i was studying penicilin nd cephalosproins, im losing my mind thus was i need u yo do , need u to write the drugs acc to thier classification nd WHIH INFECTIONS ARE THEY USED FOR LIKE EHICH BACTERIAS, ND ARE THOSE G -VE OR +VE
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything I need for a complete, well-organized answer. Let me put it all together.
Penicillins & Cephalosporins - Complete Classification Guide
Mechanism of Action (Both Classes)
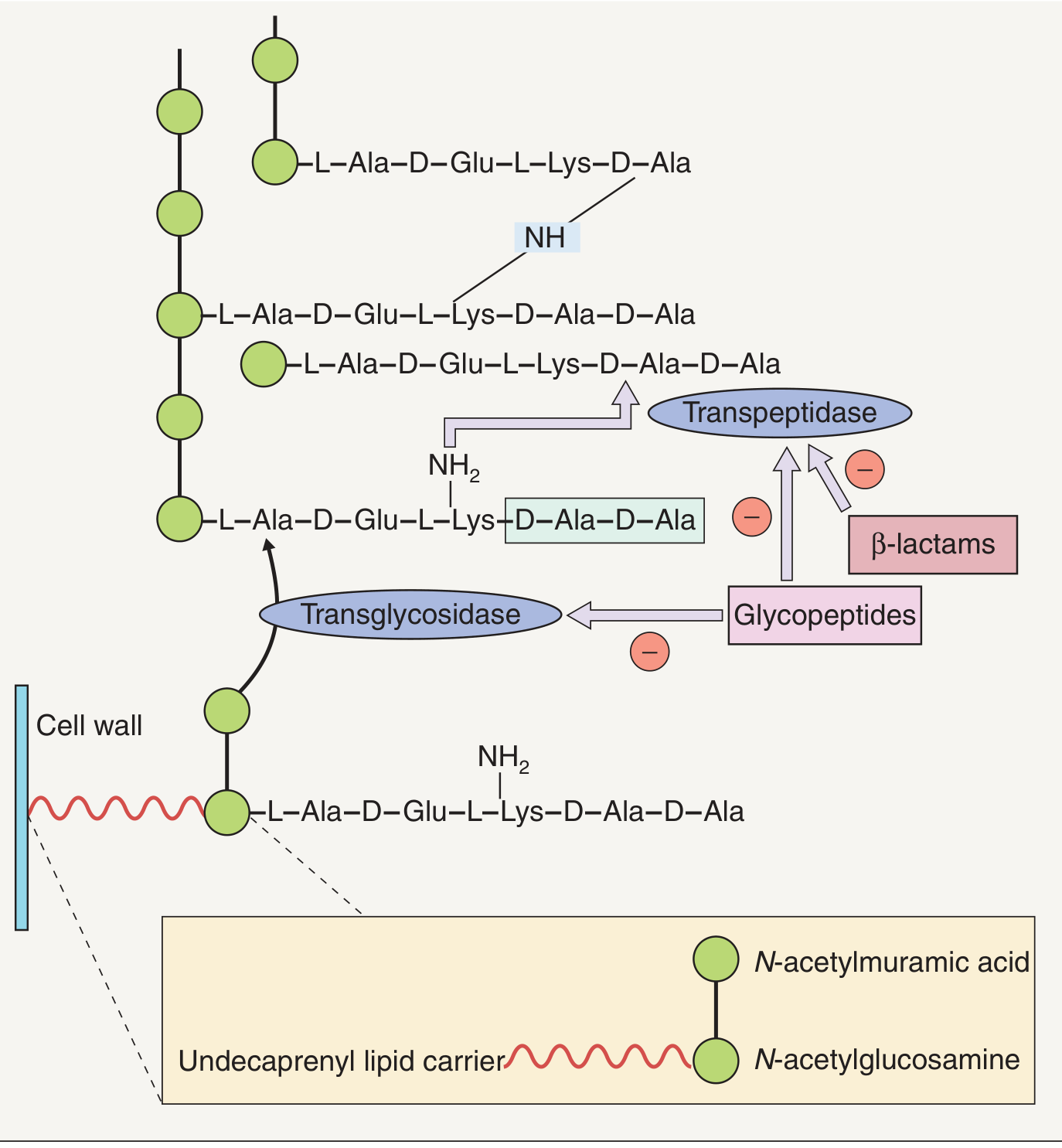
Both penicillins and cephalosporins are beta-lactam antibiotics. They are bactericidal - they kill bacteria by binding to Penicillin-Binding Proteins (PBPs) and blocking transpeptidase cross-linking of peptidoglycan chains in the bacterial cell wall.
PART 1: PENICILLINS
Penicillins are divided into 4 groups based on their spectrum:
Group 1 - Natural Penicillins
| Drug | Route |
|---|---|
| Penicillin G (benzylpenicillin) | IV/IM |
| Penicillin V (phenoxymethylpenicillin) | Oral |
Spectrum: Narrow - G(+) and a few G(-) cocci
- G(+): Streptococcus pyogenes, S. pneumoniae, Streptococcus viridans, Enterococcus (with aminoglycoside)
- G(-): Neisseria meningitidis, Neisseria gonorrhoeae (if susceptible)
- Others: Treponema pallidum (syphilis), anaerobes (except Bacteroides fragilis)
Used for:
- Streptococcal pharyngitis/tonsillitis
- Pneumococcal pneumonia (susceptible strains)
- Meningococcal meningitis
- Syphilis (Pen G is drug of choice)
- Rheumatic fever prophylaxis
- Enterococcal endocarditis (+ gentamicin)
Note: Does NOT cover beta-lactamase producing Staph aureus (MSSA or MRSA)
Group 2 - Penicillinase-Resistant (Anti-Staphylococcal) Penicillins
| Drug | Route |
|---|---|
| Nafcillin | IV |
| Oxacillin | IV |
| Dicloxacillin | Oral |
| Flucloxacillin | Oral |
| (Methicillin - historical, no longer used) | - |
Spectrum: Narrow - similar to natural penicillins BUT resistant to staphylococcal penicillinase
- G(+): MSSA (Methicillin-Susceptible Staph aureus) - this is their specialty
- Still active against Streptococci
- Do NOT cover MRSA, G(-) rods, or Pseudomonas
Used for:
- MSSA infections: skin/soft tissue (cellulitis, impetigo, folliculitis)
- MSSA bacteremia and endocarditis
- Osteomyelitis caused by MSSA
Group 3 - Aminopenicillins (Broad-Spectrum)
| Drug | Route |
|---|---|
| Ampicillin | IV/IM/Oral |
| Amoxicillin | Oral |
| Amoxicillin + Clavulanate (Augmentin) | Oral |
| Ampicillin + Sulbactam (Unasyn) | IV |
Spectrum: Broader than natural - adds G(-) coverage
- G(+): Streptococci, Enterococcus faecalis
- G(-): Haemophilus influenzae, E. coli, Proteus mirabilis, Salmonella, Shigella, some Klebsiella
- Do NOT cover Pseudomonas
- Hydrolyzed by many beta-lactamases (hence the combo with clavulanate/sulbactam)
- Adding beta-lactamase inhibitor extends to: B. fragilis (anaerobe), beta-lactamase-producing H. influenzae, MSSA
Used for:
- Otitis media (amoxicillin)
- Sinusitis, community-acquired pneumonia
- UTIs (E. coli)
- Oral/dental infections (amoxicillin-clavulanate)
- Cat, dog, human bites (amoxicillin-clavulanate = drug of choice)
- Meningitis (IV ampicillin - Listeria, Group B Strep, E. coli in neonates)
- Enterococcal endocarditis (IV ampicillin)
- Typhoid/Salmonella (ampicillin)
Group 4 - Antipseudomonal (Extended-Spectrum) Penicillins
| Drug | Combination |
|---|---|
| Piperacillin + Tazobactam (Pip-Tazo, Zosyn) | Always used with tazobactam |
| Ticarcillin + Clavulanate |
Spectrum: The broadest penicillin spectrum
- G(+): Streptococci, Enterococcus (variable)
- G(-): Pseudomonas aeruginosa, Klebsiella, E. coli, Proteus, Enterobacter, H. influenzae
- Anaerobes: B. fragilis (covered with tazobactam)
- Do NOT cover MRSA
Used for:
- Hospital-acquired/ventilator-associated pneumonia
- Febrile neutropenia
- Intra-abdominal infections
- Complicated UTIs
- Sepsis in immunocompromised patients
PART 2: CEPHALOSPORINS
Organized by generations - each higher generation shifts spectrum from G(+) toward G(-):
Key rule to remember: As generation number increases → more G(-) coverage, less G(+) coverage (with exception of 5th gen)
1st Generation - "Gram POSITIVE kings"
| Drug | Route |
|---|---|
| Cefazolin | IV/IM |
| Cephalexin (Keflex) | Oral |
| Cefadroxil | Oral |
Spectrum:
- G(+) - Strong: MSSA, Streptococci (NOT MRSA, NOT Enterococcus)
- G(-) - Limited: E. coli, Proteus mirabilis, Klebsiella pneumoniae (the "PEcK" organisms)
- No anaerobes, no Pseudomonas
Used for:
- Skin/soft tissue infections (MSSA, Streptococcal cellulitis)
- Surgical prophylaxis (Cefazolin - most common surgical prophylaxis antibiotic)
- Simple UTIs (E. coli, Klebsiella)
- Streptococcal/MSSA bone and joint infections
2nd Generation - Adds H. influenzae & Moraxella + some anaerobes
| Drug | Notes |
|---|---|
| Cefuroxime | G(-) respiratory coverage |
| Cefaclor | Oral |
| Cefprozil | Oral |
| Cefamandole | |
| Cefoxitin | + anaerobic coverage (B. fragilis) |
| Cefotetan | + anaerobic coverage (B. fragilis) |
Spectrum:
- G(+): Streptococci, MSSA (weaker than 1st gen)
- G(-): H. influenzae, Moraxella catarrhalis, E. coli, Klebsiella, Proteus
- Anaerobes (cefoxitin/cefotetan only): B. fragilis
- No Pseudomonas
Used for:
- Community-acquired pneumonia (S. pneumoniae + H. influenzae + M. catarrhalis)
- Acute otitis media, sinusitis
- Surgical prophylaxis for abdominal/GYN surgery (cefoxitin/cefotetan)
- Pelvic inflammatory disease (PID)
- Mild intra-abdominal infections
3rd Generation - Broad G(-) coverage, less G(+)
| Drug | Notes |
|---|---|
| Ceftriaxone | IV/IM - most commonly used; crosses BBB |
| Cefotaxime | IV - crosses BBB |
| Ceftazidime | IV - ONLY 3rd gen with Pseudomonas coverage |
| Cefdinir | Oral |
| Cefixime | Oral |
| Cefpodoxime | Oral |
| Cefoperazone | Also has some Pseudomonas activity |
Spectrum:
- G(+): S. pneumoniae (moderate), Streptococci - weaker than earlier gens; NO MSSA reliability
- G(-) - Strong: Enterobacteriaceae (E. coli, Klebsiella, Enterobacter, Proteus, Serratia), H. influenzae, N. meningitidis, N. gonorrhoeae
- Ceftazidime only: Pseudomonas aeruginosa (but LOSES most G(+) activity)
- No MRSA, no Enterococcus
Used for:
- Ceftriaxone is a workhorse:
- Bacterial meningitis (H. influenzae, N. meningitidis, susceptible S. pneumoniae)
- Community-acquired pneumonia (severe)
- Late-stage Lyme disease
- Gonorrhea (drug of choice now - IM ceftriaxone)
- Streptococcal endocarditis
- Typhoid/Salmonella
- Ceftazidime:
- Pseudomonal pulmonary infections (cystic fibrosis)
- Post-neurosurgical meningitis
- Febrile neutropenia
4th Generation - Broad spectrum both G(+) and G(-)
| Drug | Notes |
|---|---|
| Cefepime | IV - broad G(+) and G(-) including Pseudomonas |
| Cefpirome | IV |
Spectrum:
- G(+): Similar to ceftriaxone (Streptococci, MSSA) - better than 3rd gen
- G(-): Pseudomonas aeruginosa, Enterobacteriaceae, AmpC beta-lactamase-producing organisms (Enterobacter)
- No MRSA, no Enterococcus
Used for:
- Febrile neutropenia
- Hospital-acquired pneumonia
- Bacteremia
- Complicated UTIs
- Intra-abdominal infections
5th Generation - MRSA coverage (unique!)
| Drug | Notes |
|---|---|
| Ceftaroline (Teflaro) | IV - only beta-lactam that covers MRSA |
| Ceftobiprole | IV |
Spectrum:
- G(+) - Special: MRSA (unique - no other cephalosporin does this), MSSA, Streptococci
- G(-): Similar to 3rd gen Enterobacteriaceae - but NO Pseudomonas
- No Pseudomonas, no Enterococcus
Used for:
- Community-acquired pneumonia
- Skin and soft tissue infections (including MRSA)
- Emerging use: bacteremia
Quick Memory Summary Table
| Class | Key Drugs | Main G(+) | Main G(-) | Special |
|---|---|---|---|---|
| Natural Pen | Pen G, Pen V | Strep, Pneumococcus | N. meningitidis | Syphilis (T. pallidum) |
| Anti-Staph Pen | Nafcillin, Dicloxacillin | MSSA | None | Pen-resistant Staph |
| Aminopenicillins | Ampicillin, Amoxicillin (+BLI) | Strep, Enterococcus | H. flu, E. coli, Salmonella | Dog bites (Augmentin) |
| Anti-Pseudomonal | Pip-Tazo | Strep | Pseudomonas, Enterobacters | Febrile neutropenia |
| Ceph 1st | Cefazolin, Cephalexin | MSSA, Strep | PEcK (limited) | Surgical prophylaxis |
| Ceph 2nd | Cefuroxime, Cefoxitin | Strep, MSSA | H. flu, Moraxella | Cefoxitin: B. fragilis |
| Ceph 3rd | Ceftriaxone, Ceftazidime | S. pneumoniae (weak) | Enterobacteriaceae, N. gonorrhoeae | Ceftazidime = Pseudomonas |
| Ceph 4th | Cefepime | MSSA, Strep | Pseudomonas, AmpC | Broad both sides |
| Ceph 5th | Ceftaroline | MRSA | Enterobacteriaceae | Only beta-lactam vs MRSA |
The Big "Gaps" - What These Drugs NEVER Cover
- MRSA - only ceftaroline (5th gen) covers it; all other penicillins/cephalosporins fail
- Enterococcus faecium (VRE) - not covered by cephalosporins; aminopenicillins cover faecalis
- Atypicals (Mycoplasma, Chlamydia, Legionella) - no beta-lactam covers these
- Listeria - cephalosporins don't work; use ampicillin
Sources: Harrison's Principles of Internal Medicine 22E, Dermatology 2-Volume Set 5e, Sherris & Ryan's Medical Microbiology 8th Ed, Goodman & Gilman's Pharmacological Basis of Therapeutics
THANKS now can u help me withother beta lactam drugs- azertreonam, imipenem, droeipenem, meropenem, ertapenem, and other cell wall or membrane active agents - vancomycin, fosfomycin, daptomycin, bacitracin, cycloserine please use katzung
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I have all the information needed. Let me now compile the full organized response directly from Katzung.
Other Beta-Lactams + Cell Wall/Membrane-Active Agents
(Katzung's Basic and Clinical Pharmacology, 16th Edition)
PART 1: OTHER BETA-LACTAM DRUGS
A. MONOBACTAMS - Aztreonam
| Feature | Detail |
|---|---|
| Mechanism | Binds transpeptidases - inhibits cell wall synthesis (same as other beta-lactams) |
| Ring structure | Monocyclic beta-lactam ring (mono = one ring, unlike penicillins/cephalosporins which are bicyclic) |
| Spectrum | G(-) ONLY - no G(+), no anaerobes |
Bacteria covered (G- only):
- Pseudomonas aeruginosa
- Enterobacteriaceae (E. coli, Klebsiella, Proteus, Serratia, Enterobacter)
- H. influenzae, N. gonorrhoeae, N. meningitidis
- Similar gram-negative spectrum to 3rd-gen cephalosporins
Bacteria NOT covered:
- All G(+) organisms (zero activity)
- All anaerobes
- Resistant to many beta-lactamases EXCEPT AmpC and ESBLs
Clinical uses:
- Serious G(-) infections: pneumonia, meningitis, sepsis
- Key advantage: safe in patients with penicillin allergy (no cross-reactivity with penicillins)
- Caution: potential cross-reactivity with ceftazidime (structurally similar) - avoid if severe ceftazidime allergy
Route/Dosing: IV, 1-2g every 8 hours (half-life 1-2 hours, prolonged in renal failure)
B. CARBAPENEMS
All carbapenems are beta-lactams with the widest spectrum of all - they resist most beta-lactamases.
Shared mechanism: Bind penicillin-binding proteins (PBPs), inhibit transpeptidation - bactericidal
What carbapenems cover (shared):
- G(+): Streptococci, MSSA, many pneumococci (including pen-non-susceptible strains)
- G(-): Almost all Enterobacteriaceae (E. coli, Klebsiella, Proteus, Enterobacter, Serratia), H. influenzae
- Anaerobes: Bacteroides fragilis and most others
- Highly active vs ESBL-producing organisms and Enterobacter (resistant to their beta-lactamase)
What NO carbapenem covers:
- MRSA
- Enterococcus faecium (VRE)
- Clostridioides difficile
- Burkholderia cepacia, Stenotrophomonas maltophilia
- Carbapenem-resistant Enterobacterales (CRE - carbapenemase producers)
1. Imipenem-Cilastatin
| Feature | Detail |
|---|---|
| Extra coverage | Pseudomonas aeruginosa, Acinetobacter |
| Special note | Inactivated by renal dehydropeptidases - must be combined with cilastatin (a renal dehydropeptidase inhibitor) to prevent renal degradation |
| CSF penetration | Yes - can treat meningitis |
| Route/Dose | IV, 0.25-0.5g every 6-8 hours |
| Half-life | 1 hour |
| Key toxicity | Seizures (most common among carbapenems - especially in renal failure when drug accumulates) |
| Cross-allergy | <1% cross-reactivity with penicillin allergy |
2. Meropenem (+ Meropenem-Vaborbactam)
| Feature | Detail |
|---|---|
| Coverage | Same broad spectrum as imipenem; slightly more active vs G(-), slightly less active vs G(+) |
| Pseudomonas | Yes - covered |
| Acinetobacter | Yes - covered |
| Special note | NOT degraded by renal dehydropeptidase - no cilastatin needed |
| CSF penetration | Yes |
| Route/Dose | IV, 0.5-1g every 8 hours |
| Seizure risk | Much lower than imipenem |
| Meropenem-Vaborbactam | Vaborbactam is a beta-lactamase inhibitor added to restore activity against KPC-producing CRE (carbapenemase producers) |
3. Ertapenem
| Feature | Detail |
|---|---|
| Key difference | Does NOT cover Pseudomonas aeruginosa or Acinetobacter - use other carbapenems for these! |
| Coverage | G(+), G(-) Enterobacteriaceae, anaerobes - same as others minus Pseudomonas/Acinetobacter |
| Special note | NOT degraded by renal dehydropeptidase - no cilastatin needed |
| CSF penetration | No - limited CNS penetration |
| Half-life | Longer - allows once-daily dosing |
| Uses | Community-acquired infections, ESBL infections, intra-abdominal, complicated UTI, pelvic infections - where Pseudomonas is NOT a concern |
4. Doripenem
- Similar to imipenem and meropenem in spectrum (broad, including Pseudomonas)
- Slightly greater G(-) activity, slightly less G(+) than imipenem
- NOT degraded by renal dehydropeptidase
- No longer available in the USA (withdrawn from market)
Carbapenem Comparison at a Glance
| Drug | Pseudomonas | Acinetobacter | Needs Cilastatin | CSF | Seizure Risk |
|---|---|---|---|---|---|
| Imipenem | ✅ | ✅ | YES | ✅ | High |
| Meropenem | ✅ | ✅ | No | ✅ | Low |
| Ertapenem | ❌ | ❌ | No | ❌ | Low |
| Doripenem | ✅ | ✅ | No | ✅ | Low |
PART 2: CELL WALL & MEMBRANE-ACTIVE AGENTS
C. VANCOMYCIN (Glycopeptide)
Mechanism: Binds the D-Ala-D-Ala terminus of nascent peptidoglycan - blocks transglycosylase, preventing peptidoglycan elongation and cross-linking. Also damages the cell membrane. Bactericidal for G(+).
Why only G(+)? Vancomycin is a large molecule - it cannot penetrate the outer membrane of gram-negative bacteria.
Spectrum - G(+) only:
- MRSA (methicillin-resistant S. aureus) - this is its main indication
- MSSA, S. epidermidis
- Streptococcus pneumoniae (including pen-resistant strains)
- Enterococcus faecalis and faecium (but note VRE resistance)
- Clostridioides difficile (oral only, for CDI colitis)
- Most gram-positive anaerobes
Resistance (VRE): Enterococci modify D-Ala-D-Ala to D-Ala-D-Lac - vancomycin can no longer bind.
Clinical uses:
- MRSA infections (bacteremia, endocarditis, pneumonia, osteomyelitis, meningitis)
- Serious G(+) infections in penicillin-allergic patients
- C. difficile colitis (oral route - since it's not absorbed, stays in gut)
- Surgical prophylaxis when MRSA is a concern
Pharmacokinetics:
- Poorly absorbed orally - IV for systemic, oral only for gut infections (CDI)
- CSF penetration 7-30% with meningeal inflammation
- Renally cleared - dose adjust in renal failure
- Monitoring: AUC/MIC ratio ≥400 preferred (or traditional trough monitoring)
Toxicities:
- Nephrotoxicity (especially with aminoglycosides)
- "Red Man Syndrome" - flushing, erythema, hypotension from histamine release during rapid infusion (slow infusion prevents this - not a true allergy)
- Ototoxicity (rare)
D. DAPTOMYCIN (Lipopeptide)
Mechanism: Cyclic lipopeptide from Streptomyces roseosporus. Binds the bacterial cell membrane via calcium-dependent insertion of its lipid tail → depolarizes the membrane → potassium efflux → rapid cell death. Distinct mechanism from all cell-wall agents.
Spectrum - G(+) only:
- MRSA (including MRSA strains with reduced vancomycin susceptibility - VISA/VRSA)
- VRE (Enterococcus faecalis and faecium)
- Streptococcus spp., Staphylococcus spp.
- More rapid bactericidal activity than vancomycin
Clinical uses:
- Skin and soft tissue infections: 4 mg/kg IV once daily
- S. aureus bacteremia and right-sided endocarditis: 6 mg/kg IV once daily
- VRE infections
KEY CONTRAINDICATION: Do NOT use for pneumonia - daptomycin is inactivated by pulmonary surfactant. Use something else for lung infections!
Pharmacokinetics:
- IV only - renally cleared
- Dose adjust in renal insufficiency (CrCl <30 mL/min)
Toxicity: Myopathy/rhabdomyolysis - monitor CPK weekly. Hold statins during daptomycin therapy.
E. FOSFOMYCIN
Mechanism: Analog of phosphoenolpyruvate. Inhibits enolpyruvate transferase by binding its cysteine active site - blocks the first step in peptidoglycan synthesis (formation of UDP-N-acetylmuramic acid precursor). Earliest-acting cell wall agent.
Spectrum: Both G(+) and G(-) (at high concentrations ≥125 mcg/mL)
- E. coli, Klebsiella pneumoniae, Enterococcus faecalis
- Achieves high urinary concentrations - ideal for UTIs
Clinical uses:
- Single 3g oral dose for uncomplicated lower UTI in women (its primary indication)
- Limited data supports multi-dose regimens for male UTI/prostatitis
- Safe in pregnancy
- Synergistic with beta-lactams, aminoglycosides, fluoroquinolones
Pharmacokinetics:
- Oral (only form approved in USA) and IV (available elsewhere)
- Oral bioavailability ~40%, excreted unchanged in urine
- Half-life ~4 hours
Resistance: Inadequate drug transport into the cell.
F. BACITRACIN
Mechanism: Cyclic peptide mixture (from Bacillus subtilis). Interferes with dephosphorylation of the lipid carrier that transports peptidoglycan subunits to the growing cell wall - essentially traps the lipid carrier and stops cell wall building.
Spectrum: G(+) only
- Active against Staphylococci, Streptococci, and other gram-positive organisms
- No cross-resistance with other antibiotics
Route: TOPICAL ONLY
- Highly nephrotoxic if given systemically - never given IV/IM
- Poorly absorbed from skin - stays local
Clinical uses:
- Topical skin/wound infections with mixed G(+) flora
- Available as ointment 500 units/g, often combined with polymyxin or neomycin (e.g., Neosporin)
- Do NOT use prophylactically on wounds - commonly causes hypersensitivity reactions
G. CYCLOSERINE
Mechanism: Structural analog of D-alanine. Inhibits two enzymes:
- Alanine racemase - converts L-alanine to D-alanine
- D-alanyl-D-alanine ligase - joins two D-alanines
Result: D-alanine cannot be incorporated into the peptidoglycan pentapeptide - cell wall synthesis fails.
Spectrum: Active against many G(+) and G(-) organisms, BUT used almost exclusively for:
- Tuberculosis (TB) - specifically MDR-TB (multi-drug resistant TB) caused by Mycobacterium tuberculosis resistant to first-line agents
- Second-line TB drug
Clinical use:
- MDR-TB treatment
- Dose: 0.5-1g/day in 2-3 divided doses
- Blood levels reach 20-30 mcg/mL after 0.25g dose - sufficient to inhibit mycobacteria
Pharmacokinetics:
- Oral, well absorbed
- Widely distributed in tissues including CSF
- Mostly excreted unchanged in urine
Toxicities - CNS (dose-related, serious):
- Headaches, tremors
- Acute psychosis
- Convulsions/seizures
- Keep dose below 0.75g/day to minimize CNS effects
Master Summary Table
| Drug | Class | G(+) | G(-) | Pseudomonas | Anaerobes | Key Use | Key Toxicity |
|---|---|---|---|---|---|---|---|
| Aztreonam | Monobactam | ❌ | ✅ | ✅ | ❌ | G(-) infections in pen-allergic pts | Minimal; cross-react w/ ceftazidime |
| Imipenem | Carbapenem | ✅ | ✅ | ✅ | ✅ | Serious mixed/resistant infections | Seizures, needs cilastatin |
| Meropenem | Carbapenem | ✅ | ✅ | ✅ | ✅ | Serious infections, meningitis | Low seizure risk |
| Ertapenem | Carbapenem | ✅ | ✅ | ❌ | ✅ | Community ESBL infections | No Pseudo coverage! |
| Doripenem | Carbapenem | ✅ | ✅ | ✅ | ✅ | Off market in USA | - |
| Vancomycin | Glycopeptide | ✅ MRSA/VRE | ❌ | ❌ | G(+) only | MRSA, CDI (oral) | Nephro, Red Man Syndrome |
| Daptomycin | Lipopeptide | ✅ MRSA/VRE | ❌ | ❌ | ❌ | MRSA bacteremia, VRE | Myopathy; NOT for pneumonia |
| Fosfomycin | Phosphonate | ✅ | ✅ | ❌ | ❌ | Uncomplicated UTI (single dose) | Minimal |
| Bacitracin | Cyclic peptide | ✅ | ❌ | ❌ | ❌ | Topical skin only | Nephrotoxic if systemic |
| Cycloserine | D-Ala analog | ✅ | ✅ | ❌ | ❌ | MDR-TB only | Seizures, psychosis |
Source: Katzung's Basic and Clinical Pharmacology, 16th Edition
Two exam pearls to tattoo in your brain:
- Aztreonam = G(-) only beta-lactam - safe in penicillin allergy, structural similarity to ceftazidime is the only concern
- Ertapenem = carbapenem with no Pseudomonas coverage - the one exception in its class
This is a shared conversation. Sign in to Orris to start your own chat.