Pleomorphic adenoman
Reading File
Finding Sources
Searching PubMed
"pleomorphic adenoma" salivary gland
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is a comprehensive overview of Pleomorphic Adenoma based on authoritative surgical and pathology textbooks.
Pleomorphic Adenoma (Benign Mixed Tumor)
Definition and Epidemiology
Pleomorphic adenoma (PSA) is the most common salivary gland neoplasm, accounting for approximately 50% of all salivary gland tumors, ~65% of parotid tumors, and ~40% of intraoral minor salivary gland tumors. The annual incidence is 2.4-3.05 per 100,000.
-
Age: Most common between the 3rd and 6th decades; average age 45 years
-
Sex: Slightly more frequent in women
-
Site distribution:
- Parotid gland: >80% of cases (most common site)
- Submandibular gland: less common
- Minor salivary glands: relatively rare; most common site within the oral cavity is the hard palate
-
Robbins & Kumar Pathologic Basis of Disease, p. 697
-
Bailey and Love's Short Practice of Surgery 28th Edition, p. 861
Pathogenesis / Molecular Biology
Little is definitively known about the origin, but current understanding includes:
-
All tumor elements (including those appearing mesenchymal) are thought to derive from myoepithelial or ductal reserve (stem) cells
-
Radiation exposure increases risk
-
Most cases involve chromosomal rearrangements causing overexpression of PLAG1, a transcription factor that promotes cell growth via growth factor receptor signaling pathways
-
Cases lacking PLAG1 overexpression are often associated with HMGA2 gene mutations (encodes a DNA-binding protein)
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 697
Clinical Features
- Painless, slow-growing, mobile, well-defined solitary mass
- Gradual progression over many years; can reach enormous proportions if left untreated
- Usually located in the parotid tail (superficial lobe)
- Deep lobe tumors may present as a paratonsillar bulge
- No facial nerve involvement in benign disease
Warning signs of malignant transformation:
- Sudden increase in size
- Facial nerve palsy
- Pain
Gross Pathology
- Well-demarcated, rounded/ovoid mass, rarely exceeding 6 cm
- Broad-based surface bosselations
- Cut surface: gray-white with myxoid and blue translucent areas of chondroid (cartilage-like) stroma
- Capsule is variable: may be thick and fibrotic, attenuated, or even incomplete (especially on the palate)
- Peri-capsular nodules may be present, attached by slender pedicles - simple enucleation risks detaching these, creating foci for recurrence
- Predominantly myxoid tumors can rupture during surgery, seeding the field and causing multifocal recurrences
Histopathology
The hallmark is morphologic heterogeneity (not true nuclear pleomorphism). Key features:
| Component | Description |
|---|---|
| Ductal/epithelial cells | Form ducts, acini, tubules, strands, or sheets; cuboidal to columnar cells |
| Myoepithelial cells | Deeply chromatic, small cells underlying the ducts; can be spindle, plasmacytoid, or clear |
| Stroma | Chondromyxoid matrix - loose myxoid, hyaline tissue; islands of cartilage; rarely bone |
No significant epithelial dysplasia or mitotic activity in benign cases.
Immunohistochemistry:
- Luminal cells: CK7 (strong and diffuse)
- Myoepithelial cells: p63, S-100, SOX10, SMA
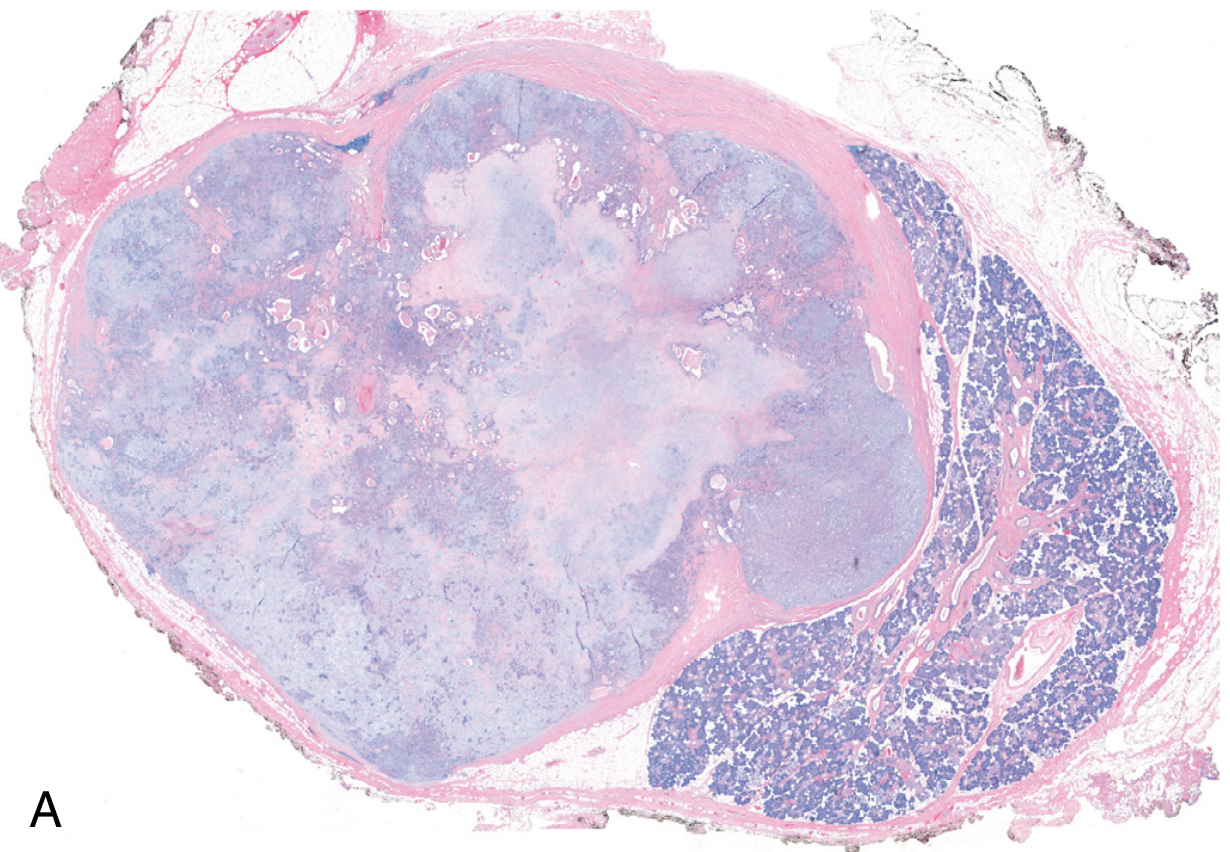
Low-power histology (H&E): Well-circumscribed tumor with a fibrous capsule and adjacent normal salivary gland parenchyma:
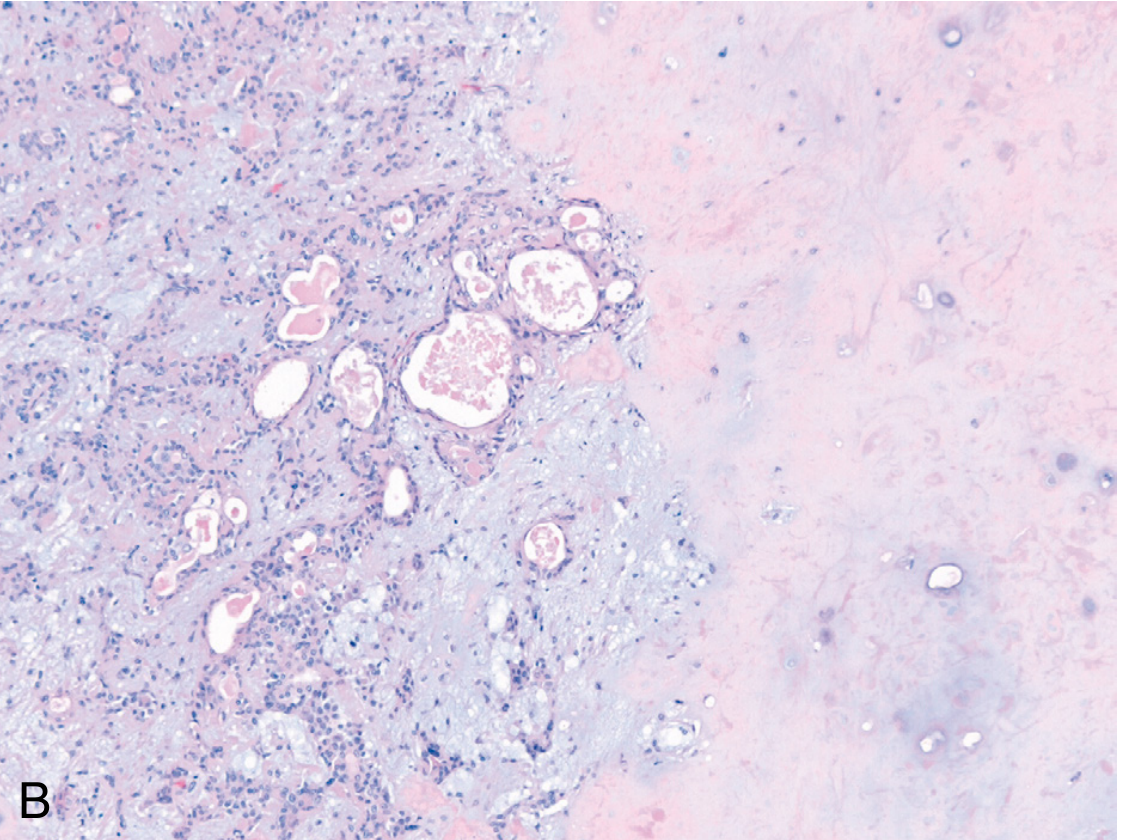
High-power histology showing ductal structures in a chondromyxoid matrix:
Recurrence
| Treatment | Recurrence Rate |
|---|---|
| Simple enucleation | ~25% |
| Parotidectomy (formal resection with cuff) | ~4% |
Recurrence is usually multifocal when it occurs, especially if capsule rupture with tumor spillage occurred at first surgery. Recurrence risk is also increased by predominantly myxoid tumors and tumors with pericapsular pseudopodal extensions.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 697
Malignant Transformation - Carcinoma ex Pleomorphic Adenoma
Overall risk of malignant change: ~6%
| Duration of Lesion | Malignant Transformation Risk |
|---|---|
| < 5 years | ~2% |
| > 15 years | ~10% |
Clinical risk factors for transformation:
- Older patient age
- Male sex
- Long duration of the tumor
- Multiple recurrences
- Deep lobe parotid location
Resulting carcinomas are typically adenocarcinomas or undifferentiated carcinomas. They are highly infiltrative and carry 30-50% mortality at 5 years - among the most aggressive salivary gland cancers.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 697
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Treatment
- Standard: Superficial or total parotidectomy with a cuff of normal tissue around the tumor to include the pseudopods
- Enucleation alone is contraindicated due to high recurrence risk from pericapsular extensions
- Minor salivary gland (oral cavity) tumors: Complete transoral excision; recurrences are rare with complete excision due to encapsulation
- CO2 laser is also used as a cutting tool for intraoral lesions
A 2025 meta-analysis (Salzano et al., 2025) directly compared extracapsular dissection vs. superficial parotidectomy, providing updated evidence on the optimal surgical approach for parotid pleomorphic adenoma.
Summary Table
| Feature | Details |
|---|---|
| Most common type | Most common salivary gland tumor overall |
| Most common site | Parotid gland (>80%) |
| Cell of origin | Myoepithelial / ductal reserve stem cells |
| Molecular markers | PLAG1 overexpression, HMGA2 mutations |
| Presentation | Painless, slow-growing, mobile mass |
| Histology | Epithelial + myoepithelial cells in chondromyxoid stroma |
| IHC | CK7 (luminal), p63/S-100/SOX10/SMA (myoepithelial) |
| Recurrence (enucleation) | ~25% |
| Recurrence (parotidectomy) | ~4% |
| Malignant transformation | ~6% overall; up to 10% after 15 years |
| Treatment | Surgical excision with normal tissue cuff |
Clinical examination of pleomorphic adenoma
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
Here is a detailed, structured account of the clinical examination of pleomorphic adenoma, organized the way a surgical examination would proceed in practice.
Clinical Examination of Pleomorphic Adenoma
1. History (Pre-Examination Clues)
Before examining the patient, key history points direct your focus:
| Feature | Expected in PSA |
|---|---|
| Duration | Months to years - very slow growth |
| Pain | Absent (painless swelling) |
| Rate of change | Gradual |
| Facial nerve symptoms | Absent (palsy = red flag for malignancy) |
| Sudden enlargement | Absent (sudden increase = malignant change alarm) |
| Age/sex | 3rd-6th decade; slightly commoner in women |
2. Inspection
Position of the Swelling
The most common site is the parotid tail (below and in front of the ear, just above the angle of the mandible). Systematically assess:
- Parotid region: Fullness below and anterior to the ear, lifting the ear lobe - the classic sign that the swelling arises from the parotid gland
- Overlying skin: Normal in color and texture; no ulceration, fixation, or redness (these suggest malignancy)
- Facial symmetry: Check for any distortion of the face or obvious asymmetry
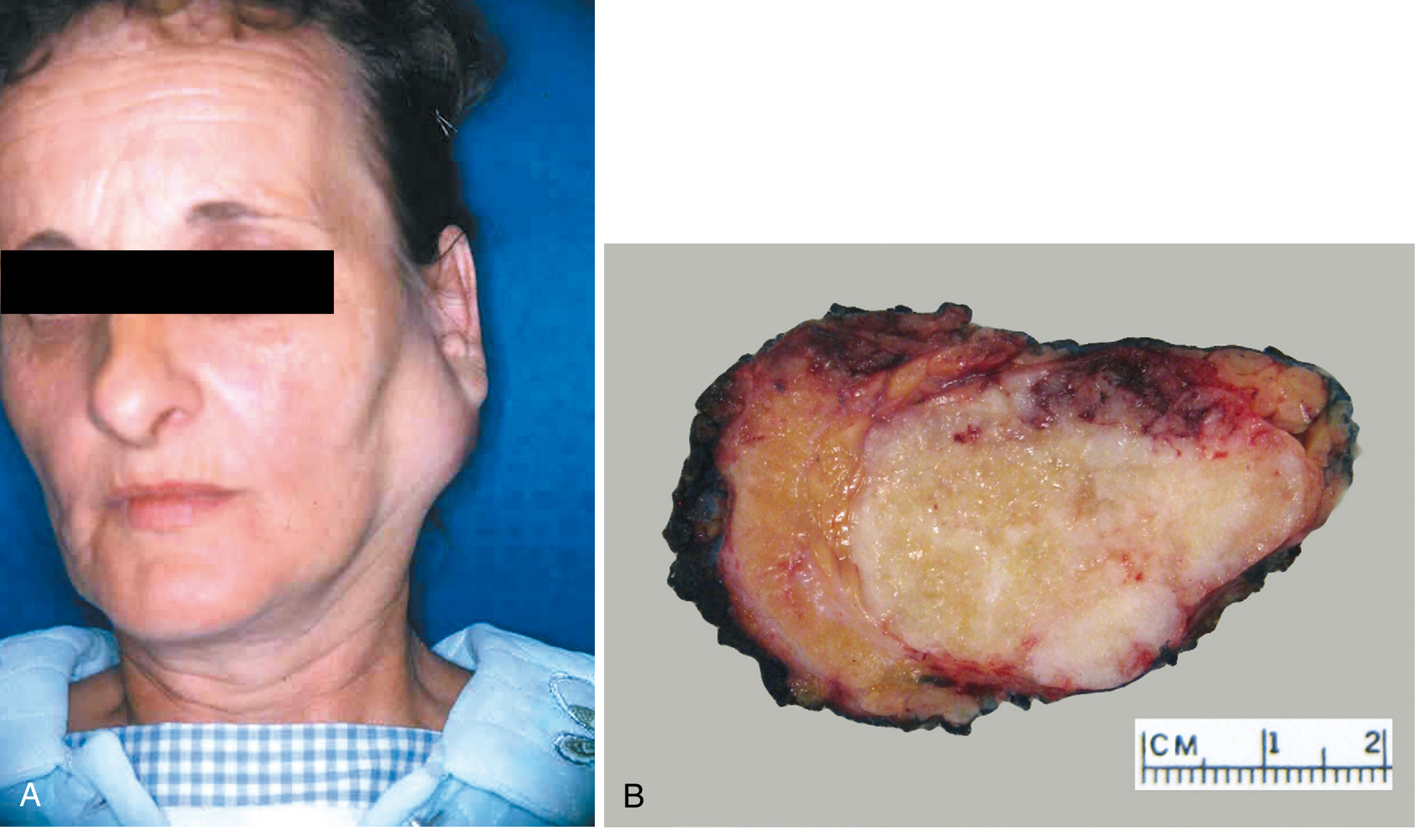
Clinical photograph - parotid pleomorphic adenoma:
Specific Inspection Points
- Earlobe sign: The ear lobe is elevated/pushed outward by the swelling - pathognomonic of parotid origin
- Trismus: Absent in benign PSA (deep lobe tumors can impair jaw opening if very large)
- Open-mouth inspection: Deep lobe tumors may present as a paratonsillar or soft palate bulge (visible only with mouth open)
- Accessory parotid tissue tumors: Only visible when the patient opens the mouth (coronoid process pushes tumor outward)
- Minor salivary gland (palate/buccal mucosa): Smooth, sessile, submucosal swelling - most commonly on the hard palate
Bailey and Love's Short Practice of Surgery, p. 861
3. Palpation
This is the most informative part of the examination.
Characteristics on Palpation
| Feature | Typical Findings in PSA |
|---|---|
| Temperature | Normal (not warm) |
| Tenderness | Non-tender |
| Size | Variable; usually 2-5 cm at presentation |
| Shape | Round/ovoid with smooth or bosselated surface |
| Surface | Smooth, sometimes lobulated/bosselated |
| Consistency | Variable - soft (myxoid-dominant) to firm/hard (chondroid/collagenous-dominant); most are firm-rubbery |
| Margins | Well-defined, clearly demarcated |
| Mobility | Mobile in all directions (not fixed to skin or deep structures) |
| Skin over swelling | Freely mobile over the swelling - not tethered |
| Fluctuance | Usually absent (myxoid types may feel fluctuant) |
The firmness varies directly with the stromal composition - myxoid tumors feel soft and may even appear fluctuant, while those with extensive chondroid or collagenous components feel hard. This is a key examination finding.
Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 2
Bimanual Palpation (for deep lobe / paratonsillar extension)
- One finger intraorally against the tonsil/soft palate, other hand externally over the parotid region
- A deep lobe PSA will be felt between both fingers as a firm mass in the parapharyngeal space
- Important to distinguish from a primary parapharyngeal tumor
Palpation of the Oral Cavity (Minor Salivary Gland PSA)
- Smooth, firm, non-tender, submucosal swelling
- Most common on the hard palate - typically posterior and lateral
- Freely movable in early stages; may be fixed to palate mucosa (does NOT imply malignancy - simply related to location)
4. Facial Nerve Assessment (Critical)
Always formally test the facial nerve (CN VII) in any parotid swelling. In benign PSA:
| Branch | Test | Expected Result in PSA |
|---|---|---|
| Temporal | Raise eyebrows | Normal |
| Zygomatic | Close eyes tightly | Normal |
| Buccal | Smile, show teeth | Normal |
| Marginal mandibular | Depress lower lip | Normal |
| Cervical | Neck platysma | Normal |
Facial nerve palsy = red flag for malignant transformation or malignant tumor. Any branch involvement demands urgent re-evaluation.
5. Regional Lymph Nodes
- Palpate the parotid/periparotid nodes, upper deep cervical chain, and jugulodigastric nodes
- In benign PSA: no palpable lymphadenopathy
- Lymphadenopathy suggests malignancy (carcinoma ex PSA) or a different primary diagnosis altogether
6. Intraoral Examination
- Open mouth widely - look for paratonsillar bulge (deep lobe PSA)
- Inspect the Stensen's duct orifice (opposite upper 2nd molar): secretions should be clear; turbid/purulent discharge suggests infection not tumor
- Bimanually palpate submandibular and sublingual glands if the swelling is in that territory
7. Complete Head and Neck Examination
- Contralateral parotid: Check for bilateral disease (rare in PSA; common in Warthin's)
- Submandibular glands: PSA can arise here; bimanual palpation required
- Skin: Any skin changes, fistulae, or previous scars
8. Examination Summary: Classic PSA vs. Red Flags
| Feature | Benign PSA (Expected) | Red Flag (Malignant Change) |
|---|---|---|
| Pain | Absent | Present |
| Facial nerve | Intact | Palsy |
| Growth | Slow, years | Rapid acceleration |
| Skin | Normal, free | Fixed, ulcerated |
| Consistency | Firm, rubbery | Hard, stony |
| Mobility | Mobile | Fixed/tethered |
| Lymph nodes | Not palpable | Enlarged |
| Trismus | Absent | May be present |
Bailey and Love's Short Practice of Surgery, p. 861; Scott-Brown's Otorhinolaryngology Head & Neck Surgery
9. Special Notes
- Calcification on imaging (CT/USS): presence of calcification within a parotid or parapharyngeal mass strongly suggests pleomorphic adenoma - no other salivary tumor calcifies in this way
- Submandibular PSA: Must bimanually palpate; risk of marginal mandibular nerve injury at surgery is higher here
- Accessory parotid PSA: Felt as a mass along the line of Stensen's duct, anterior to the main gland; only moves forward when the patient opens the mouth (coronoid displacement)
Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 2, p. 162
Clinical examination of pleomorphic adenoma
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Here is a complete, step-by-step account of the clinical examination of pleomorphic adenoma, structured as it would be conducted at the bedside or in an OSCE setting.
Clinical Examination of Pleomorphic Adenoma
Step 1: General Observation (From the End of the Bed)
Before touching the patient, stand back and observe:
- A visible swelling in the pre-auricular/parotid region, below the ear, pushing the ear lobe upward and outward
- No obvious facial asymmetry from nerve weakness
- Patient typically appears comfortable and in no distress (painless condition)
- Assess whether the swelling is unilateral or bilateral
Step 2: History Points that Guide Examination
| Question | Expected Answer in PSA |
|---|---|
| How long has it been there? | Months to many years - very slow growth |
| Is it painful? | No - painless |
| Any facial weakness? | No - facial nerve intact |
| Any sudden recent increase in size? | No (if yes - alarm for malignant transformation) |
| Any difficulty opening mouth / swallowing? | Usually no (deep lobe may cause dysphagia) |
Step 3: Inspection
Site and Extent
The parotid region is the most common location (>80% of cases). Inspect systematically:
For parotid PSA:
- Swelling below and in front of the ear, at the parotid tail
- The ear lobe is elevated and pushed outward - this is pathognomonic of parotid origin
- The swelling fills the space between the mastoid process posteriorly and the ramus of mandible anteriorly
- Lower border may extend toward the upper neck
Pre-auricular swelling in PSA with surgical markings:

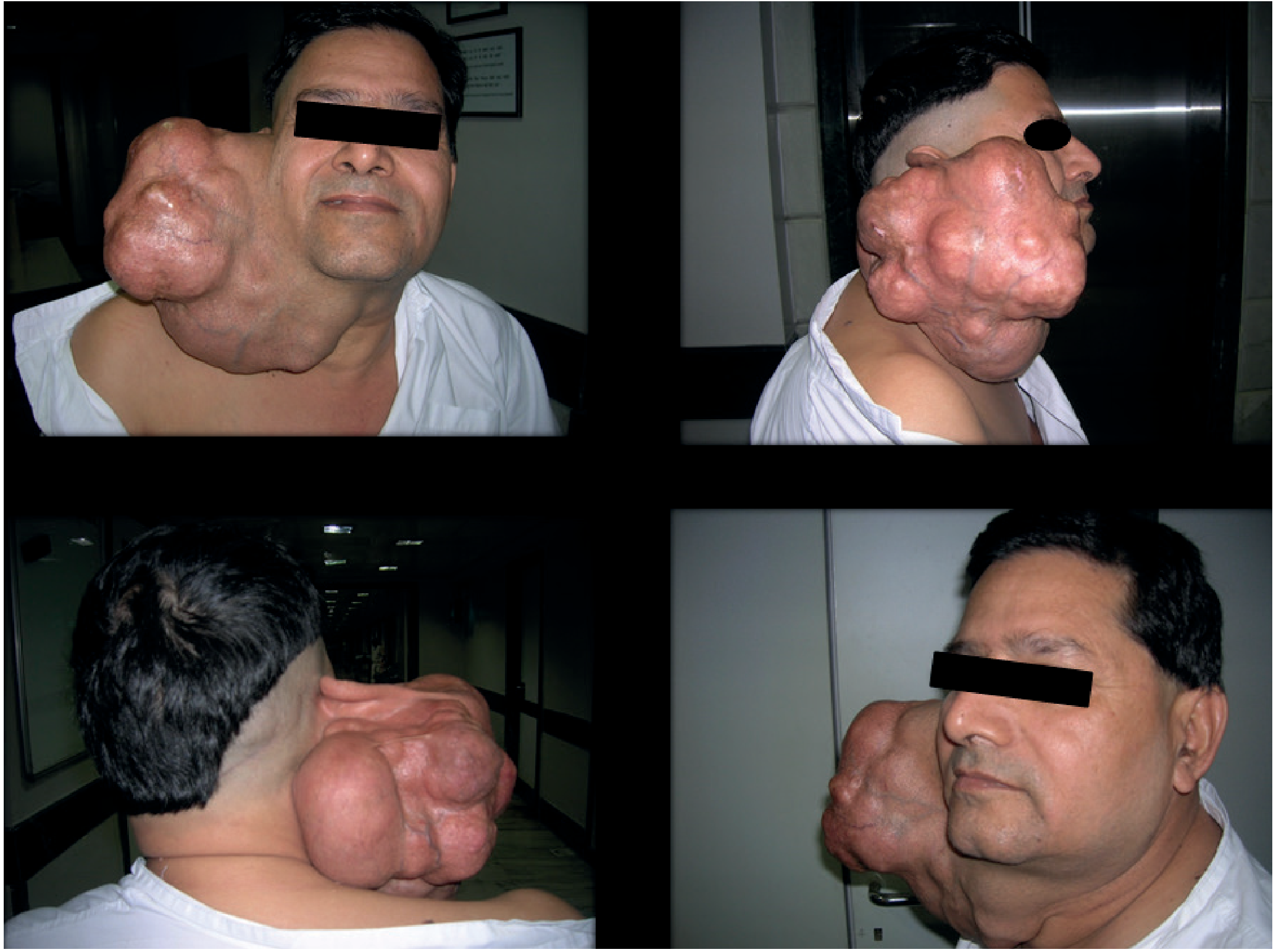
Gross neglected PSA (untreated for 15 years):
What to Note on Inspection
| Feature | Expected Finding |
|---|---|
| Skin color | Normal - no erythema, no discoloration |
| Skin surface | Smooth, no ulceration, no peau d'orange |
| Skin fixation | Skin moves freely over the swelling |
| Shape | Smooth, rounded, or lobulated contour |
| Scars | Check for previous surgery (recurrent PSA) |
| Facial symmetry | Symmetrical - no drooping, no lagophthalmos |
| Mouth opening | Ask patient to open mouth widely - look for paratonsillar/soft palate bulge (deep lobe tumor) |
Important: Ask the patient to open their mouth. If the tumor arises from accessory parotid tissue along Stensen's duct, it may only become visible or more prominent when the coronoid process moves forward - pushing the tumor outward.
Step 4: Palpation
This is the most informative part of the examination.
Approach
- Warm hands
- Stand to the side and slightly behind the patient
- Use both hands to compare both sides
- Always palpate gently first
Characteristics to Elicit
| Feature | Method | Expected Finding in PSA |
|---|---|---|
| Temperature | Dorsum of examining hand | Normal - not warm |
| Tenderness | Gentle pressure | Non-tender |
| Size | Measure in two dimensions | Usually 2-5 cm; can be larger if long-standing |
| Shape | Trace margins | Round or ovoid |
| Surface | Roll fingers over swelling | Smooth or bosselated (lobulated) |
| Consistency | Compress gently | Firm-rubbery typically; soft if myxoid-dominant; hard if chondroid-dominant |
| Margins | Edge of swelling | Well-defined, clearly demarcated |
| Mobility | Move in horizontal and vertical planes | Mobile in all directions - not fixed to skin or deep tissues |
| Skin fixation | Pinch skin over the swelling | Skin moves freely - not tethered |
| Deep fixation | Ask patient to clench teeth (masseter contracts, fixes parotid tissue) | Normal parotid tissue fixes; PSA should become less mobile on clenching if within the gland |
| Fluctuance | Two-finger test | Usually absent; myxoid tumors may appear fluctuant |
| Transillumination | If fluctuant | Negative (solid tumor) |
| Pulsatility | Feel for expansile pulsation | Absent |
Key clinical point on consistency:
The firmness varies directly with the stromal composition - soft in myxoid-dominant tumors, hard in tumors with extensive chondroid or collagenous stroma. This variation in consistency on palpation is itself a characteristic feature of PSA.
Scott-Brown's Otorhinolaryngology Head & Neck Surgery, p. 162
Step 5: Facial Nerve Assessment (MANDATORY in All Parotid Swellings)
Formally test all 5 branches of the facial nerve (CN VII). Record findings for each:
| Branch | Test | Expected in Benign PSA |
|---|---|---|
| Temporal | "Raise your eyebrows" | Normal - wrinkles symmetrical |
| Zygomatic | "Close your eyes tightly" | Normal - eyes close fully and symmetrically |
| Buccal | "Smile and show me your teeth" / "Puff out your cheeks" | Normal - symmetrical |
| Marginal mandibular | "Pull down your lower lip" | Normal - symmetrical |
| Cervical | "Tighten your neck muscles" / platysma contraction | Normal |
Any facial nerve palsy = red flag. In benign PSA, the facial nerve is ALWAYS intact. Facial palsy strongly indicates malignancy - either carcinoma ex pleomorphic adenoma or a primary malignant tumor.
Bailey and Love's Short Practice of Surgery, p. 861
Step 6: Intraoral Examination
Always examine inside the mouth for every parotid or salivary gland swelling.
Parotid Assessment Intraorally
-
Stensen's duct orifice - opposite the upper 2nd molar tooth (parotid papilla):
- Massage the gland from behind forward
- Clear saliva should flow freely = normal
- Turbid or purulent discharge = sialadenitis/sialadenosis (not PSA)
-
Paratonsillar bulge - ask patient to open wide and say "Aah":
- A deep lobe PSA pushing through the stylomandibular tunnel presents as a medially displaced tonsil or bulging of the soft palate/lateral pharyngeal wall
- This is the "dumbbell tumor" - one lobe palpable externally, one palpable intraorally
Minor Salivary Gland PSA (Hard Palate)
Most commonly found on the posterior-lateral hard palate:
- Smooth, firm, dome-shaped submucosal swelling
- Mucosa over it is intact and normal-colored
- Non-tender, non-pulsatile
- Slowly enlarging over months-years
Minor salivary gland PSA on the hard palate:

Step 7: Bimanual Palpation (for Deep Lobe / Parapharyngeal Extension)
For suspected deep lobe involvement:
- Place one finger intraorally against the tonsil/lateral pharyngeal wall
- Place the other hand externally over the parotid
- A deep lobe extension or dumbbell tumor will be felt compressible between both fingers
- Always examine both sides for comparison
Step 8: Regional Lymph Node Examination
Systematically palpate all cervical lymph node groups:
| Group | Method |
|---|---|
| Parotid/preauricular nodes | In front of tragus |
| Periparotid nodes | Over the parotid gland itself |
| Jugulodigastric (Level II) | Below and anterior to the ear at the angle of mandible |
| Upper, mid, lower deep cervical chain | Along the sternocleidomastoid |
| Posterior triangle | Behind SCM |
| Submental / submandibular | Below the chin / under the mandible |
Expected finding in benign PSA: No palpable lymphadenopathy
Lymphadenopathy = red flag for malignancy or metastatic disease
Step 9: Examination of Other Salivary Glands
Always check the remaining salivary glands:
- Contralateral parotid: Usually normal; bilateral parotid swelling is characteristic of Warthin's tumor or systemic disease (sarcoidosis, Sjögren's), not PSA
- Submandibular glands: Bimanually palpate (one finger under chin externally, one finger on floor of mouth intraorally) - PSA can arise here
- Sublingual glands: Inspect and palpate intraorally
Step 10: Summary - Benign PSA vs. Malignancy Alarm Signs
| Feature | Benign PSA | Red Flag (Malignant) |
|---|---|---|
| Pain | Absent | Present |
| Facial nerve | Fully intact | Any palsy |
| Growth rate | Slow (years) | Rapid acceleration |
| Skin | Normal, free | Fixed, ulcerated |
| Consistency | Soft-firm-rubbery | Hard, stony |
| Mobility | Mobile | Fixed to skin or deep |
| Lymph nodes | Not palpable | Enlarged |
| Trismus | Absent | May be present |
| Duct secretion | Clear saliva | Unchanged / blood-stained |
Complete Examination Summary (OSCE-Style)
"This patient has a painless, slow-growing, well-defined, firm, mobile, bosselated swelling in the right parotid region measuring approximately [X] cm. The overlying skin is normal and freely mobile. The ear lobe is elevated. There is no facial nerve weakness on formal cranial nerve testing. Intraorally, the right Stensen's duct orifice is producing clear saliva; there is no paratonsillar bulge. Regional lymph nodes are not palpable. These findings are consistent with a pleomorphic adenoma of the right parotid gland."
- Bailey and Love's Short Practice of Surgery 28th Edition, p. 861
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, p. 162
- Cummings Otolaryngology Head and Neck Surgery, p. 1647
Clinical examination of hydrocele
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Here is a complete, step-by-step account of the clinical examination of hydrocele, structured as it would be conducted at the bedside or in an OSCE setting.
Clinical Examination of Hydrocele
Definition
A hydrocele is an abnormal collection of serous fluid within the tunica vaginalis around the testis (or occasionally along the spermatic cord). It is the most common cause of a painless scrotal swelling.
Bailey and Love's Short Practice of Surgery 28th Edition, p. 1586
Types - Anatomical Classification
Understanding the types is essential before examining, as each has distinct clinical findings:
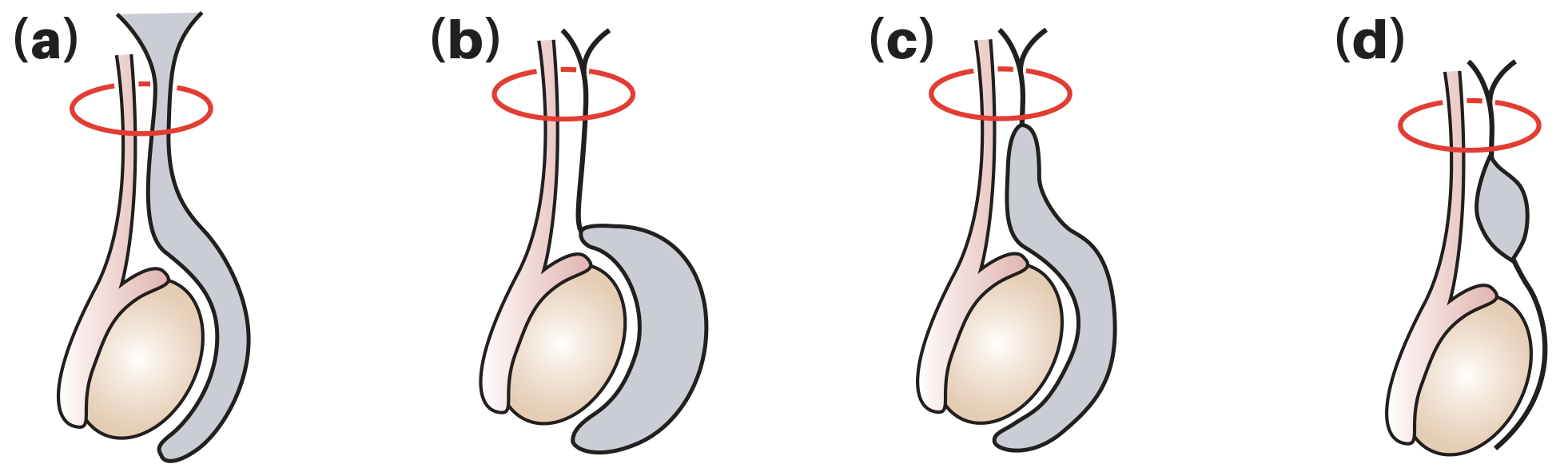
| Type | Key Feature | Clinical Clue |
|---|---|---|
| Vaginal (non-communicating) | Most common; fluid within tunica vaginalis only | Can get above it; testis impalpable within it |
| Congenital (communicating) | Patent processus vaginalis; communicates with peritoneum | May reduce when lying down; may vary in size |
| Infantile | Extends up into inguinal canal but processus closed proximally | Cord cannot be felt separately above swelling |
| Hydrocele of the cord | Isolated mid-cord cyst | Oval swelling above testis; moves down when testis pulled |
Step 1: General Inspection
- Patient examined in both standing and supine positions - mandatory
- Note which side is affected (unilateral or bilateral)
- Assess the overall scrotal appearance before touching
On Inspection
| Feature | Expected in Hydrocele |
|---|---|
| Position | Hangs lower than normal; scrotum appears enlarged on affected side |
| Shape | Rounded, smooth, pear-shaped or globular swelling |
| Skin | Normal color and texture; no erythema, no edema, no peau d'orange |
| Overlying skin | Freely mobile over the swelling |
| Scrotal folds | May be obliterated / stretched by large hydrocele |
| Penile position | May be buried/obscured by a very large hydrocele |
Step 2: The Three Key Clinical Questions
Always systematically answer these three questions during examination:
Question 1: Can you GET ABOVE the swelling?
- Place two fingers at the neck of the scrotum, just below the external inguinal ring
- Attempt to pinch and feel a normal spermatic cord above the upper limit of the swelling
| Finding | Interpretation |
|---|---|
| Can get above it (cord palpable separately above) | Swelling confined to scrotum - consistent with hydrocele |
| Cannot get above it (swelling continuous with inguinal canal) | Swelling extends into inguinal canal - suggests inguinal hernia descending into scrotum |
This is the single most important initial distinction in scrotal examination.
Bailey and Love's Short Practice of Surgery, p. 1586
Question 2: Is the testis/epididymis separately palpable?
- Attempt to feel the testis and epididymis separately within/around the swelling
| Finding | Interpretation |
|---|---|
| Testis and epididymis IMPALPABLE (enclosed within the swelling) | Classic hydrocele - fluid surrounds the testis completely |
| Testis palpable separately beside the swelling | Epididymal cyst or paratesticular swelling |
Question 3: Does the swelling transilluminate?
- In a dark room, press a torch/penlight firmly against one side of the swelling
- Look from the other side
| Finding | Interpretation |
|---|---|
| Bright red/pink transillumination (light transmits freely) | Hydrocele - thin-walled sac filled with clear serous fluid |
| Does NOT transilluminate | Solid swelling (tumor, haematocele) or thick-walled sac (longstanding hydrocele, filarial) |
Hydroceles transilluminate brightly. This is the clinical hallmark of a fluid-filled scrotal swelling.
Bailey and Love, Summary Box 86.5, p. 1587
Step 3: Palpation
Technique
- Warm hands; hold scrotum gently with non-dominant hand
- Use dominant hand to systematically palpate all scrotal contents
- Compare both sides
Characteristics to Elicit
| Feature | Expected Finding in Hydrocele |
|---|---|
| Temperature | Normal - not warm (warmth = epididymo-orchitis) |
| Tenderness | Non-tender (painless swelling) |
| Size | Variable; can be small to very large |
| Shape | Smooth, globular or pear-shaped |
| Surface | Smooth |
| Consistency | Fluctuant - fluid-filled; tense in large hydroceles |
| Margins | Well-defined upper border (can get above it in vaginal type) |
| Mobility | Moderately mobile within scrotum |
| Testis | Usually impalpable (surrounded by fluid); felt posteriorly in some cases |
| Reducibility | Non-reducible (distinguishes from hernia) |
Testing for Fluctuance
- Place index and middle fingers of one hand on opposite poles of the swelling
- Flick with the other hand - impulse transmitted in all directions = fluctuant = fluid-filled
Testing for Reducibility
- Attempt to compress or reduce the swelling upward
- A hydrocele is NOT reducible (in contrast to a hernia)
- Exception: A congenital/communicating hydrocele may partially reduce when the child lies down (fluid drains back into peritoneal cavity via patent processus)
Step 4: Special Tests
Transillumination (Confirmatory Test)
This is the most important special test:
- Darken the room
- Apply a strong torch/penlight to the posterior surface of the scrotal swelling
- Observe from in front
Positive (hydrocele): The swelling glows bright red-orange throughout - the light passes freely through the clear serous fluid
Negative: No glow - suggests solid swelling (tumor, haematocele) or turbid/thick fluid (chylocele, infected hydrocele)
Important caveat: A large, tense hydrocele may not transilluminate well if the walls have become thickened. An ultrasound is invaluable in this situation.
Cough Impulse
- Ask patient to cough while you feel the swelling
- Hydrocele: No cough impulse (sac is isolated from peritoneal cavity in acquired type)
- Communicating hydrocele / hernia: Positive cough impulse
Step 5: Specific Features by Type
Vaginal (Primary) Hydrocele
- Most common type; middle-aged to older men
- Painless, globular, smooth scrotal swelling
- Can get above it
- Testis impalpable (enclosed)
- Positive transillumination
- Non-tender, non-reducible
- May reach large size before patient presents
Congenital (Communicating) Hydrocele
- Infants/young children; history of intermittent or variable swelling
- Swelling may be smaller in the morning (fluid drained back overnight in recumbent position)
- Pressure on swelling may not fully empty it (communication too small)
- Check for bilateral swelling - if bilateral, rule out ascites
- Usually no hernia (communication too small to allow herniation of bowel)
Hydrocele of the Cord
- Oval, smooth swelling above the testis along the cord
- Separate from testis (testis palpable below it)
- Key sign: moves downward and becomes less mobile when the testis is pulled gently downward (the cord tethers it)
- May be mistaken for an inguinal hernia
- Transilluminates brightly
Secondary Hydrocele
- In a young man, an acutely presenting hydrocele raises suspicion of underlying testicular tumor - do NOT aspirate (risk of malignant needle-track implantation)
- May also occur secondary to infection (epididymo-orchitis), trauma, torsion, or post-radiotherapy
- The secondary cause may be detectable on careful palpation (thickened/tender epididymis, irregular testis)
Bailey and Love, p. 1587
Step 6: Complete the Examination
Examine Both Sides
- Compare both testes in size, consistency, and position
- Feel for epididymis posterolaterally to each testis
Examine the Inguinal Regions
- Check for evidence of a hernia or lymphadenopathy bilaterally
- Palpate the inguinal canal for any direct or indirect hernia
Examine the Abdomen
- Particularly important in bilateral hydroceles in children (rule out ascites)
- In adults with secondary hydrocele: examine for abdominal lymphadenopathy or retroperitoneal mass (testicular tumor metastasizes to para-aortic nodes)
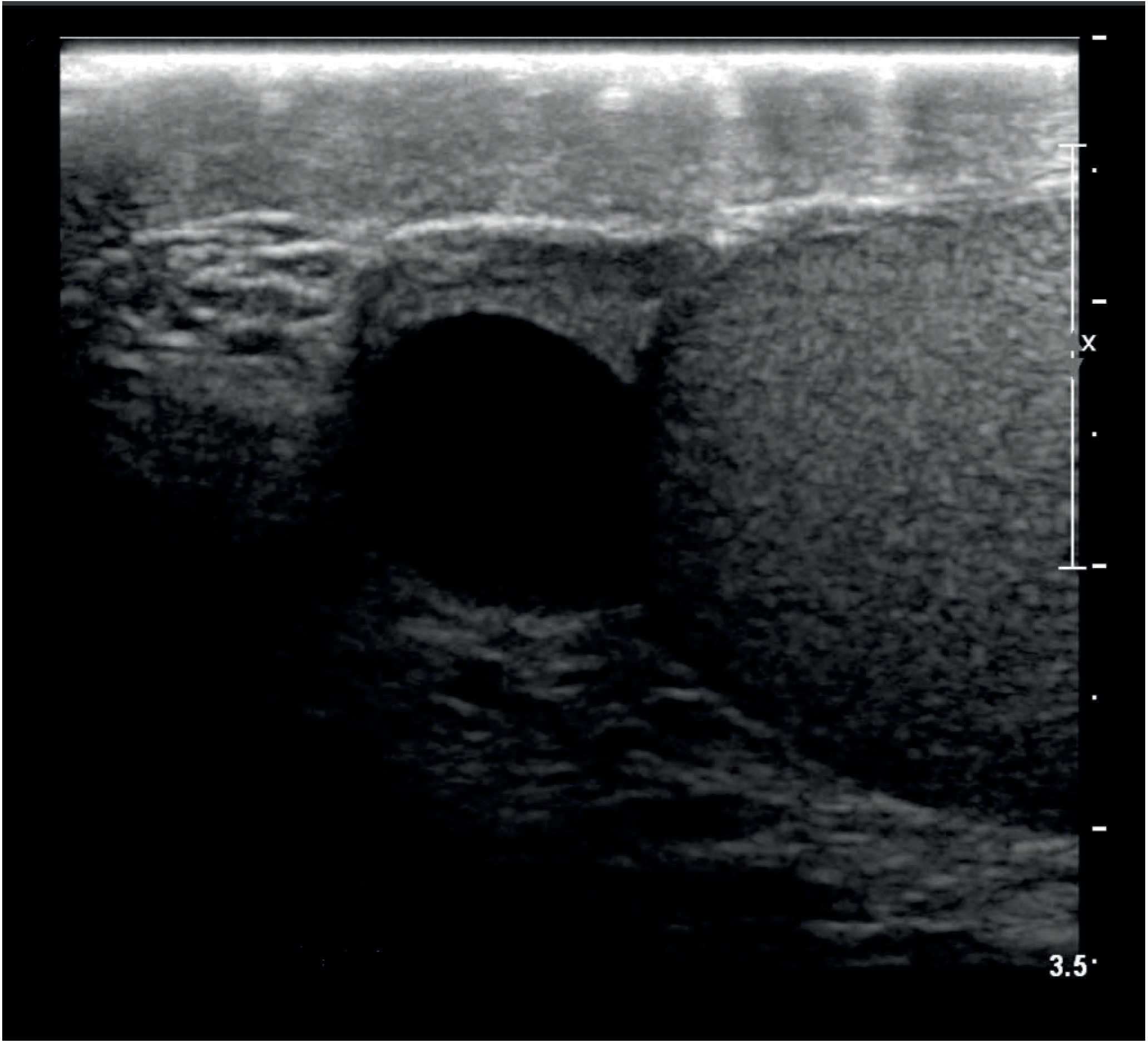
Step 7: Investigations
| Investigation | Purpose |
|---|---|
| Scrotal USS | Most important adjunct - confirms diagnosis, assesses testis (especially when impalpable within the hydrocele), excludes underlying tumor |
| Tumour markers (AFP, β-hCG, LDH) | If testicular tumor suspected (acute hydrocele in young man) |
| FBC/CRP | If secondary to infection |
Ultrasound image of a fluid-filled scrotal cyst:
Step 8: Differential Diagnosis of Scrotal Swelling
| Condition | Can Get Above? | Testis Palpable Separately? | Transillumination | Tender? |
|---|---|---|---|---|
| Vaginal hydrocele | Yes | No (enclosed) | Yes - brightly | No |
| Epididymal cyst | Yes | Yes (separate) | Yes (brightly) | No |
| Inguinoscrotal hernia | No | Yes | No | No (unless obstructed) |
| Testicular tumor | Yes | No (within testis) | No | No (usually) |
| Epididymo-orchitis | Yes | No (swollen, tender) | No | Yes |
| Haematocele | Yes | No | No | Variable |
| Varicocele | Yes | Yes | No | Dull ache |
| Hydrocele of cord | Yes | Yes (below) | Yes | No |
Examination Summary (OSCE-Style)
"This patient has a smooth, globular, non-tender, fluctuant swelling in the right scrotum. The upper border is well-defined and I am able to get above the swelling to feel a normal spermatic cord. The testis and epididymis are not separately palpable within the swelling. There is no cough impulse and the swelling is not reducible. Transillumination is positive - the swelling glows brightly. These findings are consistent with a vaginal hydrocele of the right side. I would confirm this with a scrotal ultrasound and ensure the underlying testis is normal."
- Bailey and Love's Short Practice of Surgery 28th Edition, p. 1586-1587
- General Anatomy and Musculoskeletal System - THIEME Atlas, p. 248
This is a shared conversation. Sign in to Orris to start your own chat.