Steven jhonson syndeome
Reading File
Finding Sources
Searching PubMed
"Stevens-Johnson syndrome"[MeSH Terms] AND management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have everything needed for a comprehensive, well-illustrated answer.
Stevens-Johnson Syndrome (SJS)
Overview and Classification
Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) represent a spectrum of the same disease - rare, acute, life-threatening mucocutaneous reactions that are nearly always drug-induced. They are classified by the extent of epidermal detachment:
| Category | Epidermal Detachment | Mortality |
|---|---|---|
| SJS | < 10% BSA | ~5% |
| SJS/TEN overlap | 10-30% BSA | ~19% |
| TEN (Lyell syndrome) | > 30% BSA | 15-25% |
(BSA = body surface area)
- Dermatology 2-Volume Set 5e, p. 412
- Goldman-Cecil Medicine, p. 4306
Epidemiology
- Incidence: 1.2-6 per million person-years (SJS); 0.4-1.2 per million (TEN)
- Female:male ratio ~ 1.5:1
- Over 95% of TEN cases and the majority of SJS cases are drug-induced
- HIV infection significantly increases risk (up to 1000-fold)
- Andrews' Diseases of the Skin, p. 342
Causative Drugs
More than 100 drugs have been implicated. The highest-risk drugs include:
Highest risk:
- Allopurinol - currently the most common cause in Europe
- Sulfonamides (TMP-SMX): 1-3 per 100,000
- Anticonvulsants: carbamazepine (14:100,000), lamotrigine (1:1,000 adults), phenytoin, phenobarbital, valproate
- Nevirapine (antiretroviral)
- NSAIDs (especially oxicam class)
Also implicated:
- Aminopenicillins, cephalosporins, quinolones, tetracyclines
- Fansidar (sulfadoxine/pyrimethamine): 10:100,000 - highest incidence of any drug
- Chlormezanone, acetaminophen (particularly in children)
The reaction typically begins 7-21 days after starting the causative drug. For anticonvulsants, risk is greatest during the first 2 months of treatment.
- Andrews' Diseases of the Skin, p. 342
- Goldman-Cecil Medicine, p. 4305
Pharmacogenetics / HLA Associations
Genetic susceptibility plays a major role, especially in specific ethnic groups:
| HLA Allele | Drug | Population |
|---|---|---|
| HLA-B*15:02 | Carbamazepine | Han Chinese, Thai, Malaysian, East Indian |
| HLA-B*15:02 | Lamotrigine | Taiwanese |
| HLA-B*15:02 | Phenytoin | Han Chinese |
| HLA-B*58:01 | Allopurinol | Han Chinese |
| HLA-A*31:01 | Carbamazepine | Europeans |
Clinical implication: HLA typing should be performed in all Asians before starting carbamazepine. The FDA recommends screening for HLA-B*15:02 in patients of Asian ancestry. HLA-B*15:02 is present in 4-15% of affected Asian populations but is extremely rare in Northern Europeans (<0.01%).
- Dermatology 2-Volume Set 5e, p. 412
Pathogenesis
The core mechanism is extensive keratinocyte apoptosis leading to full-thickness epidermal necrosis and separation at the dermal-epidermal junction.
Key mediators:
- Granulysin - a cytotoxic secretory protein released by CD8+ cytotoxic T lymphocytes and NK cells; this is now considered the primary mediator of keratinocyte killing
- Fas-FasL interaction - death receptor-ligand pair triggering apoptosis
- Drug-specific T-cell activation (pharmacogenetic interaction between drug/metabolite and HLA)
- TNF-alpha also contributes to keratinocyte death
The histology shows full-thickness epidermal cell death with a subepidermal split and a lymphohistiocytic infiltrate with eosinophils in the dermis.
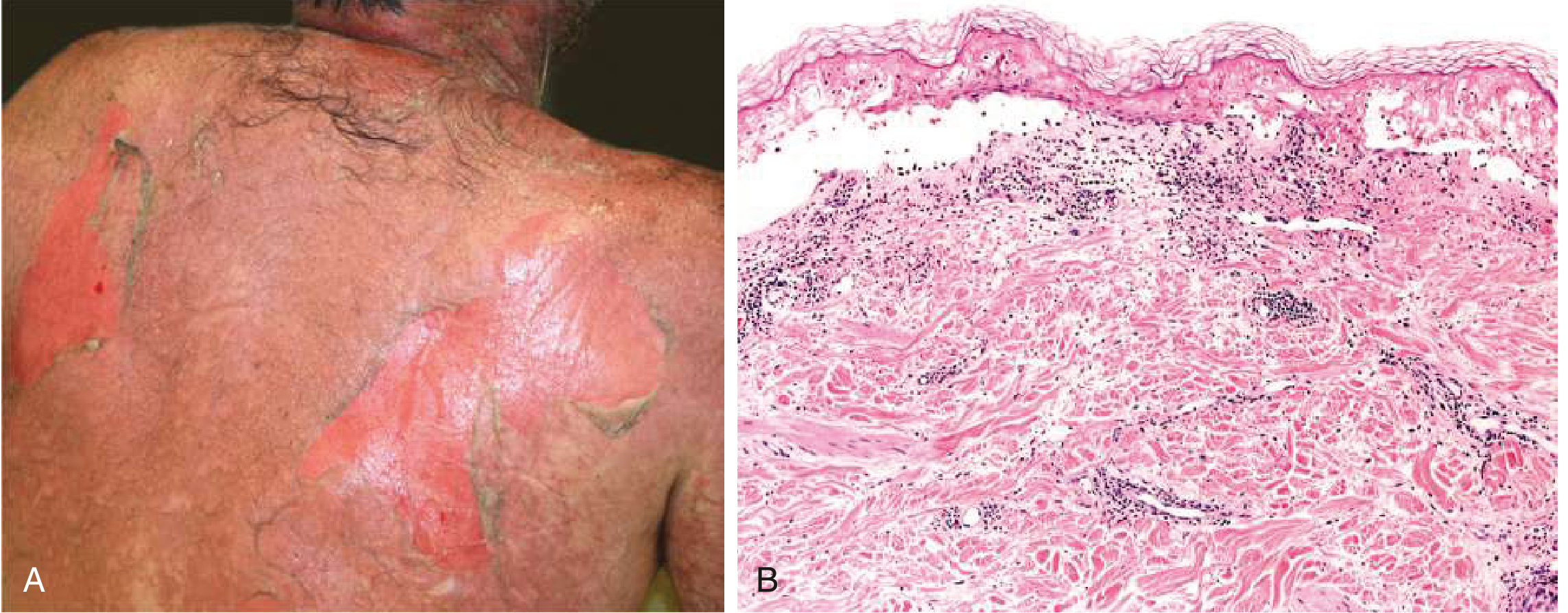
Figure: TEN showing denuded skin (A) and histology with full-thickness epidermal cell death and subepidermal separation (B). From Goldman-Cecil Medicine.
Clinical Features
Prodrome (1-3 days before skin lesions)
- Fever, malaise, sore throat
- Burning/painful eyes
- Painful skin - a key early warning sign
- Upper respiratory tract symptoms
Mucosal Involvement (almost always present)
- Oral/lip mucosa: erosions, hemorrhagic crusting, difficulty eating/swallowing
- Ocular: conjunctivitis, pseudomembrane formation, corneal erosions - can lead to permanent visual impairment
- Genital: erosions, urethritis
- Respiratory: bronchial epithelial sloughing (severe cases)
- Mucous membrane involvement typically precedes or accompanies skin changes
Skin Lesions
- Begin as erythematous macules on the trunk and face
- Evolve to flat, atypical target lesions (not the classic 3-ring targets of EM)
- Nikolsky sign positive: lateral pressure on erythematous skin causes epidermal detachment
- Asboe-Hansen sign: pressure on bullae causes lateral extension
- Blisters coalesce to form large areas of denuded skin
Distribution
- Starts on trunk, spreads to face and proximal extremities
- Palms/soles involved
- Acral surfaces > central in some cases
Systemic Involvement (severe cases/TEN)
- Pulmonary: bronchial sloughing, ARDS
- Hepatic involvement
- Renal impairment
- GI tract involvement
Diagnosis
Clinical diagnosis based on:
- Characteristic skin and mucosal lesions
- Positive Nikolsky sign
- History of drug exposure 7-21 days prior
- Skin biopsy: full-thickness necrosis, subepidermal blister
SCORTEN (Severity of Illness Score for TEN) - calculated at day 1 and day 3:
| Parameter | 1 point each if present |
|---|---|
| Age > 40 years | |
| Malignancy | |
| Heart rate > 120/min | |
| Initial BSA detachment > 10% | |
| BUN > 28 mg/dL (10 mmol/L) | |
| Serum bicarbonate < 20 mEq/L | |
| Serum glucose > 252 mg/dL (14 mmol/L) |
SCORTEN score 0-1 = ~3.2% mortality; score ≥5 = >90% mortality
ALDEN score helps establish causality (drug to SJS/TEN relationship).
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Staphylococcal scalded skin syndrome (SSSS) | Cleavage is subcorneal (not full thickness); occurs mainly in children; Gram+ staph exotoxin |
| Generalized bullous fixed drug eruption | No systemic involvement; marked hyperpigmentation; previous lesions at same site |
| Drug-induced linear IgA bullous dermatosis | IgA on DIF |
| Erythema multiforme (EM) | True 3-zone targets; acral distribution; usually HSV-triggered; no/minimal mucositis |
| AGEP | Pustular, not bullous; rapid resolution on drug withdrawal |
Management
1. Immediate - Stop the Causative Drug
This is the single most important intervention. Each additional day of continued drug use is associated with increased mortality. Drugs with short half-lives should be stopped first.
2. Supportive Care (mainstay of treatment)
- Transfer to a burn unit or specialized center - outcomes are significantly better
- Fluid and electrolyte replacement (treat like a burn patient)
- Temperature-controlled environment (patients cannot thermoregulate)
- Wound care: non-adhesive dressings, avoid debridement of intact blisters
- Nutritional support: early enteral feeding
- Ophthalmologic evaluation and care - daily, to prevent permanent sequelae (amniotic membrane transplant in acute phase)
- Pain management
- Infection surveillance and treatment (leading cause of death is sepsis)
3. Specific/Adjunctive Therapies
(No single therapy has definitive RCT evidence; options include:)
| Agent | Rationale/Use |
|---|---|
| TNF-alpha inhibitors (etanercept 50 mg SC x1-2 doses) | Blocks TNF-mediated keratinocyte apoptosis; observational data suggests benefit in TEN |
| Cyclosporine (3-5 mg/kg/day) | Inhibits T-cell activation and Fas-FasL pathway; most studied adjunctive agent |
| IVIg (1 g/kg/day x3 days) | May block Fas-FasL; may decrease fever duration; high doses may help |
| Corticosteroids (IV methylprednisolone 1-2 mg/kg or 60 mg q6h short course) | Controversial; may increase infection risk; some benefit in early disease |
- Goldman-Cecil Medicine, p. 4307
- Dermatology 2-Volume Set 5e, p. 413-414
Note: A 2024 systematic review on SJS/TEN from immune checkpoint inhibitors (PMID 39279714) highlights a growing subset of drug-induced cases from oncologic immunotherapy agents, requiring modified management approaches.
Sequelae / Complications
Ocular (most common long-term problem):
- Symblepharon, trichiasis, corneal scarring, dry eye syndrome, visual impairment/blindness
Skin:
- Post-inflammatory hyper/hypopigmentation
- Nail dystrophy or nail loss (anonychia)
- Scarring alopecia
Mucosal:
- Oral/esophageal strictures
- Phimosis, vaginal synechiae
- Bronchiolitis obliterans (rare but severe)
Psychological:
- PTSD, depression, significant reduction in quality of life
Key Points Summary
- SJS/TEN is a spectrum - classified by % BSA epidermal detachment (<10%, 10-30%, >30%)
- Almost always drug-induced in adults; onset 7-21 days after starting the drug
- Top culprits: allopurinol, sulfonamides, carbamazepine, lamotrigine, NSAIDs, nevirapine
- HLA screening (especially HLA-B*15:02) before carbamazepine in Asian patients is mandatory
- Pathogenesis: CD8+ T cell/NK cell-mediated keratinocyte apoptosis via granulysin and Fas-FasL
- Diagnosis: clinical + positive Nikolsky sign + skin biopsy
- SCORTEN predicts mortality
- Treatment: stop the drug immediately + burn unit care + supportive therapy; cyclosporine and etanercept are most promising adjunctive agents
- Ocular sequelae are the most common cause of long-term morbidity
Sources: Andrews' Diseases of the Skin, p. 340-345; Dermatology 2-Volume Set 5e, pp. 412-415; Goldman-Cecil Medicine, pp. 4305-4307; Fitzpatrick's Dermatology Vol 1-2, p. 783
Its effect on esophogus
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Searching PubMed
"Stevens-Johnson syndrome"[MeSH Terms] AND "esophagus"[MeSH Terms]
Searching PubMed
"Stevens-Johnson" AND esophageal
Reading Article
PMID: 39500588
Reading Article
PMID: 39280887
I now have comprehensive, multi-source data to write a focused, well-cited answer.
SJS/TEN: Effects on the Esophagus
The esophagus is the primary gastrointestinal organ affected in SJS/TEN, though involvement beyond the oropharynx is considered uncommon in SJS and more prominent in TEN.
Why the Esophagus Is Affected
The same immune-mediated mechanism driving skin destruction - CD8+ cytotoxic T-lymphocyte attack on epithelial cells - targets the squamous epithelium lining the esophagus. Since the esophagus (especially the upper two-thirds) is lined with non-keratinized stratified squamous epithelium, it is vulnerable to the same Fas-FasL and granulysin-mediated apoptosis that causes epidermal detachment in the skin.
- Yamada's Textbook of Gastroenterology, p. 2313
Acute Phase: Esophageal Manifestations
1. Esophagitis / Mucosal Inflammation
- The first and most common manifestation
- Ranges from mild esophagitis to diffuse ulceration and necrosis
2. Endoscopic Findings
At upper GI endoscopy, the esophagus may show:
- Diffuse erythema and friability
- Whitish plaques - can mimic candida esophagitis (important diagnostic pitfall)
- Necrotic plaques with mucosal sloughing
- Ulcerations along the esophageal mucosa
Biopsy differentiates SJS esophagitis from candidiasis: SJS shows lymphocytic infiltration and epithelial necrosis, not fungal hyphae.
3. Massive Gastrointestinal Bleeding
In severe cases, esophageal mucosal sloughing can lead to life-threatening hemorrhage. A 2024 case report (PMID 39500588) described a patient with SJS who developed massive GI bleeding with haemodynamic instability; endoscopy revealed necrotic plaques and mucosal sloughing throughout the esophagus requiring intensive care, multiple transfusions, and IV dexamethasone.
4. Oropharyngeal/Esophageal Pain
-
Severe oropharyngeal mucositis with erosions and mucosal sloughing
-
Odynophagia (painful swallowing) and dysphagia that may severely limit oral intake
-
Nutritional support (enteral or parenteral) is often required acutely
-
Sleisenger and Fordtran's GI and Liver Disease, p. 381
GI Involvement Beyond the Esophagus
While the esophagus bears the brunt of GI involvement, SJS/TEN can affect other parts of the gut:
| Site | Findings |
|---|---|
| Stomach / Duodenum | Diffuse erythema and friability (even without esophageal involvement) |
| Colon | Appearance resembles severe ulcerative colitis or pseudomembranous colitis; biopsy shows necrosis and lymphocytic infiltrate without crypt abscesses or neutrophils |
| Bowel (extensive TEN) | Mucosal sloughing of large bowel segments - can cause hematemesis, melena, and even intestinal perforation |
The colonic histology pattern resembles graft-versus-host disease - a key distinguishing feature from IBD.
- Sleisenger and Fordtran's GI and Liver Disease, p. 381
Chronic / Long-Term Sequelae
This is clinically important - esophageal complications can persist long after the acute disease resolves.
1. Esophageal Strictures and Webs
- Result from fibrosis and scarring following mucosal healing
- Can be single or multiple
- Cause progressive dysphagia weeks to months after the acute episode
- Esophageal dilation (endoscopic bougie or balloon) is often required for treatment
- Harrison's Principles of Internal Medicine 22E, p. 1872; Yamada's Textbook of Gastroenterology, p. 2313
2. Esophageal Epidermoid Metaplasia (EEM) - Newly Recognized
A 2024 pediatric case report (PMID 39280887) described the first case of esophageal epidermoid metaplasia developing in an 8-year-old girl after SJS with esophageal stricture. EEM is a rare condition in which the normal esophageal squamous epithelium undergoes keratinizing (epidermoid) metaplasia. This is significant because:
- EEM is associated with esophageal squamous cell carcinoma
- The authors recommend close surveillance, biopsy for dysplasia, endoscopic treatment, and TP53 genetic sequencing in pediatric SJS patients with esophageal involvement
Management of Esophageal Involvement
| Phase | Management |
|---|---|
| Acute | NPO or liquid diet; parenteral/enteral nutrition; IV fluids; treat GI bleeding with endoscopy if needed; IV corticosteroids (e.g., dexamethasone) for severe mucosal disease |
| Endoscopic | Upper GI endoscopy for diagnosis and to exclude candidiasis; avoid aggressive intervention on fragile mucosa acutely |
| Long-term | Surveillance for stricture development; serial endoscopic dilation for strictures; biopsy surveillance for dysplasia/metaplasia |
Key Takeaways
- The esophagus is the most commonly affected GI organ in SJS/TEN - other GI sites are rare but described
- Acute findings: esophagitis, diffuse erythema, whitish plaques (mimic candidiasis), mucosal sloughing, and rarely massive hemorrhage
- Colonic involvement histologically mimics GvHD (lymphocytic necrosis, no crypt abscesses)
- Long-term: esophageal strictures and webs requiring dilation are the primary sequela
- Newly recognized: esophageal epidermoid metaplasia post-SJS carries a risk of squamous cell carcinoma - surveillance is warranted
Sources: Yamada's Textbook of Gastroenterology 7e, p. 2313; Sleisenger and Fordtran's GI and Liver Disease, p. 381; Harrison's Principles of Internal Medicine 22E, p. 1872; PMID 39500588 (2024); PMID 39280887 (2024)
This is a shared conversation. Sign in to Orris to start your own chat.