Neurocysticercosis
Reading File
Finding Sources
Searching PubMed
neurocysticercosis diagnosis treatment
Reading File
Reading File
Reading File
Searching Images
neurocysticercosis MRI brain cyst scolex
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive review of neurocysticercosis (NCC):
Neurocysticercosis (NCC)
Definition & Etiology
Neurocysticercosis is a CNS infection caused by the larval stage (cysticercus) of Taenia solium, the pork tapeworm. It is the most common parasitic disease of the human CNS and the most common cause of symptomatic/acquired epilepsy worldwide.
Humans become infected by ingesting T. solium eggs (not larvae) via:
- Fecal-oral contamination from a tapeworm carrier (including auto-infection)
- Contaminated food or water
The ingested eggs hatch in the intestine → oncospheres penetrate the intestinal wall → disseminate hematogenously → lodge in the CNS, muscles, eye, and subcutaneous tissue → develop into cysticerci over 2–3 months.
Epidemiology
- Endemic in Latin America, sub-Saharan Africa, South and Southeast Asia, Eastern Europe
- Most common cause of adult-onset epilepsy in endemic regions
- Estimated 0.45–1.35 million epilepsy cases due to NCC in Latin America; ~1 million in India; 0.31–4.6 million in Africa
- Increasingly important in the US due to immigration: estimated 1,320–5,050 new cases/year; 33,060 cysticercosis-related hospitalizations from 1998–2011
Life Cycle and Pathophysiology
| Step | Detail |
|---|---|
| Ingestion of eggs | T. solium eggs in contaminated food/water/fecal matter |
| Oncosphere penetration | Hatches in small intestine, crosses intestinal wall |
| Hematogenous spread | Oncospheres travel to CNS, muscle, eye, subcutaneous tissue |
| Cyst formation | Develop into cysticerci (~1 cm) over months |
| Host immune response | Intact cysts cause little inflammation; dying cysts trigger intense edema and seizures |
| Resolution | Degenerating cyst calcifies over 1–2 years |
The BBB normally shields viable cysts from immune attack — when the cyst dies (spontaneously or with treatment), antigen release provokes a perilesional inflammatory response that is the principal cause of symptoms.
Classification by Location
1. Parenchymal NCC (most common)
- Cysts in brain parenchyma, predominantly at the gray-white junction
- Seizures are the dominant presentation
- Over 1–2 years, cysts degenerate → fibrosis → calcification
2. Extraparenchymal NCC
| Form | Characteristics |
|---|---|
| Intraventricular | Most commonly 4th ventricle; causes obstructive hydrocephalus; highly symptomatic |
| Subarachnoid (racemose) | Cysts grow without scolex in the subarachnoid space; aggressive form; arachnoiditis, hydrocephalus, vasculitis, stroke |
| Spinal | Intra- or extramedullary; rare |
| Ocular | Subretinal or vitreous; visual symptoms |
Stages of Cyst Evolution (Critical for Imaging Interpretation)
| Stage | Pathology | CT | MRI | Symptoms |
|---|---|---|---|---|
| Vesicular (viable) | Viable cyst, intact BBB, minimal inflammation | Hypodense cyst, ± scolex dot | CSF-isointense cyst, hypointense scolex | Often asymptomatic |
| Colloidal (degenerating) | Scolex disintegrating, intense edema | Ring-enhancing lesion, edema | Heterogeneous signal, ring enhancement, perilesional edema | Seizures, headache |
| Granular-nodular | Fibrotic retraction | Nodular enhancement | Small enhancing nodule | Seizures decreasing |
| Calcified | Complete involution | Dense calcification | Hypointense nodule on T2* | May still cause seizures via perilesional gliosis |
Clinical Manifestations
Seizures are the most common presentation (50–70%), typically focal with or without secondary generalization, occurring most often during the colloidal (degenerating) stage.
Other features:
- Headache — most common non-seizure symptom
- Increased intracranial pressure — from intraventricular cysts or communicating hydrocephalus
- Focal neurological deficits — depending on cyst location
- Meningitis — subarachnoid NCC; chronic basilar meningitis pattern
- Stroke — vasculitis from subarachnoid cysts
- Cysticercotic encephalitis — rare; massive cyst burden with diffuse cerebral edema; can be fatal if antiparasitics are given prematurely
- Psychiatric symptoms — cognitive decline, dementia (in heavy infection)
- Hydrocephalus — obstructive (intraventricular) or communicating (arachnoiditis)
In 80–90% of parenchymal cases, lesions resolve within 3–6 months; ~20% of patients continue to have seizures requiring ongoing antiepileptic therapy.
Diagnosis
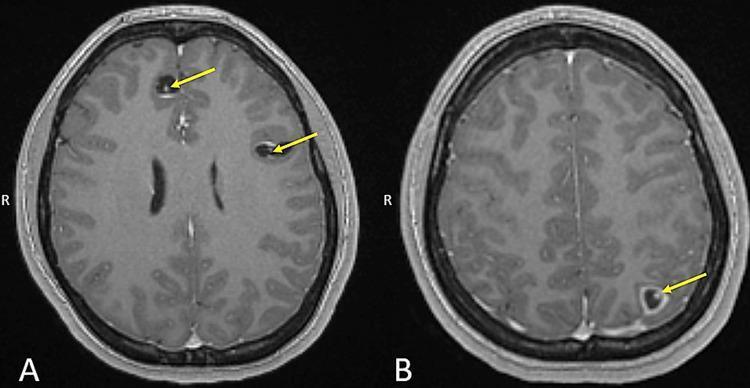
Diagnosis relies on a combination of neuroimaging, serology, clinical history, and exposure context. No single test is pathognomonic, but the "hole-with-dot" sign on MRI (cyst + eccentric scolex) is highly specific.
Neuroimaging
CT findings:
- 1–2 cm cystic lesion with thin walls and a 1–3 mm mural nodule (scolex)
- Ring-like enhancement with surrounding edema
- Calcified lesion (chronic stage)
- Hydrocephalus
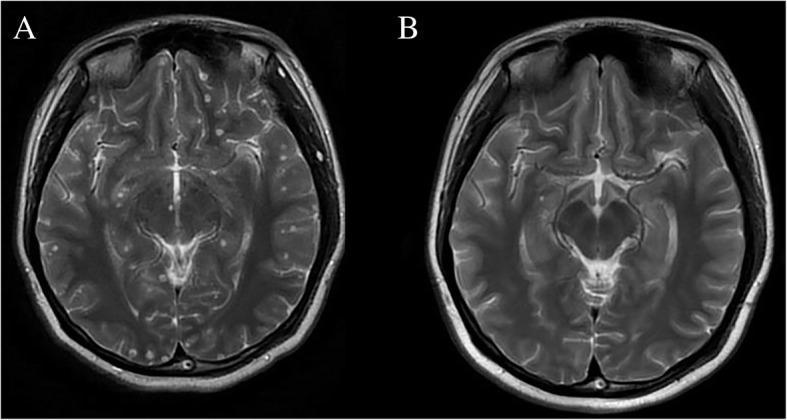
MRI findings (more sensitive):
- Vesicular stage: CSF-isointense cyst, hypointense scolex ("hole-with-dot")
- Colloidal stage: ring enhancement, perilesional edema on FLAIR
- Calcified stage: hypointense on T2/GRE; may have perilesional FLAIR signal in seizure-causing calcifications
Serology
- EITB (enzyme-linked immunoelectrotransfer blot) — most specific serologic test; sensitivity ~94–98% with ≥2 cysts, but only ~50–70% with single cyst or calcified lesion
- ELISA (CSF or serum) — less specific
- CSF pleocytosis (lymphocytic/eosinophilic) with elevated protein in subarachnoid NCC
Del Brutto Diagnostic Criteria
Combines absolute, major, minor, and epidemiological criteria to classify diagnosis as definitive or probable.
Treatment
Treatment must be individualized based on number, location, viability of cysts, and presence of hydrocephalus.
Treatment Table (IDSA/ASTMH 2017 Guidelines)
| Form | Subgroup | Recommendation |
|---|---|---|
| Parenchymal — viable or enhancing (1–2 cysts) | — | Albendazole monotherapy + steroids |
| Parenchymal — viable or enhancing (>2 cysts) | — | Albendazole + praziquantel + steroids |
| Parenchymal — calcified | Any number | No antiparasitic treatment |
| Cysticercotic encephalitis (diffuse edema) | — | No antiparasitic; steroids only |
| Intraventricular — removal feasible | Lateral/3rd ventricle | Neuroendoscopic removal; no medical therapy if successful |
| Intraventricular — removal feasible | 4th ventricle | Neuroendoscopic or microsurgical removal |
| Intraventricular — removal not feasible | — | Ventricular shunt → then antiparasitic + steroids |
| Subarachnoid | ± Hydrocephalus | Shunt if hydrocephalus → prolonged albendazole ± praziquantel |
| Hydrocephalus, no visible cysts | — | Ventricular shunt; no antiparasitic |
| Spinal cysticercosis | — | Surgical removal or antiparasitic + steroids (individualized) |
| Ocular cysticercosis | — | Surgical resection |
Antiparasitic Drugs
Albendazole (drug of choice over praziquantel):
- Dose: 400 mg twice daily for up to 21 days (or 15 mg/kg/day in two divided doses)
- Advantages over praziquantel: shorter course, lower cost, better subarachnoid penetration, drug levels increased (not decreased) by dexamethasone
- Contraindicated in pregnancy, children <2 years, and hepatic cirrhosis
- Drug interactions: dexamethasone and praziquantel increase albendazole levels; phenytoin, phenobarbital, carbamazepine, and ritonavir decrease levels
Praziquantel:
- Used in combination with albendazole for patients with >2 cysts (improves efficacy)
- Levels decreased by dexamethasone and antiepileptic drugs (carbamazepine, phenytoin)
Corticosteroids
- Essential adjunct to antiparasitics to blunt inflammatory response from dying cysts
- Dexamethasone or prednisone; duration tailored to clinical response
- Mandatory when treating subarachnoid/intraventricular NCC (antiparasitics can precipitate acute hydrocephalus)
Antiepileptic Drugs (AEDs)
- All patients with seizures require AEDs
- Monotherapy controls seizures in most
- Duration: typically continued until cyst resolution on imaging; long-term AEDs needed in ~20% who have persistent seizures
Surgery
- Neuroendoscopy: standard approach for intraventricular NCC — avoids need for medical therapy if cyst successfully removed
- VP shunt: for hydrocephalus when cysts are not surgically accessible
- Microsurgery: for fourth-ventricular cysts or selected cases
Prognosis
- Most parenchymal NCC has a favorable prognosis: cysts resolve in 80–90% within 3–6 months; seizures remit in most patients
- Subarachnoid and intraventricular NCC carry higher morbidity and mortality (hydrocephalus, stroke, arachnoiditis)
- Cysticercotic encephalitis is life-threatening; antiparasitics are contraindicated until edema resolves
Prevention
- Access to clean water and sanitation
- Cooking pork thoroughly (cysticerci in muscle killed at 56°C for >5 min)
- Good hand hygiene (to prevent fecal-oral transmission of eggs)
- Treating tapeworm carriers (intestinal taeniasis) in endemic communities
Key sources: Bradley and Daroff's Neurology in Clinical Practice; Tintinalli's Emergency Medicine; Katzung's Basic and Clinical Pharmacology, 16th ed.; Washington Manual of Medical Therapeutics
Recent evidence (2025–2026):
- A 2025 systematic review and meta-analysis (PMID 40381508) supports neuroendoscopic management as the preferred approach for intraventricular NCC, consistent with the IDSA guidelines above.
- A 2026 systematic review (PMID 42087630) on NCC-associated meningitis highlights the aggressive course of subarachnoid/racemose NCC with meningitic complications.
- A 2025 systematic review (PMID 40822429) documents a range of movement disorders as uncommon but recognized manifestations of NCC.
AION
Reading File
Finding Sources
Searching PubMed
"anterior ischemic optic neuropathy"[MeSH Terms]
Reading File
Reading File
Reading File
Searching Images
anterior ischemic optic neuropathy fundus disc edema pallor
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
I have comprehensive data from multiple authoritative sources. Let me now compile the full AION review.
Anterior Ischemic Optic Neuropathy (AION)
Definition
Anterior ischemic optic neuropathy is an infarction or ischemia of the anterior portion of the optic nerve, supplied by the short posterior ciliary arteries (branches of the ophthalmic artery). It is the most frequent cause of optic disc swelling in adults over 50 years and the most common acute optic neuropathy in the older age group.
There are two fundamentally distinct forms:
| Feature | NA-AION (Nonarteritic) | A-AION (Arteritic) |
|---|---|---|
| Cause | Atherosclerosis / vasculopathy | Giant cell (temporal) arteritis |
| Frequency | ~95% of all AION | ~5% (more common in Caucasian females) |
| Age | Usually >40–50 years | Usually >60 years |
| ESR/CRP | Normal | Elevated |
| Visual loss | Moderate to severe | Severe, often catastrophic |
| Disc appearance | Hyperemic or mixed edema | Chalky white pallor (pathognomonic) |
| Premonitory TIAs | Absent | Present in ~10% (amaurosis fugax) |
| Systemic symptoms | Absent | Headache, jaw claudication, PMR, scalp tenderness |
| Treatment | No proven treatment | Emergency high-dose glucocorticoids |
Blood Supply of the Optic Nerve Head
The anterior optic nerve (optic disc and laminar/retrolaminar portion) is supplied by:
- Short posterior ciliary arteries (SPCAs) → form the Circle of Zinn-Haller → supply the prelaminar, laminar, and retrolaminar segments
- The central retinal artery does NOT supply the optic nerve head
Because this is an end-arterial territory with minimal collateral circulation, any compromise in SPCA perfusion leads rapidly to ischemia.
Nonarteritic AION (NA-AION)
Pathophysiology
NA-AION results from a transient hypoperfusion of the SPCAs in a structurally vulnerable optic disc. The mechanism is multifactorial:
- Disc at risk — small, crowded optic disc with a cup-to-disc ratio <0.2 (absent or tiny physiological cup) predisposes to compartment-syndrome-like ischemia when disc edema develops
- Atherosclerotic narrowing of SPCAs → reduced perfusion reserve
- Nocturnal hypotension — many patients note visual loss on awakening; arterial blood pressure dips during sleep reduce optic nerve head perfusion pressure below a critical threshold in a compromised vessel
- Intra-axonal edema → secondary vascular compression within the constrained disc anatomy
Risk Factors
- Systemic: Hypertension, diabetes mellitus, hypercholesterolaemia, ischaemic heart disease, smoking, obstructive sleep apnoea
- Ocular: Small cup-to-disc ratio ("disc at risk") — single strongest local risk factor
- Drug-related: PDE5 inhibitors (sildenafil, etc.) — case reports; causal link uncertain
- Perioperative: Cardiac surgery (CABG), spinal surgery (especially prone positioning) — from hypotension + anaemia + elevated IOP from dependent positioning/fluid overload
- Other: Acute blood loss, antiphospholipid antibody syndrome, collagen vascular disease, migraine
Clinical Features
- Painless, sudden or subacute monocular visual loss — often noticed on awakening
- Altitudinal visual field defect (inferior > superior) — most characteristic; respects horizontal meridian
- Other field defects: arcuate, central, cecocentral, or complete loss
- Relative afferent pupillary defect (RAPD) — present in unilateral or asymmetric cases
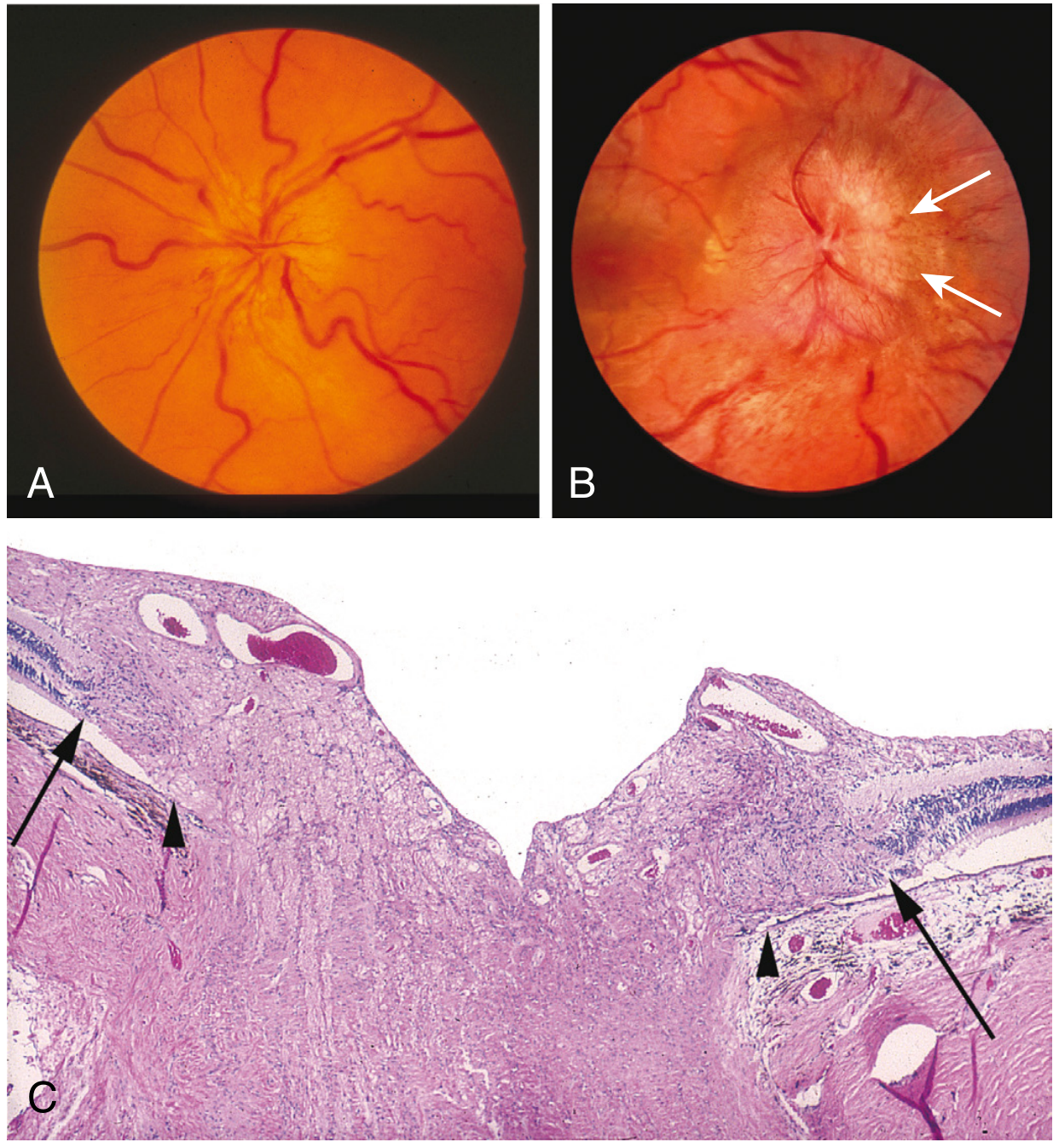
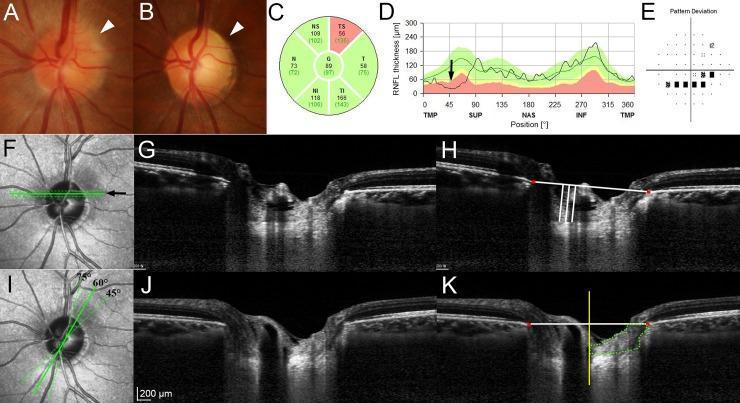
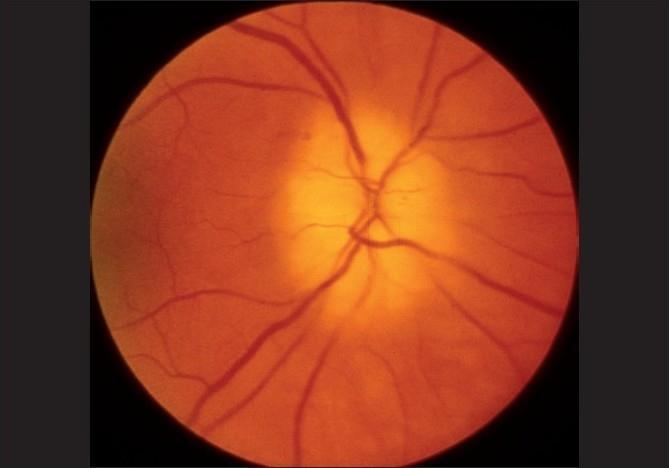
- Optic disc edema — typically pallid (pale) edema in the acute phase, often segmental; may be hyperemic
- Peripapillary splinter (flame-shaped) hemorrhages
- Visual acuity: ranges from mildly reduced to hand motions; often 20/200 or better (less severe than arteritic)
- Fellow eye: shows a "disc at risk" (small cup); risk of AION in second eye is ~15–19% over 5 years
Fundus Images
Course and Prognosis
- Visual loss is usually permanent with subsequent optic atrophy
- 32.6% of patients improve somewhat over a 6-month period
- End-stage disc appearance: segmental or diffuse pallor without significant cupping (unlike arteritic AION, which shows increased cupping)
- Spontaneous improvement is more common in younger patients and diabetics with small enhancing lesions
Treatment — NA-AION
No proven treatment exists. Glucocorticoids are not beneficial in nonarteritic AION and should not be prescribed.
Management focuses on:
- Risk factor modification: optimise blood pressure, glycaemia, lipids; stop smoking
- Avoid nocturnal hypotension: review antihypertensive dosing (avoid over-aggressive evening dosing)
- Aspirin: sometimes used given atherosclerotic aetiology, but no RCT evidence for prevention of fellow eye involvement
- Optic nerve sheath decompression: shown to be ineffective and potentially harmful (Ischemic Optic Neuropathy Decompression Trial)
- Protect the fellow eye — minimise vasculopathic risk factors
Arteritic AION (A-AION) — Giant Cell Arteritis
Pathophysiology
A-AION is caused by granulomatous vasculitis of the SPCAs in the context of giant cell arteritis (GCA). Inflammation leads to thrombotic occlusion → complete infarction of the optic nerve head. Bilateral blindness can occur within hours to days without treatment.
Clinical Features
| Feature | Detail |
|---|---|
| Systemic symptoms | Headache (temporal), scalp tenderness, jaw claudication, fever, weight loss, malaise |
| PMR | Proximal girdle aching and stiffness in ~50% |
| Amaurosis fugax | Transient monocular visual loss in ~10% — critical warning sign |
| Visual loss | Sudden, profound, often complete (counting fingers or worse) |
| Fundus | Chalky white pallor of the optic disc — virtually pathognomonic |
| Bilateral involvement | Without treatment, second eye affected in 25–50% within days to weeks |
| Age | Virtually always >50; typically >60 years |
Investigations
- ESR — typically >50 mm/hr (often >100); may be normal in ~5% of GCA
- C-reactive protein (CRP) — sensitive and specific; elevated in virtually all
- Platelet count — often elevated (reactive thrombocytosis)
- Temporal artery biopsy — mandatory; harvest a long segment (>2 cm) given skip lesions; examine multiple sections. Do NOT delay treatment while awaiting biopsy.
- Biopsy yield: remains positive for ~2 weeks after starting steroids; obtain as soon as practical
- If biopsy is negative by an experienced pathologist, arteritic AION is highly unlikely and glucocorticoids should be tapered
Treatment — A-AION (Emergency)
This is a neuro-ophthalmologic emergency. Treatment must begin immediately upon clinical suspicion — do not wait for biopsy results.
| Agent | Regimen |
|---|---|
| IV methylprednisolone | 1 g/day IV × 3 days (for acute vision-threatening disease or bilateral involvement) |
| Oral prednisolone | 1 mg/kg/day (60–80 mg/day) for less acute presentations; taper slowly over months–years |
| Tocilizumab | 162 mg SC weekly or 8 mg/kg IV every 4 weeks — effective for sustained suppression; reduces steroid exposure; now guideline-endorsed |
| Aspirin | Low-dose aspirin as adjunct (reduces risk of ischaemic complications in GCA) |
Goal: Prevent blindness in the fellow eye — vision lost in the presenting eye rarely recovers significantly, but prompt treatment prevents contralateral involvement.
Posterior ION (PION) — Contrast with AION
PION is uncommon and occurs when the posterior optic nerve is ischaemic without involving the disc:
- Disc appears normal on fundoscopy in acute phase (unlike AION)
- Mainly associated with: severe perioperative anaemia + hypotension (spine/cardiac surgery), shock, massive GI bleeding
- Should always raise suspicion for GCA if disc swelling is absent
- Treatment: reverse anaemia and hypotension immediately; blood transfusion if operative
Differential Diagnosis
| Condition | Key Distinguishing Features |
|---|---|
| Optic neuritis (MS) | Age <45, female, periorbital pain with eye movements, visual loss recovers, normal disc (retrobulbar), responds to steroids |
| Papilledema | Bilateral, disc is hyperemic (not pale), associated with raised ICP, visual acuity preserved early |
| Central retinal artery occlusion | Retinal pallor, cherry-red spot, sudden painless total visual loss, no disc pallor initially |
| Compressive optic neuropathy | Progressive (not sudden), proptosis, pain, normal disc initially |
| Leber hereditary optic neuropathy | Young males, bilateral (sequential), mitochondrial genetics |
Summary: NA-AION vs A-AION at a Glance
| NA-AION | A-AION | |
|---|---|---|
| Aetiology | Vasculopathy + disc at risk | Giant cell arteritis |
| Age | >40 | >60 |
| Visual loss | Variable, often incomplete | Severe, often complete |
| Disc oedema | Hyperaemic or mixed pallor | Chalky white |
| ESR/CRP | Normal | Elevated |
| Systemic Sx | Absent | Headache, jaw claudication, PMR |
| Amaurosis fugax | No | ~10% |
| Treatment | Supportive (risk factors) | Emergency steroids ± tocilizumab |
| Bilateral risk | ~15–19% (5-yr) | 25–50% without Rx |
| Prognosis | Some spontaneous improvement | Poor unless treated immediately |
Key sources: Localization in Clinical Neurology 8e; Harrison's Principles of Internal Medicine 22e; Goldman-Cecil Medicine; Robbins, Cotran & Kumar Pathologic Basis of Disease; Barash's Clinical Anesthesia 9e
This is a shared conversation. Sign in to Orris to start your own chat.