Central type of lung cancer : specimen identification pathology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Excellent - I have the classic Robbins pathology figure. Now I can compile a thorough, well-illustrated answer.
Central Type of Lung Cancer: Specimen Identification & Pathology
Overview
"Central" lung cancers arise from the major bronchi (main, lobar, or segmental), forming a hilar/perihilar mass visible on gross examination and imaging. The two tumors that are classically central are:
| Type | Centrality | Key Gross Feature |
|---|---|---|
| Squamous Cell Carcinoma (SCC) | Central (most common central type) | Gray-white hilar mass; cavitation common |
| Small Cell Carcinoma (SCLC) | Centrally located, pale gray mass | Extends into parenchyma; widespread nodal disease |
Adenocarcinoma is classically peripheral, though it can occasionally arise centrally. Large cell carcinoma has no specific location predilection.
1. Squamous Cell Carcinoma - The Archetypal Central Tumor
Gross Specimen Identification
- Arises in major bronchi (main or lobar) - Panel D in the image below shows the classic appearance
- Gray-white firm mass at the hilum invading contiguous parenchyma
- Often causes bronchial obstruction - leading to distal atelectasis, obstructive pneumonia, or abscess
- Large lesions undergo central necrosis - creating cavitation (seen on imaging)
- First spreads to local hilar lymph nodes, then mediastinal nodes; distant spread is later than other types
Histological Identification
- Keratin pearls (concentric whorls of keratinized cells) - Panel C below
- Intercellular bridges (desmosomes) between cells - arrows in Panel C
- Ranges from well-differentiated (prominent keratinization) to poorly differentiated (minimal squamous features)
- Precursor lesion: squamous metaplasia → dysplasia → carcinoma in situ over years - detectable by sputum cytology early on
Immunohistochemistry (IHC)
- p40, p63 (squamous markers) - positive
- CK5/6 - positive
- TTF-1 - negative (distinguishes from adenocarcinoma)
Key Association
- Strongly associated with cigarette smoking (male predominance)
- Paraneoplastic hypercalcemia via PTH-related peptide secretion
2. Small Cell Carcinoma - The Other Central Type
Gross Specimen Identification
- Pale gray, centrally located mass extending into lung parenchyma
- Typically hilar/perihilar mass with mediastinal widening
- Virtually always has hilar and mediastinal lymph node metastases at diagnosis
- Surgical resection is rarely indicated - disease is essentially always systemic at presentation
Histological Identification (Panel F below)
- Cells are small, round to fusiform, with:
- Scant cytoplasm
- Finely granular chromatin ("salt-and-pepper" pattern)
- Indistinct nucleoli
- Cells arranged in diffuse sheets
- Numerous mitotic figures and extensive necrosis
- Azzopardi effect (also called Azzapardi): blue basophilic encrustation of vascular walls from DNA released by necrotic tumor cells - a hallmark feature
- Crush artifact in small biopsies (cells are very fragile)
Immunohistochemistry
- Neuroendocrine markers: Synaptophysin, Chromogranin A, CD56 - positive
- Ki-67: Very high (>80%) - reflects high proliferative rate
- TTF-1 - often positive (~90%)
- Epithelial markers (EMA, cytokeratin) - positive
Key Molecular Features
| Marker | Small Cell | Non-Small Cell |
|---|---|---|
| TP53 mutations | ~90% | ~50% |
| RB mutations | ~90% | ~20% |
| KRAS mutations | Rare | ~30% (adeno) |
| Neuroendocrine granules (EM) | Present | Absent |
| Mucin | Absent | Present (adeno) |
Paraneoplastic Syndromes (SCLC)
- SIADH - from ADH/vasopressin secretion
- Cushing syndrome - ACTH secretion
- Lambert-Eaton myasthenic syndrome - autoantibodies against voltage-gated calcium channels
- Gastrin-releasing peptide, calcitonin also secreted
Classic Pathology Image (Robbins)
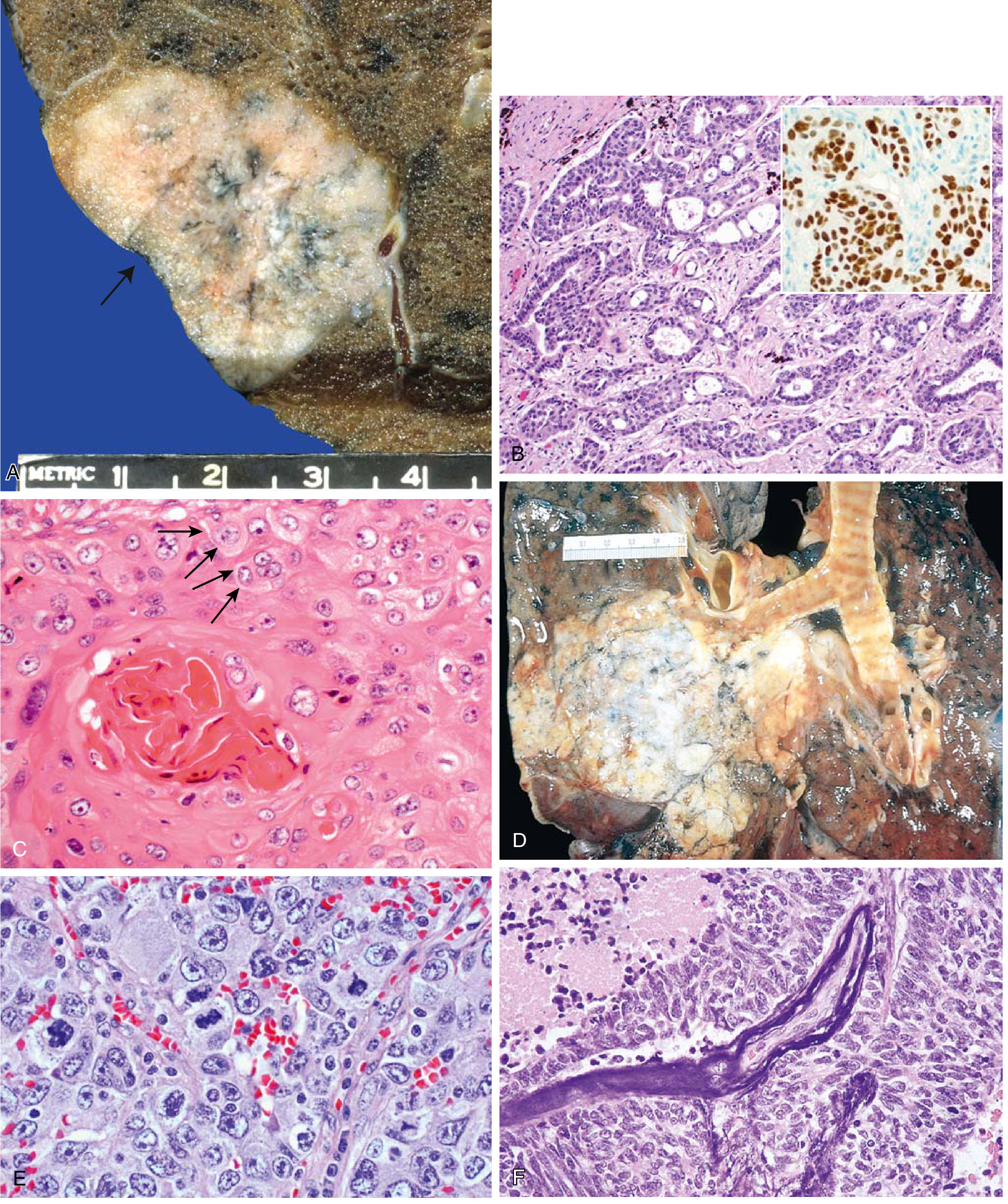
Panel D = Squamous cell carcinoma as a central (hilar) mass invading contiguous parenchyma - the classic gross specimen appearance of central lung cancer.
Panel F = Small cell carcinoma: small basophilic cells + necrosis (top left) + Azzopardi effect (blue DNA encrusting vessel walls).
Quick Comparison: Central vs. Peripheral
| Feature | Central (SCC / SCLC) | Peripheral (Adenocarcinoma) |
|---|---|---|
| Location | Major bronchi, hilum | Peripheral lung parenchyma |
| Gross | Hilar mass, cavitation (SCC) | Subpleural nodule, pleural puckering |
| Smoking | Strongly linked | Less so (adenocarcinoma can arise in non-smokers) |
| Early detection by sputum cytology | Yes (SCC) | Less useful |
| Cavitation | Common (SCC) | Rare |
| IHC TTF-1 | Negative (SCC); often positive (SCLC) | Positive |
| IHC p40/p63 | Positive (SCC) | Negative |
Specimen Workup for Central Lung Cancer
- Bronchoscopy + biopsy - first-line for central lesions (direct visualization)
- Bronchial washings / brushings / BAL - cytology for central airway tumors
- Sputum cytology - useful for squamous cell carcinoma (central, exfoliating cells)
- EBUS-guided TBNA - for hilar/mediastinal nodal staging
- Resection specimen - lobectomy/pneumonectomy; gross exam identifies the bronchial involvement, nodal status
Source: Robbins & Kumar Basic Pathology, pp. 485-490 (Fig. 11.44, Table 11.6)
Miliary tb Bronchiectasis : specimen identification pathology
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
I have all the content and images needed. Here is the comprehensive answer:
Miliary TB & Bronchiectasis: Specimen Identification & Pathology
PART 1: MILIARY TUBERCULOSIS
What is "Miliary" TB?
The term miliary derives from the Latin milium (millet seed). On gross examination, the lung (and other organs) are studded with innumerable tiny yellow-white foci resembling scattered millet seeds.
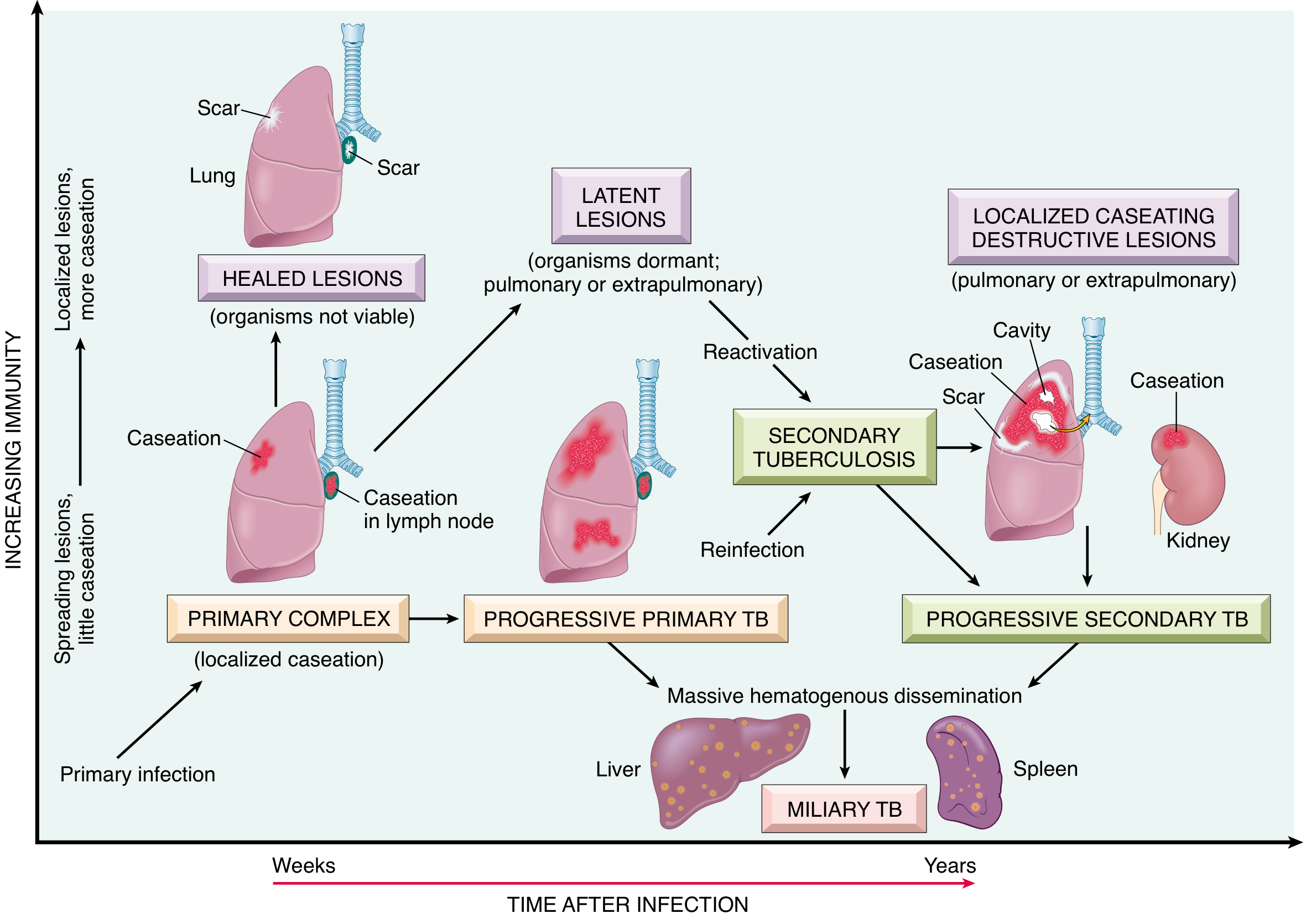
Pathogenesis - How Miliary TB Occurs
Miliary TB results from massive hematogenous dissemination of Mycobacterium tuberculosis, which occurs in two settings:
- Progressive primary TB - organisms drain through lymphatics → enter venous blood → recirculate to lung via pulmonary arteries
- Progressive secondary (reactivation) TB - erosion of a cavity into a blood vessel seeds the systemic circulation
The natural history and spectrum, including where miliary TB fits, is shown in this diagram:
Gross Specimen Identification
| Feature | Description |
|---|---|
| Size | 1-2 mm (millet seed sized) foci |
| Color | Yellow-white |
| Texture | Firm, discrete nodules |
| Distribution | Randomly scattered throughout lung parenchyma |
| Cut surface | Both lungs uniformly peppered; same lesions visible in liver, spleen, bone marrow, adrenals, kidneys, fallopian tubes, epididymis |
| Appearance | Consolidation-like at microscopic level; macroscopically punctate |
Key gross feature: Unlike secondary (postprimary) TB which concentrates at lung apices, miliary foci are randomly distributed throughout the entire lung - upper, middle, and lower lobes equally involved.
When miliary lesions enlarge and coalesce, they can produce consolidation of large regions or even whole lobes.
Microscopic/Histological Identification
The hallmark is the caseating granuloma:
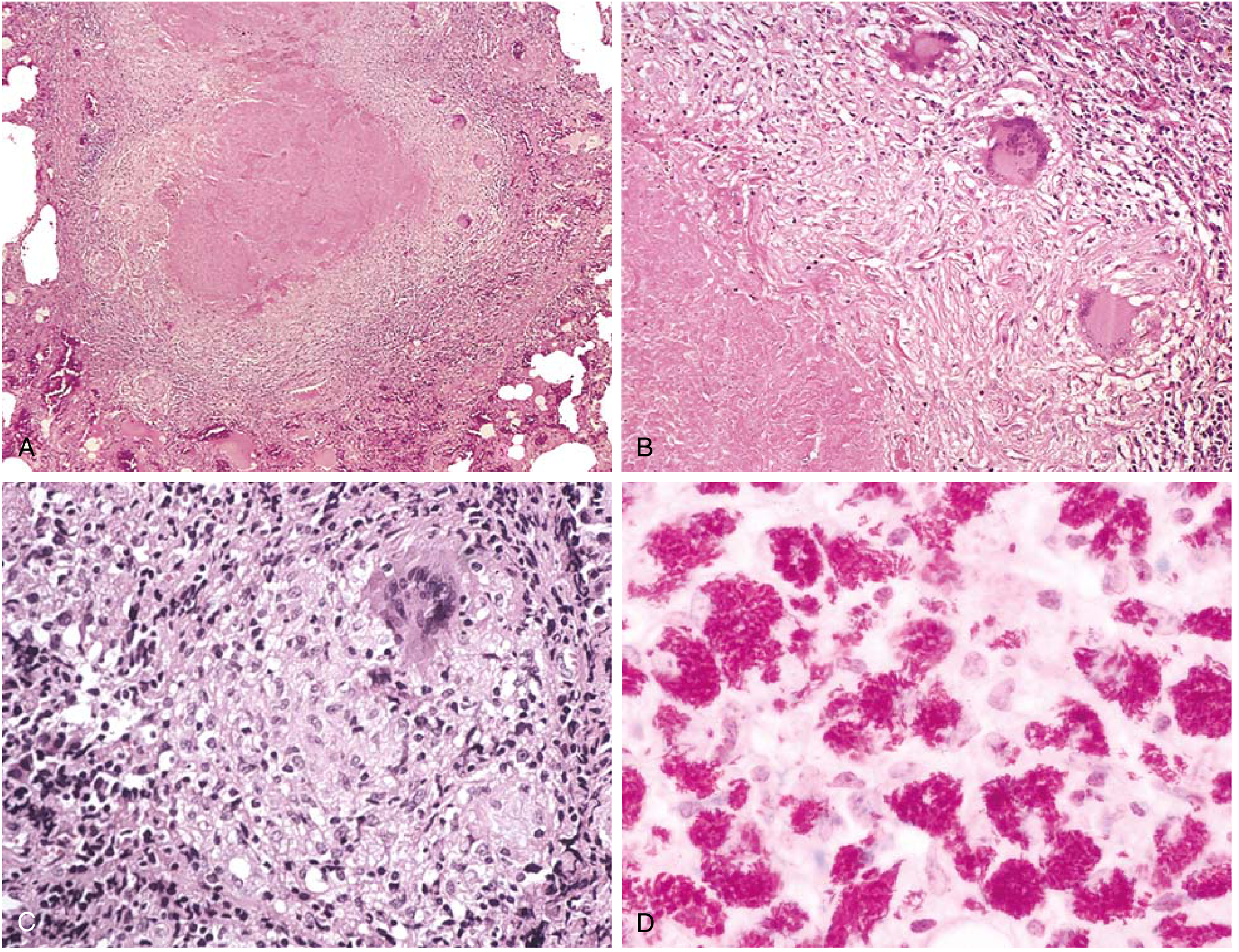
Panel A & B = Classic tubercle: central caseous necrosis surrounded by epithelioid histiocytes and multinucleated Langhans giant cells, enclosed by a fibrolymphocytic rim.
Panel C = Non-caseating granuloma (can occur even in immunocompetent patients - always stain for AFB regardless).
Panel D = Immunocompromised patient: no granulomas - instead sheets of macrophages packed with mycobacteria (acid-fast stain shows red bacilli).
Histological Components of Each Miliary Focus:
- Central caseous necrosis - pink, granular, cheese-like, acellular core
- Epithelioid macrophages - elongated, activated macrophages surrounding the necrotic center
- Langhans giant cells - multinucleated giant cells with nuclei arranged in a horseshoe/peripheral pattern at the granuloma periphery
- Lymphocytic cuff - outer rim of lymphocytes
- Fibroblastic rim - peripheral fibrosis in healing lesions
Special Stains
- Ziehl-Neelsen (ZN) / Kinyoun stain - acid-fast bacilli stain red against a blue background
- Bacilli are most numerous in the early exudative and caseous phases but too few to find in late fibrocalcific stages
- In immunocompromised: AFB are abundant but granulomas are absent
Systemic Miliary TB - Organ Distribution
| Organ | Findings |
|---|---|
| Liver | Yellow-white miliary nodules on surface and cut section |
| Spleen | Enlarged; studded with firm yellow-white granulomas |
| Bone marrow | Granulomas detectable on trephine biopsy |
| Meninges | Tuberculous meningitis |
| Kidneys | Noncaseating granulomas (may progress to renal TB) |
| Adrenal glands | Can cause Addison disease |
| Fallopian tubes / epididymis | Genital TB |
PART 2: BRONCHIECTASIS
Definition
Bronchiectasis is permanent abnormal dilation of bronchi, resulting from chronic transmural inflammation that destroys the muscular and elastic components of bronchial walls, replacing them with fibrous tissue.
Pathogenesis
The key sequence:
- Impaired airway defense (mucociliary clearance failure, immune deficiency) → bacterial colonization
- Chronic infection → recruitment of neutrophils and macrophages
- Proteolytic and oxidative enzyme release (from both bacteria and inflammatory cells) → destruction of smooth muscle and elastic tissue
- Fibrous replacement → permanent dilation
- Bronchial hypervascularity - bronchial arteries hypertrophy; abnormal bronchial-pulmonary arterial anastomoses form (basis of massive hemoptysis)
Common pathogens: Haemophilus spp. (55%), Pseudomonas spp. (26%), Streptococcus pneumoniae (12%)
Gross Specimen Identification
| Feature | Description |
|---|---|
| Location | Most often bilateral lower lobes (gravity-dependent pooling of secretions); upper lobes in TB and CF |
| Dilated airways | Visibly widened bronchi extending peripherally (normally bronchi taper toward periphery - in bronchiectasis, they fail to taper or widen) |
| Contents | Airways filled with thick, purulent material (pus) or mucus plugs |
| Wall | Bronchial walls thickened, fibrotic, inflamed |
| Distal airways | Occluded by secretions or obliterated by fibrosis |
| Cut section | Multiple dilated sac-like spaces, cysts, or tubular channels - the classic "multiple cystic cavities" on cut section of lower lobe |
Three Morphological Types (Gross & Radiological Classification)
| Type | Gross Description | CT/CXR Appearance |
|---|---|---|
| Cylindrical (tubular) | Uniformly dilated bronchi; regular lumen; walls parallel | Tram-track sign (parallel linear opacities); signet ring sign (dilated bronchus beside pulmonary artery) |
| Varicose | Irregular/beaded pattern of dilated bronchi; alternating constrictions and dilatations | String of pearls appearance |
| Saccular (cystic) | Peripheral balloon-type dilation; most severe type; most common after obstruction/infection | Clusters of cysts; ring shadows; air-fluid levels |
Saccular type is the most common after bronchial obstruction or infection.
Microscopic/Histological Identification
- Bronchial wall destruction - loss of smooth muscle, elastic tissue, cartilage
- Chronic transmural inflammation - neutrophils, lymphocytes, plasma cells throughout bronchial wall
- Luminal exudate - purulent material (neutrophils, bacteria, debris) filling lumen
- Fibrosis - replaces destroyed muscular/elastic components
- Goblet cell metaplasia - excessive mucus secretion
- Bronchial artery hypertrophy - increased submucosal vascularity, anastomotic channels
- Squamous metaplasia of bronchial epithelium in chronic disease
Causes Affecting Specimen Distribution
| Distribution | Cause |
|---|---|
| Bilateral lower lobes | Post-infectious, aspiration |
| Upper lobes | TB, cystic fibrosis, allergic bronchopulmonary aspergillosis (ABPA) |
| Middle lobe / lingula | Right middle lobe syndrome, NTM (Lady Windermere syndrome) |
| Diffuse | Cystic fibrosis, primary ciliary dyskinesia, hypogammaglobulinemia |
Comparison Summary
| Feature | Miliary TB | Bronchiectasis |
|---|---|---|
| Gross hallmark | 1-2 mm yellow-white millet seed-like foci scattered throughout lung | Permanently dilated bronchi filled with pus; lower lobe predominance |
| Histological hallmark | Caseating granuloma with Langhans giant cells | Chronic transmural inflammation; wall destruction; fibrosis |
| Key special stain | ZN / acid-fast stain (red bacilli) | None specific; H&E sufficient |
| Distribution | Random (hematogenous) - all lobes equally | Gravity-dependent; bilateral lower lobes (common) |
| Contents | Granulomas / caseous foci | Pus, mucus, secretions |
| Vascular change | Minimal | Bronchial artery hypertrophy, abnormal anastomoses |
| Complication | Meningitis, Addison disease, organ failure | Massive hemoptysis, amyloidosis, cor pulmonale |
Sources: Robbins & Kumar Basic Pathology, pp. 476-478 (TB morphology, miliary TB); Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 353-354 (miliary TB); Schwartz's Principles of Surgery, 11th Ed., pp. 2332-2334 (bronchiectasis morphology)
Breast carcinoma Peptic ulcer : specimen identification pathology
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
Finding Sources
Finding Sources
I now have comprehensive content and all key images. Let me compile the full answer.
PART 1: BREAST CARCINOMA - Specimen Identification & Pathology
Gross Specimen Identification
The gross appearance of breast carcinoma depends on the stromal reaction (desmoplasia):
| Gross Feature | Description |
|---|---|
| Size | Usually 2-3 cm at presentation (without mammographic screening) |
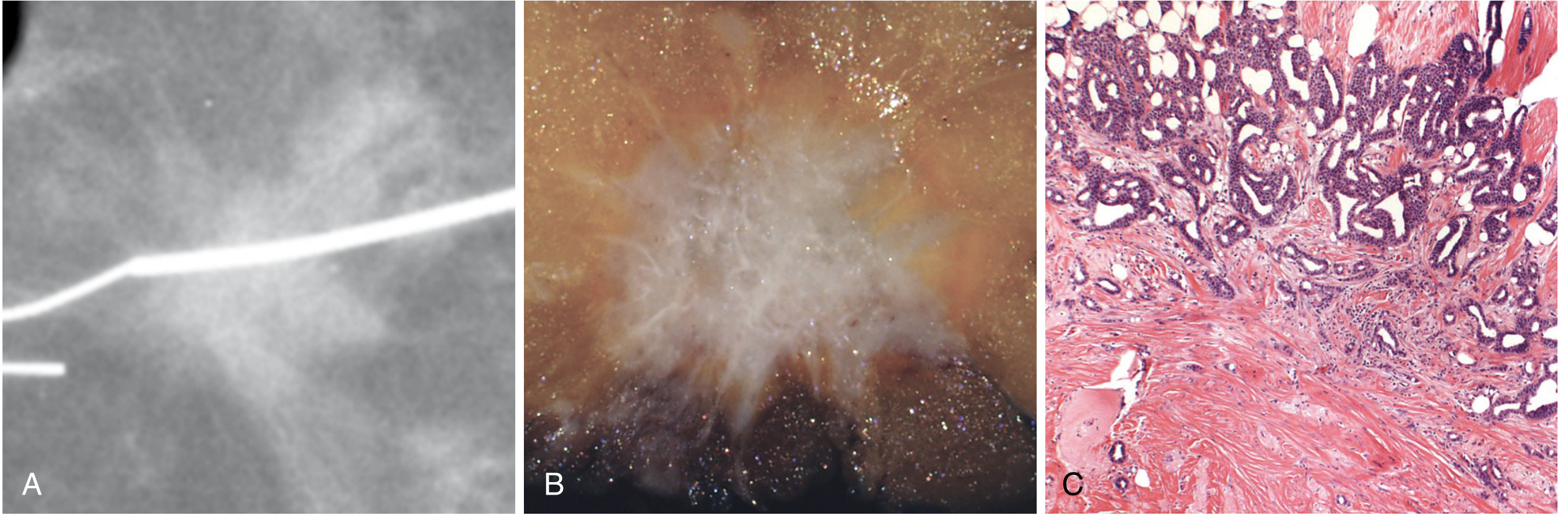
| Shape | Irregular, poorly defined, stellate/spiculated margins ("star-shaped") |
| Consistency | Hard, gritty or "stone-like" when cut - due to desmoplastic stroma and microcalcifications |
| Cut surface sound | Characteristic grating or scratching sound when scraped (chalky-white desmoplastic stroma + calcifications) |
| Color | Chalky-white to pale gray-yellow on cut section |
| Borders | Poorly circumscribed; infiltrating into surrounding fat |
| Skin changes | Skin retraction, dimpling (Cooper ligament tethering); peau d'orange (lymphatic obstruction causing skin edema) |
| Nipple | May show retraction or Paget's disease (eczematous nipple changes) |
Key gross teaching point: In scirrhous (hard) carcinoma, the breast may be shrunken and drawn in toward the growth. Pulling at the breast produces dimpling or puckering - this is due to tumor infiltration shortening Cooper's suspensory ligaments.
Histological Grading (Nottingham Histologic Score)
All invasive breast carcinomas are graded 1-3 based on three features, each scored 1-3:
| Feature | Grade 1 (Score 1) | Grade 2 (Score 2) | Grade 3 (Score 3) |
|---|---|---|---|
| Tubule/gland formation | >75% of tumor forms tubules | 10-75% tubules | <10% tubules |
| Nuclear pleomorphism | Small, regular, uniform nuclei | Moderate variability | Marked pleomorphism, prominent nucleoli |
| Mitotic rate | Low | Moderate | High |
Total score: 3-5 = Grade 1 (well differentiated); 6-7 = Grade 2 (moderate); 8-9 = Grade 3 (poorly differentiated)
Histological Types
1. Invasive Carcinoma of No Special Type (NST) / Invasive Ductal Carcinoma (IDC)
- Most common (~70-80%)
- Haphazard stromal invasion
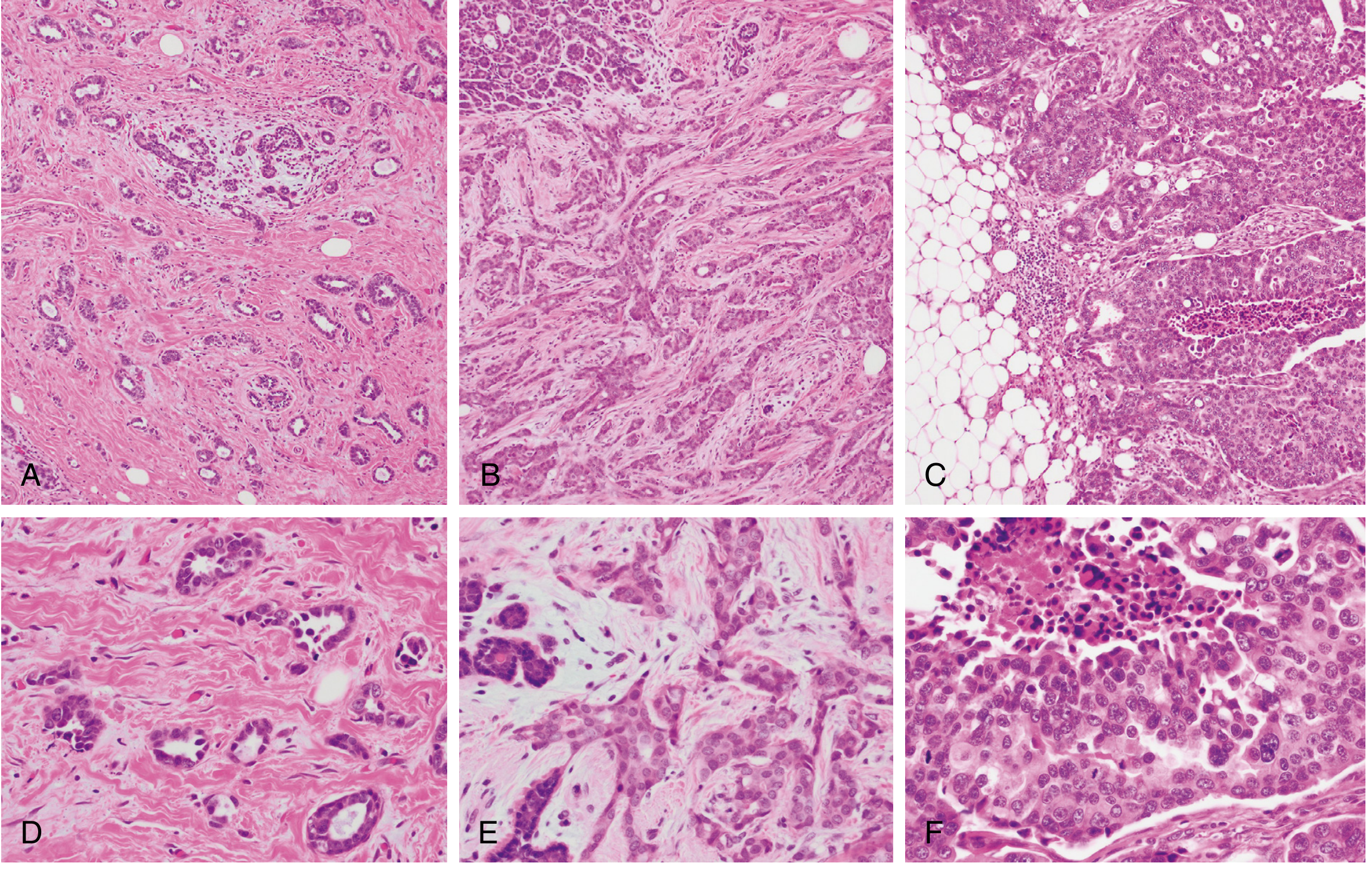
- Exuberant desmoplastic response (dense fibrous stroma) - Panel C in Fig. 23.20 above
- Variable tubule formation depending on grade
2. Special Histological Subtypes
| Subtype | Histological Hallmark | ER/PR/HER2 Status |
|---|---|---|
| Invasive Lobular Carcinoma | Dyscohesive cells in linear cords ("Indian file" / "single-file" pattern); signet ring cells with intracytoplasmic mucin | ER+/PR+ (luminal) |
| Mucinous (Colloid) Carcinoma | Clusters of tumor cells floating in large lakes of extracellular mucin; soft, gelatinous, well-circumscribed on gross | ER+/PR+ |
| Tubular Carcinoma | Exclusively well-formed tubules; may mimic benign sclerosing lesion | ER+/PR+ |
| Medullary Pattern | Sheets of high-grade tumor with prominent tumor-infiltrating lymphocytes (TILs); well-circumscribed; scant desmoplasia | Often TNBC |
| Metaplastic Carcinoma | Squamous or mesenchymal (spindle, chondroid, osseous) differentiation within the tumor | TNBC |
| Papillary Carcinoma | True papillary fronds lined by tumor cells | ER+/PR+ |
ILC key feature: Loss of E-cadherin expression (CDH1 gene mutation) - single cells cannot adhere; also predisposes to signet ring carcinoma of stomach.
Immunohistochemistry (IHC) - Receptor Status
| Marker | Significance |
|---|---|
| ER (Estrogen Receptor) | Positive in ~70% of invasive carcinomas; predicts response to hormonal therapy (tamoxifen, aromatase inhibitors) |
| PR (Progesterone Receptor) | Co-expressed with ER; additional prognostic value |
| HER2/neu (ERBB2) | Amplified/overexpressed in ~20%; predicts trastuzumab (Herceptin) response |
| Ki-67 | Proliferative index; high in grade 3 / TNBC |
| TTF-1 | Negative (helps exclude lung primary in metastatic setting) |
| GCDFP-15 | Positive in breast (apocrine differentiation) |
| GATA3 | Highly specific breast marker; useful in carcinoma of unknown primary |
| CK7+/CK20- | Typical breast IHC profile |
Triple Negative Breast Cancer (TNBC): ER-/PR-/HER2- = worst prognosis; no targeted therapy; often basal-like.
Spread of Breast Carcinoma
- Lymphatic: Axillary nodes (most common) → supraclavicular nodes → Virchow node (left); internal mammary nodes
- Hematogenous: Lung, liver, bone (especially axial skeleton), brain, adrenal glands
- ILC-specific spread: Peritoneum, retroperitoneum, leptomeninges, GI tract, ovaries, uterus
PART 2: PEPTIC ULCER - Specimen Identification & Pathology
Definition
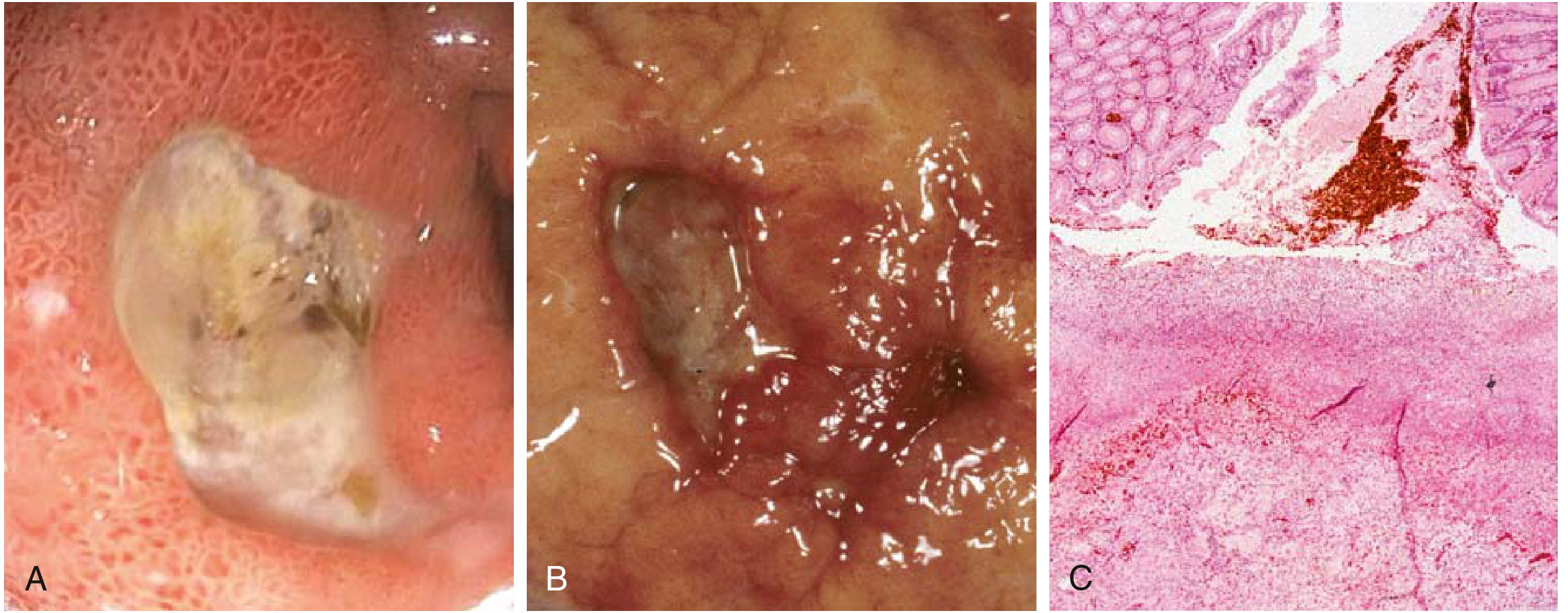
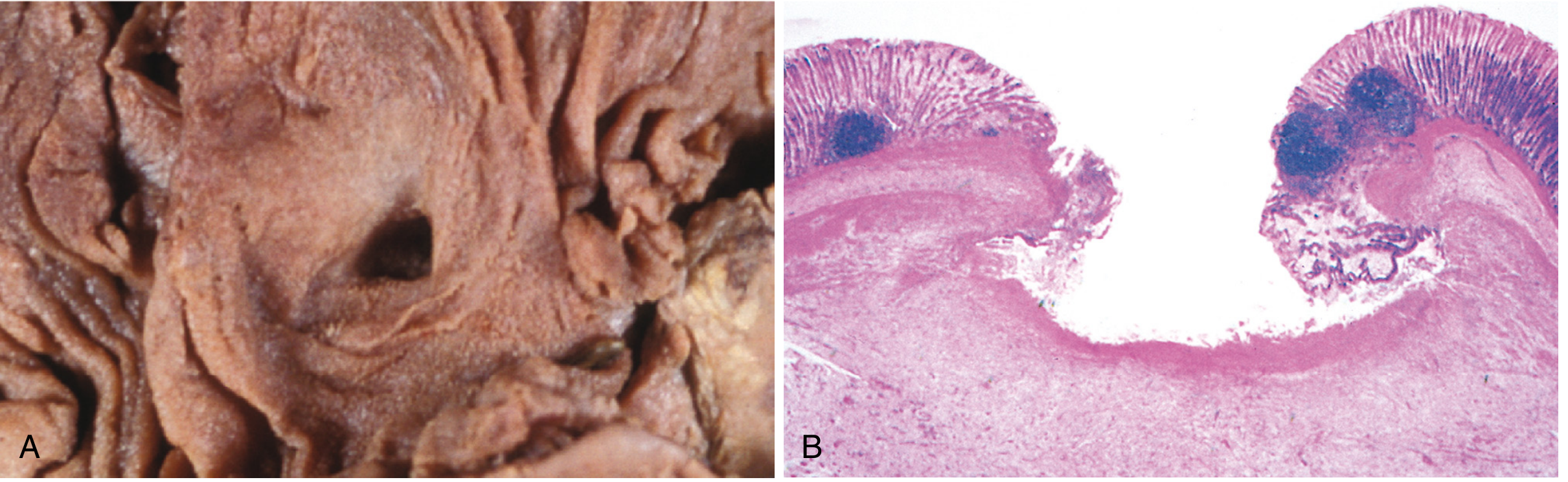
A peptic ulcer is a round to oval, sharply punched-out mucosal defect that extends through the muscularis mucosae into the submucosa or deeper, resulting from an imbalance between acid/pepsin damage and mucosal defense mechanisms.
Gross Specimen Identification
Sites
- Proximal duodenum (most common, 4x more than stomach) - within a few cm of the pyloric valve, anterior duodenal wall
- Gastric - lesser curvature at the junction of body and antrum
Gross Features
| Gross Feature | Peptic Ulcer (Benign) | Malignant Ulcer (Gastric Cancer) |
|---|---|---|
| Edge | Sharply punched-out, clean, "as if punched with a hole punch" | Heaped-up, irregular, everted margins |
| Mucosal margin | Level with or slightly overhanging surrounding mucosa | Raised, indurated, nodular |
| Mucosal folds | Radiate toward the ulcer base like spokes | Fused, clubbed, or stop before reaching the edge |
| Base | Smooth and clean (peptic digestion of exudate); gray-white or brown | Necrotic, irregular, shaggy |
| Shape | Round to oval | Irregular |
| Number | Solitary in >80% | Variable |
| Depth | Through muscularis mucosae (at least) | Variable |
Microscopic/Histological Identification
The chronic peptic ulcer has a classic four-zone architecture from the surface inward:
Four Layers (Surface to Depth)
| Zone | Composition | Description |
|---|---|---|
| Zone 1 (Surface) | Fibrinoid necrotic slough | Thin layer of fibrinoid debris; degraded blood products; neutrophilic exudate |
| Zone 2 | Active inflammatory exudate | Neutrophilic infiltrate; acute inflammatory cells |
| Zone 3 | Granulation tissue | Highly vascular; immature capillaries; neutrophils + mononuclear cells; fibroblasts - this is the ulcer base |
| Zone 4 (Deepest) | Fibrous / collagenous scar | Dense collagen (fibrosis); may involve entire wall thickness |
Additional microscopic features:
- Endarteritis obliterans: Larger vessels in the scarred base are thickened with narrowed lumen - and may be thrombosed (cause of hemorrhage)
- Radiating mucosal folds: Scarring draws surrounding mucosa into folds that radiate outward (visible on gross and endoscopy)
- Foveolar metaplasia: Gastric-type cells in duodenal ulcers (protective response)
- H. pylori: Identifiable in superficial mucous layer with Giemsa, Warthin-Starry silver stain, or immunohistochemistry - comma/S-shaped organisms
- Perineural inflammation: Chronic inflammatory cells around nerves (contributes to pain)
Benign vs. Malignant Ulcer - Key Differentiation
| Feature | Benign Peptic Ulcer | Malignant (Carcinomatous) Ulcer |
|---|---|---|
| Edges | Punched out, clean, regular | Heaped up, irregular, everted |
| Mucosal folds | Radiate to crater edge | Stop short; fused or clubbed |
| Base | Smooth, clean, granulation tissue | Necrotic, shaggy |
| Surrounding mucosa | Normal or gastritis | Thickened, nodular, indurated |
| Depth | Deep but regular | Variable |
| Biopsy edges | Normal epithelium | Malignant cells |
Clinical pearl: All gastric ulcers require biopsy from the edge (4-quadrant + base) to exclude malignancy. Duodenal ulcers are almost never malignant and do not routinely require biopsy.
Complications of Peptic Ulcer Disease
| Complication | Frequency | Key Pathology |
|---|---|---|
| Hemorrhage | 15-20% (most common) | Erosion of endarteritic vessels; accounts for 25% of ulcer deaths |
| Perforation | ~5% | Free air under diaphragm; chemical/bacterial peritonitis |
| Pyloric stenosis | Chronic scarring | Gastric outlet obstruction; succussion splash |
| Penetration | Into adjacent organs | Into pancreas (posterior DU) → pancreatitis; into liver |
| Malignant transformation | Rare (gastric only) | Not seen with duodenal ulcers |
Quick Comparison Summary
| Feature | Breast Carcinoma | Peptic Ulcer |
|---|---|---|
| Gross hallmark | Hard, irregular, stellate, gritty mass; spiculated margins; skin dimpling | Round, punched-out defect; clean base; mucosal folds radiating to crater |
| Histological hallmark | Invasive epithelial cells + desmoplastic stroma; graded by tubules/nuclei/mitoses | Four-zone architecture: fibrinoid necrosis → exudate → granulation tissue → fibrosis |
| Consistency on cut | Grating/scratchy (calcifications + desmoplasia) | Ulcer base smooth; edges firm (fibrotic) |
| Key special stain | ER, PR, HER2 IHC; GATA3 | H. pylori (Giemsa, Warthin-Starry) |
| Key complication | Lymph node metastasis; systemic spread | Hemorrhage (most common); perforation |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 978-979 (Figs. 23.20-23.21), pp. 717-718 (Fig. 17.17); Robbins & Kumar Basic Pathology, pp. 555-556 (Fig. 13.15)
This is a shared conversation. Sign in to Orris to start your own chat.