Parathyroid gland
Reading File
Finding Sources
Searching the Web
parathyroid gland anatomy physiology hormones 2024
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is a comprehensive overview of the parathyroid gland, drawing from Harrison's Principles of Internal Medicine 22E, Medical Physiology (Boron & Boulpaep), and Histology: A Text and Atlas.
Parathyroid Gland
Anatomy & Location
There are four parathyroid glands (two superior, two inferior), located on the posterior, medial aspect of each thyroid lobe. They are supplied by the inferior thyroid artery in most individuals, though vascular supply may arise from anastomoses between the superior and inferior thyroid arteries.
- Weight: ~30–40 mg each
- Size: ~3–4 mm (pea-sized)
- Embryology: Superior glands derive from 4th pharyngeal pouch; inferior glands from the 3rd pharyngeal pouch (along with the thymus — which explains why inferior glands can be ectopic, sometimes found in the mediastinum)
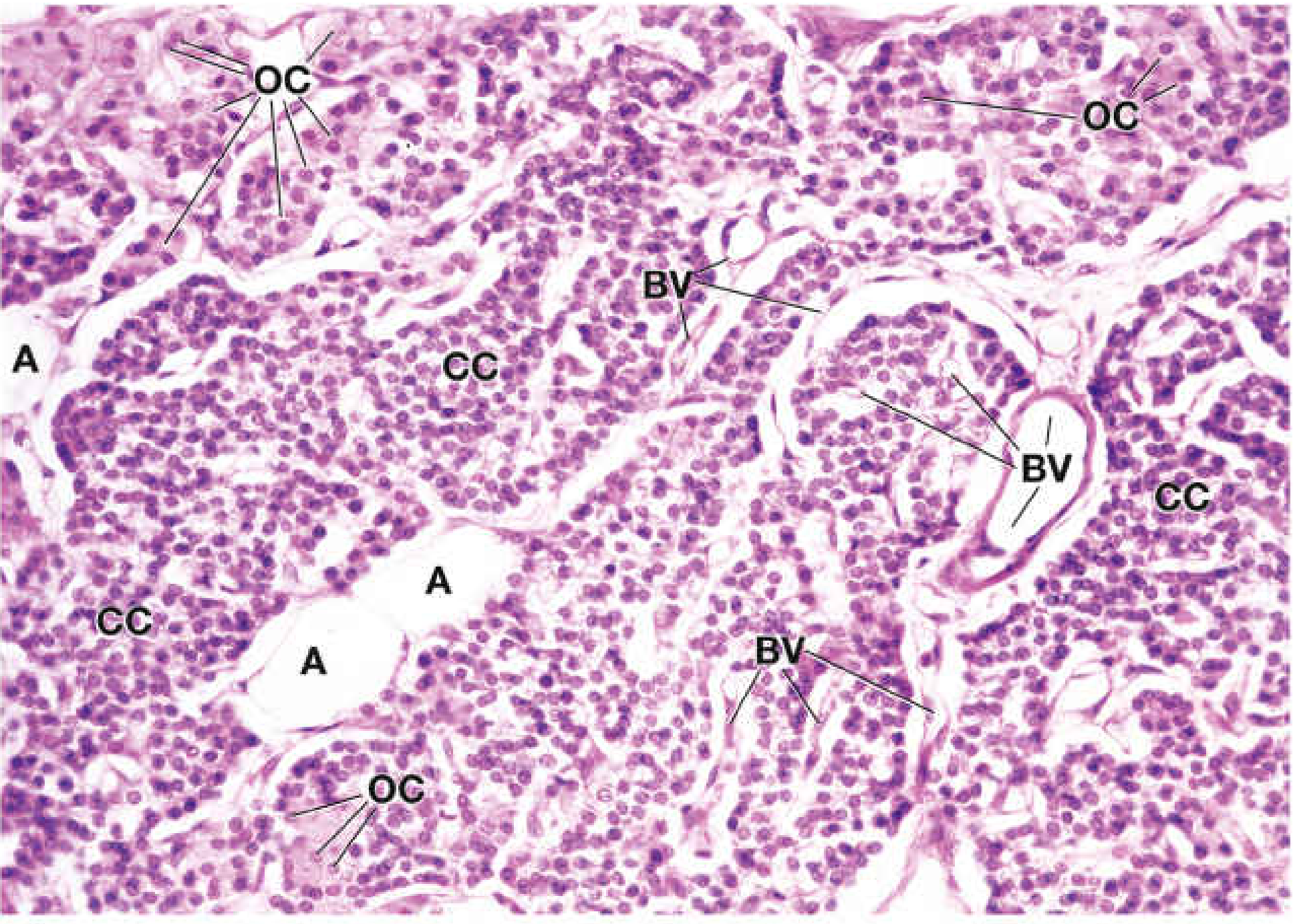
Histology
The parenchyma is arranged as cords or sheets of cells separated by capillaries and delicate connective tissue septa. Two cell types are identifiable on H&E:
| Cell Type | Features | Function |
|---|---|---|
| Chief cells (principal cells) | Most numerous; small round nucleus, scant cytoplasm | Synthesize and secrete PTH |
| Oxyphil cells | Larger, fewer; eosinophilic cytoplasm, smaller darker nucleus; appear in clusters | Function uncertain; appear at end of first decade, increase around puberty |
Blood vessels and adipose tissue are associated with connective tissue trabeculae.
PTH — Structure & Biosynthesis
- 84-amino acid single-chain peptide
- The amino-terminal PTH(1–34) fragment is biologically active and highly conserved
- Synthesized as pre-pro-PTH → signal sequence cleaved in ER lumen → pro-PTH → pro-sequence cleaved in Golgi → mature PTH stored in secretory granules
Actions of PTH
PTH is the primary regulator of calcium homeostasis in the extracellular fluid (ECF).
Bone
- Stimulates osteoclast-mediated bone resorption → releases Ca²⁺ and phosphate into blood
- Chronically high PTH → increased bone turnover, osteoporosis
Kidney
- Distal tubule: Increases Ca²⁺ reabsorption (↑ serum Ca²⁺)
- Proximal tubule: Inhibits phosphate reabsorption → phosphaturia (↓ serum phosphate)
- Proximal tubule: Stimulates 1α-hydroxylase → converts 25-OH vitamin D → 1,25(OH)₂D (calcitriol)
Intestine (indirect)
- Via calcitriol → increases intestinal Ca²⁺ and phosphate absorption
Net effect: ↑ serum Ca²⁺, ↓ serum phosphate
Regulation of PTH Secretion
PTH secretion is controlled by a tight negative feedback loop:
| Stimulus | Effect on PTH |
|---|---|
| ↓ Serum Ca²⁺ | ↑ PTH secretion (major stimulus) |
| ↑ Serum Ca²⁺ | ↓ PTH via calcium-sensing receptor (CaSR) |
| ↑ 1,25(OH)₂D | ↓ PTH synthesis and release |
| ↑ FGF23 | ↓ PTH secretion |
| Hypomagnesemia | Impairs PTH secretion (paradoxically) |
Calcium-Sensing Receptor (CaSR) Mechanism
Ca²⁺ binds the CaSR on chief cells → activates Gαx → PLC activation → IP₃ + DAG → ↑ intracellular Ca²⁺ + PKC activation → inhibition of PTH granule release (counterintuitive: most secretory cells are stimulated, not inhibited, by this pathway).
PTH Receptor
- PTH1R (primary receptor): G protein-coupled receptor, couples to adenylyl cyclase (↑ cAMP) and phospholipase C; most abundant in kidney (proximal and distal convoluted tubules) and bone
- PTH2R: Identified but role in calcium homeostasis unclear
- PTH and PTHrP (parathyroid hormone-related peptide) act through the same PTH1R receptor
Disorders
Hypercalcemia
| Cause | Mechanism |
|---|---|
| Primary hyperparathyroidism | Adenoma (most common ~80%), hyperplasia, carcinoma; autonomous PTH excess |
| Humoral hypercalcemia of malignancy (HHM) | PTHrP overproduction by tumor cells (squamous cell carcinoma of lung, kidney, breast) |
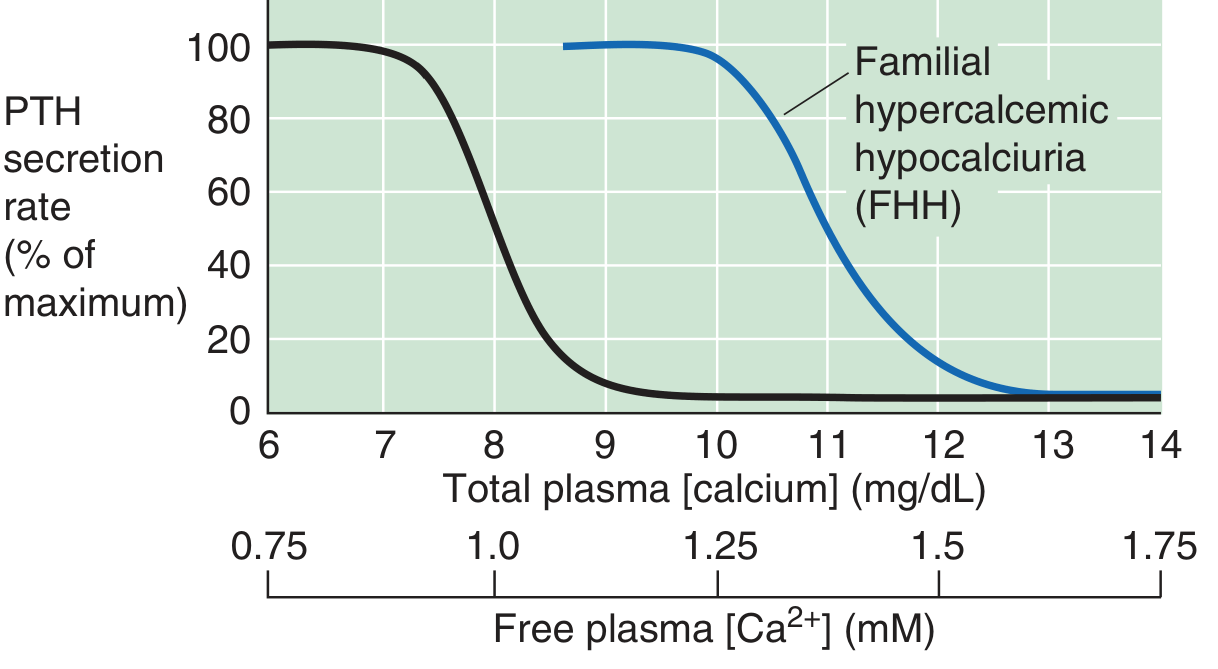
| Familial hypocalciuric hypercalcemia (FHH) | Inactivating CaSR mutation → set-point shift right → PTH unsuppressed at normal Ca²⁺ levels |
| Vitamin D toxicity, granulomatous disease (sarcoidosis), lymphoma | Excess 1,25(OH)₂D |
Symptoms of hypercalcemia: Fatigue, depression, mental confusion, anorexia, nausea/vomiting, constipation, polyuria, nephrolithiasis, short QT on ECG, arrhythmias (typically symptomatic at Ca²⁺ >11.6–12.0 mg/dL)
Hypocalcemia
| Cause | Mechanism |
|---|---|
| Hypoparathyroidism | PTH deficiency (post-surgical, autoimmune, DiGeorge syndrome) |
| Pseudohypoparathyroidism (PHP) | PTH resistance at proximal renal tubule |
| Hypomagnesemia | Impairs PTH secretion and end-organ response |
Clinical Pearls
- Surgery for primary hyperparathyroidism is highly effective and reverses bone density loss
- Calcimimetics (e.g., cinacalcet) activate CaSR → suppress PTH → used in secondary/tertiary hyperparathyroidism
- Calcilytics (CaSR negative allosteric modulators) show promise in autosomal dominant hypocalcemia type 1
- PTH(1–34) (teriparatide) is used therapeutically for postmenopausal osteoporosis and as hormone replacement in hypoparathyroidism
- About 50% of total plasma Ca²⁺ is ionized (free); PTH responds to the ionized fraction, not total calcium
Sources: Harrison's Principles of Internal Medicine 22E, p. 3315–3318; Medical Physiology (Boron & Boulpaep), p. 1554–1555; Histology: A Text and Atlas, p. 2067–2069
This is a shared conversation. Sign in to Orris to start your own chat.