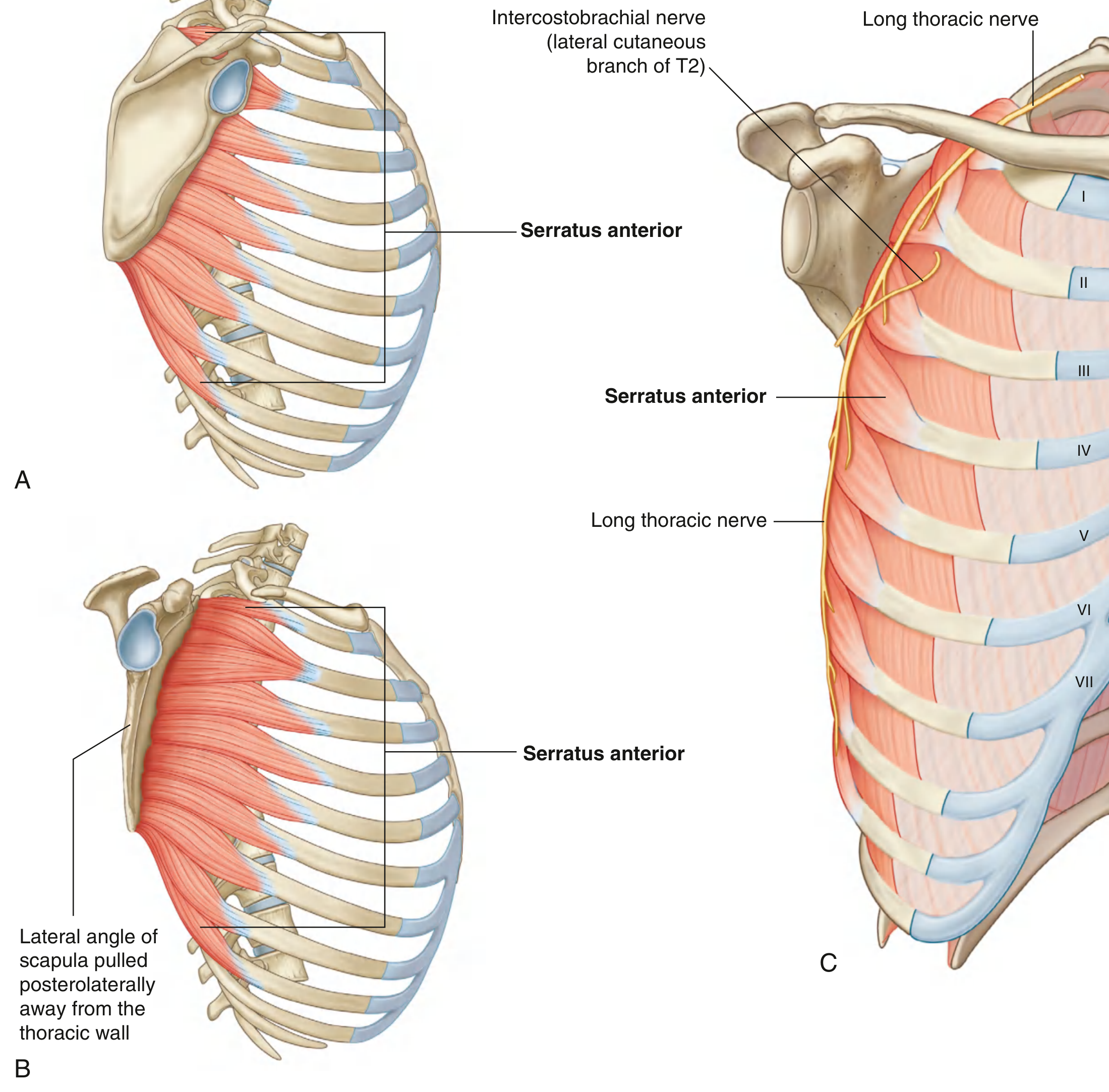
The serratus anterior muscle originates from the lateral surfaces of the upper 8-9 ribs and inserts on the costal (anterior) surface of the medial border of the scapula. Its two key functions are:
- Protraction and rotation of the scapula (necessary for arm elevation above 90°)
- Keeping the costal surface of the scapula closely apposed to the thoracic wall - Gray's Anatomy for Students
It is innervated by the long thoracic nerve (C5, C6, C7), which descends superficially along the lateral thoracic wall on the external surface of the serratus anterior muscle, just deep to skin and subcutaneous fascia - making it particularly vulnerable to injury.
Types of Scapular Winging
| Feature | Medial Winging | Lateral Winging |
|---|---|---|
| Nerve injured | Long thoracic nerve (C5-C7) | Spinal accessory nerve (CN XI) / Dorsal scapular nerve |
| Muscle paralyzed | Serratus anterior | Trapezius / Rhomboids |
| Inferior angle moves | Medially (elevated, translated medially) | Laterally |
| Mnemonic | SWIM - Serratus Winging is Inferior Medial | TRAWL - Trapezius/Rhomboids Are Winged Laterally |
- Miller's Review of Orthopaedics, 9th Ed, p. 405
Causes
1. Long Thoracic Nerve Palsy (most common cause - 55% of cases)
The long thoracic nerve is injured by:
- Direct trauma to the shoulder or lateral thoracic wall (football, falls, accidents)
- Carrying heavy loads on the shoulder ("rucksack paralysis") - the nerve is compressed by its superficial course
- Repetitive overhead activities - athletes, weight-lifters, throwing sports
- Iatrogenic - axillary lymphadenectomy (mastectomy, up to 10% of radical mastectomies), first rib resections, thoracotomies, scalenectomies, chest tube insertion, brachial plexus block
- Neuralgic amyotrophy (Parsonage-Turner syndrome) - accounts for the majority of non-traumatic cases
- Infections - viral, Lyme disease (painful long thoracic neuropathy)
- Familial brachial plexus neuropathy
- Radiation therapy for breast cancer (rare)
- Localization in Clinical Neurology, 8th Ed
2. Spinal Accessory Nerve (CN XI) Palsy - Lateral Winging
Paralysis of the trapezius muscle. CN XI is vulnerable in the posterior triangle of the neck (at Erb's point), where it can be damaged during:
- Cervical lymph node biopsy or radical neck dissection
- Penetrating trauma
3. Dorsal Scapular Nerve Palsy - Lateral Winging
Paralysis of the rhomboids (rhomboid major and minor). Much rarer due to the protected course of the nerve.
4. Non-neurological Causes
- Osteochondromas of the scapula or ribs
- Fracture malunions of the scapula
- Muscle contracture (e.g., in fascioscapulohumeral muscular dystrophy - causes bilateral winging)
- Voluntary winging (can be performed intentionally by some individuals)
- Miller's Review of Orthopaedics, 9th Ed
Clinical Features
- At rest: winging may not be apparent
- On pushing the arms forward against a fixed wall (the "wall push-up test" or "serratus anterior test"): the scapula becomes visibly winged, lifting away from the thoracic wall - especially the lower two-thirds
- Weakness raising the arm above the head (arm cannot be elevated past 90° because the scapula cannot rotate upward properly)
- Shoulder pain and fatigue on overhead activity
- With stretch injuries: sharp pain radiating from the shoulder to the neck and upper arm
"Nerve paralysis usually causes no deformity of the scapula when the arm is at rest. If, however, the patient is asked to push the arm forward against resistance... the scapula becomes winged, especially in its lower two-thirds region." - Localization in Clinical Neurology, 8th Ed
Clinical Testing
- Wall push-up test: Patient stands facing a wall, places both hands on the wall, and pushes. Winging of the medial border indicates serratus anterior weakness (long thoracic nerve palsy).
- Arm elevation: Ask the patient to flex the arm to 90° and hold it. Winging that increases with abduction suggests trapezius weakness (lateral winging).
Investigations
- EMG/Nerve conduction studies: Confirm the nerve involved; show denervation in the affected muscle
- MRI of the shoulder and chest wall: Assess the nerve and muscle
- Imaging (X-ray/CT): Rule out bony causes (osteochondroma, fracture)
Management
Conservative (first-line)
- Most cases of traumatic or post-viral long thoracic nerve palsy are self-limited and responsive to physical therapy
- Selective muscle strengthening exercises (serratus anterior rehabilitation)
- Bracing/taping in select cases
- Avoid aggravating activities
Surgical (for persistent or severe cases)
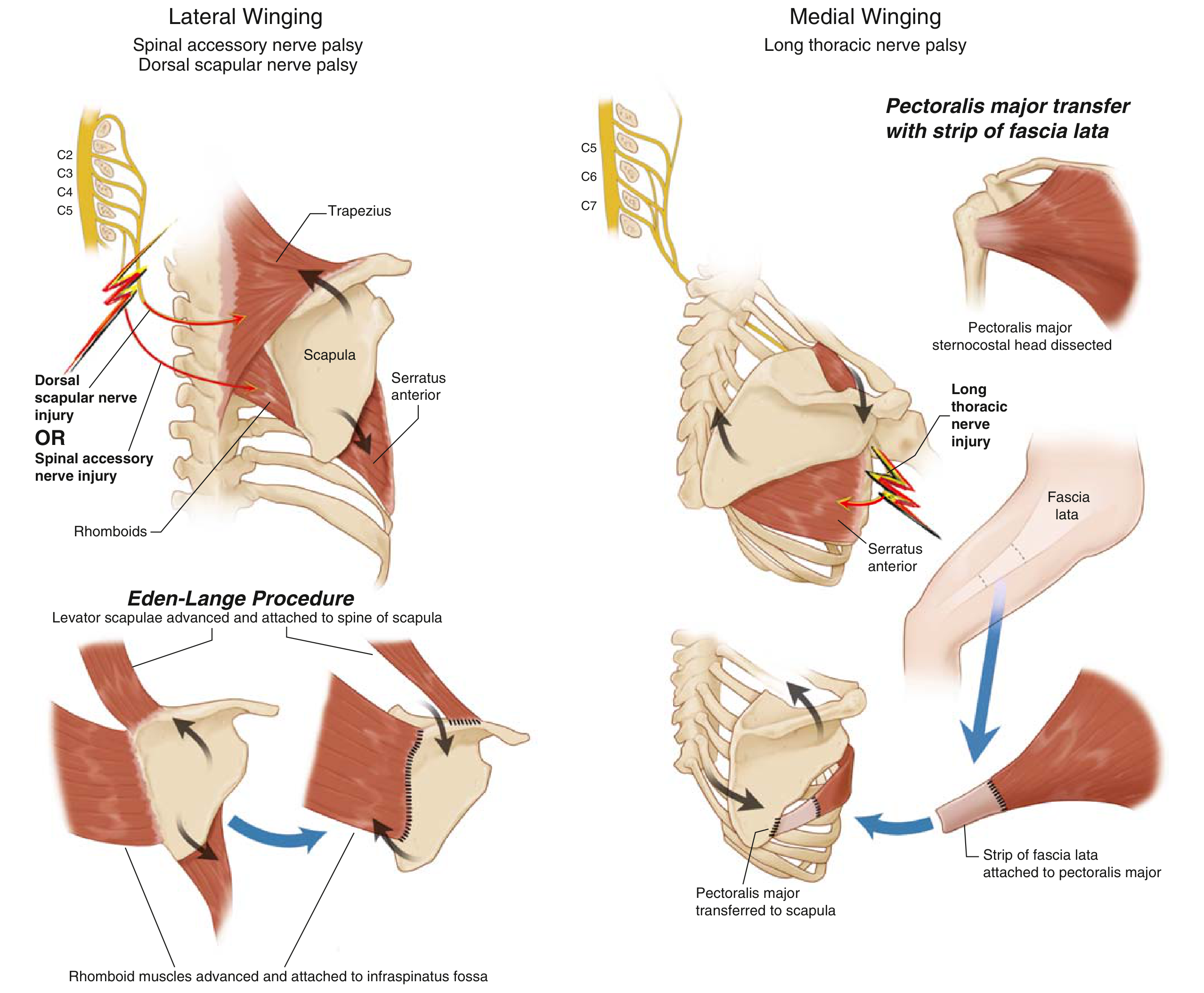
When conservative treatment fails over 12-24 months, surgical options include:
| Winging Type | Procedure | Details |
|---|---|---|
| Medial winging (long thoracic nerve palsy) | Pectoralis major transfer | Sternocostal head of pectoralis major transferred to the scapula, supplemented with a strip of fascia lata |
| Lateral winging (spinal accessory/dorsal scapular nerve palsy) | Eden-Lange procedure | Levator scapulae is advanced and attached to the spine of the scapula; rhomboid muscles are advanced to the infraspinatus fossa |
- Miller's Review of Orthopaedics, 9th Ed, p. 405
- Fischer's Mastery of Surgery, 8th Ed
Summary Mnemonics
SWIM - Serratus Winging is Inferior Medial (long thoracic nerve palsy = medial winging)
TRAWL - Trapezius and Rhomboids Are Winged Laterally (spinal accessory or dorsal scapular nerve palsy = lateral winging)
Key clinical pearl: Winging can occur from diverse causes - nerve injuries (long thoracic, spinal accessory, dorsal scapular), bony abnormalities (osteochondromas, fractures), muscle disease (facioscapulohumeral dystrophy), or even voluntarily. Differentiating medial from lateral winging by identifying the direction of the inferior angle movement guides both the diagnosis and treatment choice.
This is a shared conversation. Sign in to Orris to start your own chat.