Nephrotic syndrome
Reading File
Finding Sources
Searching PubMed
"nephrotic syndrome"[MeSH Terms] AND management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative sources. Let me compile the full response:
Nephrotic Syndrome
Definition
Nephrotic syndrome is a clinical complex defined by:
| Feature | Threshold |
|---|---|
| Proteinuria | >3.5 g/day (adults); >50 mg/kg/24h or >40 mg/h/m² in children |
| Hypoalbuminemia | Serum albumin <3 g/dL |
| Generalized edema | Periorbital, dependent, anasarca in severe cases |
| Hyperlipidemia | Elevated cholesterol, TG, LDL, VLDL; decreased HDL |
| Lipiduria | Free fat or "oval fat bodies" in urine |
- Robbins Pathologic Basis of Disease
- Harrison's Principles of Internal Medicine 22E (2025)
Pathophysiology
The fundamental defect is increased glomerular capillary wall permeability - a structural or physicochemical disruption in the endothelium, glomerular basement membrane (GBM), or podocytes that allows plasma proteins to escape into the urinary space.
The cascade:
- Glomerular injury → disrupted size/charge barrier → protein leakage into urine
- Proteinuria → depletes serum albumin faster than the liver can compensate → hypoalbuminemia
- Hypoalbuminemia → reduced intravascular oncotic pressure → fluid shifts into interstitium → edema
- Hyperlipidemia - driven by: increased hepatic lipoprotein synthesis, abnormal lipid transport, and decreased lipid catabolism. Lipiduria follows as lipoproteins leak across the glomerular wall
- Sodium retention compounds edema via RAAS activation (hypovolemia-triggered renin → aldosterone), sympathetic stimulation, and reduced atrial natriuretic peptide
Underfill vs. Overfill Edema
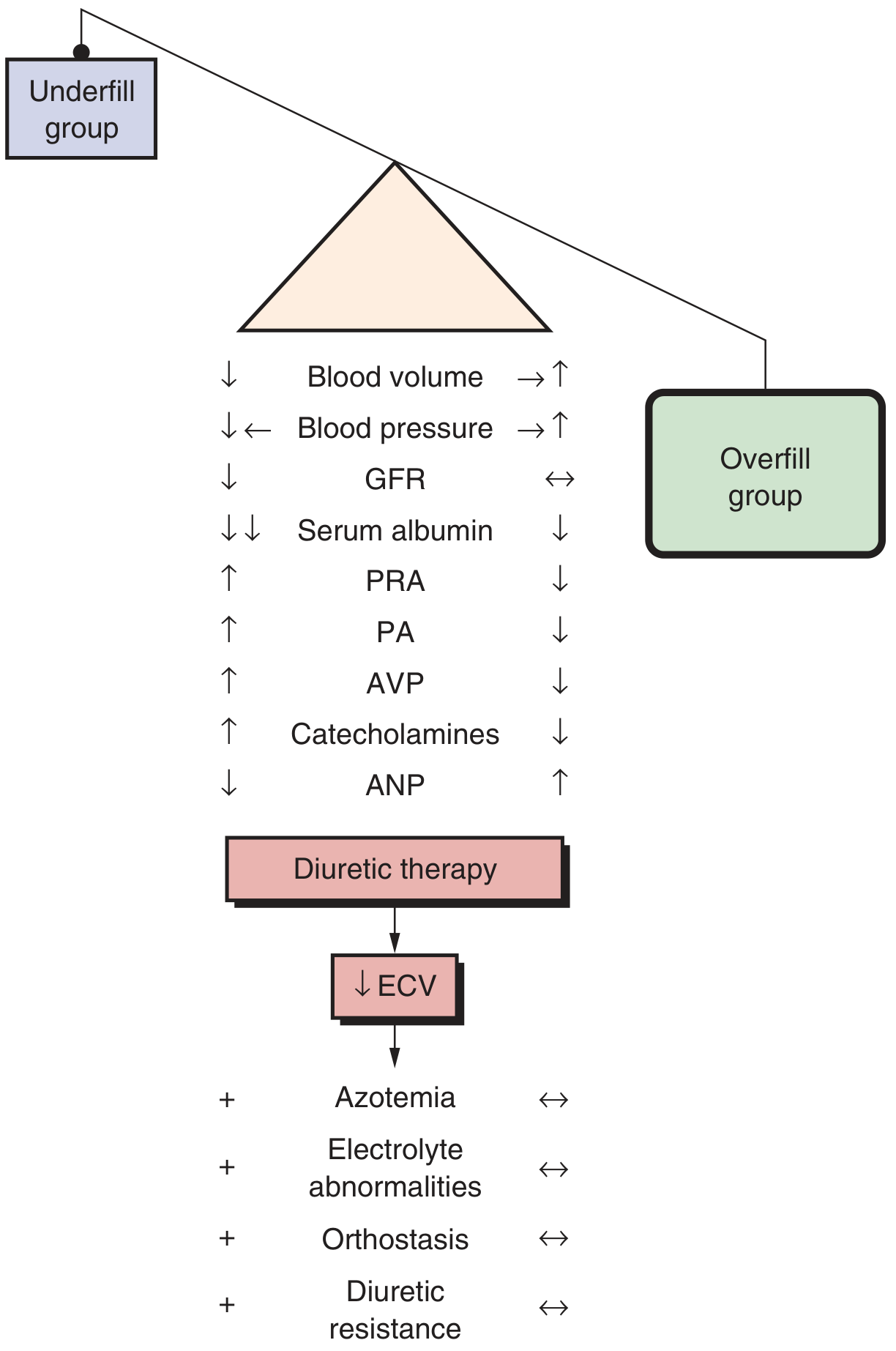
Fig. Comparison of underfill (low plasma volume, high PRA/aldosterone/catecholamines) vs. overfill (expanded plasma volume, suppressed RAAS) edema mechanisms. Minimal change disease classically causes underfill; most other causes cause overfill. - Brenner and Rector's The Kidney
Causes / Classification
Primary (Idiopathic) Glomerular Diseases
| Disease | Key Features | Steroid Response |
|---|---|---|
| Minimal Change Disease (MCD) | Most common in children (70-90%); normal LM, foot process effacement on EM; selective albuminuria | Excellent (90-95% remission in children) |
| Focal Segmental Glomerulosclerosis (FSGS) | Segmental sclerosis of some glomeruli; podocyte injury; circulating permeability factors; nonselective proteinuria | Poor |
| Membranous Nephropathy | In situ immune complex formation (anti-PLA2R antibodies most common); subepithelial deposits; may progress to renal failure | Variable |
| Membranoproliferative GN (MPGN) | GBM thickening + mesangial hypercellularity; immune complex-mediated | Poor |
| C3 Glomerulopathy | Dysregulated complement activation; dense deposit disease | Poor |
Secondary Causes
Medications/Chemicals: Mercury, organic gold, penicillamine, bucillamine, street heroin, probenecid, captopril, NSAIDs, lithium
Infections: HIV, hepatitis B/C, malaria, syphilis, infective endocarditis
Systemic Diseases:
- Diabetes mellitus (most common overall cause globally)
- Systemic lupus erythematosus (lupus nephritis class V)
- Amyloidosis (AL or AA)
- Malignancy (especially solid tumors - see below)
Inherited: Congenital nephrotic syndrome (Finnish type - NPHS1/nephrin mutations; NPHS2/podocin mutations, presenting as FSGS pattern)
- Brenner and Rector's The Kidney; Robbins Pathologic Basis of Disease
Clinical Features
- Edema - characteristically soft, pitting, periorbital (especially in the morning), and dependent. Severe cases progress to pleural effusions, ascites, and anasarca
- Hypertension - present in 30% of children with MCD, up to 50% of adults
- Foamy urine (lipiduria)
- Acellular urinary sediment (in MCD; hematuria more common in FSGS/membranous)
- Decreased GFR in 25-40% of patients, often reversible with treatment
Complications
| Complication | Mechanism |
|---|---|
| Infections | Loss of immunoglobulins in urine; pneumococcal and staphylococcal infections especially dangerous |
| Thromboembolism | Loss of anticoagulant proteins (antithrombin III, protein C/S); increased platelet aggregability; hepatic overproduction of procoagulants. Renal vein thrombosis classic with membranous nephropathy |
| Cardiovascular disease | Persistent hyperlipidemia; all patients with nephrotic hypercholesterolemia should receive lipid-lowering agents |
| Malnutrition | Ongoing protein losses |
| Hypothyroidism | Loss of thyroid-binding globulin → altered thyroid function tests |
| Drug toxicity alterations | Hypoalbuminemia reduces protein binding of drugs (e.g., furosemide, warfarin), expanding volume of distribution |
| AKI | Hypovolemia; interstitial edema (nephrosarca); ATN |
Investigations
- Urinalysis: Proteinuria (dipstick ≥3+), lipiduria, oval fat bodies, fatty casts; typically no RBC casts
- Urine protein:creatinine ratio or 24-hour urine protein
- Serum albumin, total protein - low
- Lipid panel - elevated cholesterol, TGs
- Serum creatinine/eGFR - assess baseline kidney function
- Complement levels (C3, C4) - low in MPGN, lupus; normal in MCD/FSGS/membranous
- ANA, anti-dsDNA - SLE
- Anti-PLA2R antibodies - primary membranous nephropathy (70% sensitivity)
- Hepatitis B/C, HIV serology
- Serum protein electrophoresis (amyloid/myeloma)
- Renal biopsy - required in adults for all new-onset nephrotic syndrome (except diabetics with typical presentation). In children, MCD is presumed and steroids started empirically; biopsy only for non-responders
Management
General (All Causes)
| Intervention | Target |
|---|---|
| Dietary salt restriction | Reduces edema |
| Loop diuretics (furosemide) | Control edema - avoid intravascular volume depletion (especially in underfill patients). Resistance common due to albumin binding; dose adjustment needed |
| ACE inhibitors / ARBs | Reduce proteinuria, counter coagulopathy, dyslipidemia, and progression of CKD |
| SGLT2 inhibitors | Lower urinary protein excretion and preserve kidney function (Harrison's 2025) |
| Statins | All patients with nephrotic hypercholesterolemia |
| Anticoagulation | For thromboembolic complications; prophylaxis in high-risk (serum albumin <2 g/dL + membranous) |
| Vaccinations | Pneumococcal, influenza (due to infection risk) |
Disease-Specific Immunosuppression
Minimal Change Disease:
- First-line: Prednisone (8 weeks; 90-95% remission in children, 80-90% in adults)
- Frequent relapsers / steroid-dependent: Cyclophosphamide, mycophenolate mofetil (MMF), calcineurin inhibitors (CNIs: tacrolimus, cyclosporine), rituximab
- Steroid-resistant: Repeat biopsy (may reveal underlying FSGS)
FSGS:
- Primary FSGS: High-dose steroids (4+ months before declaring resistance); CNIs for steroid-resistant cases; rituximab; voclosporin
- Secondary FSGS: Treat underlying cause; RAAS blockade
Membranous Nephropathy:
- Low-risk: Observation + RAAS blockade
- High-risk or progressive: Rituximab (now first-line immunosuppression per recent evidence); cyclophosphamide + steroids (Ponticelli regimen); CNIs
Diabetic Nephropathy:
- Tight glycemic control; RAAS blockade; SGLT2 inhibitors; finerenone
Prognosis
- MCD: Excellent long-term prognosis; most children enter complete remission. Adults have more delayed response and more resistant relapses
- FSGS: Progressive in many; ~50% reach ESRD within 10 years if untreated; high recurrence rate post-transplant (circulating factor)
- Membranous nephropathy: "Rule of thirds" - 1/3 spontaneous remission, 1/3 partial remission, 1/3 progressive CKD
- Severity correlates with proteinuria: Higher 24-h urine protein = faster GFR decline
Recent Evidence (PubMed, 2024-2025)
A 2025 Cochrane meta-analysis [PMID 40337980] reviewed interventions for idiopathic steroid-resistant nephrotic syndrome in children, noting the ongoing evidence base for calcineurin inhibitors and rituximab in this challenging subgroup. A 2024 systematic review [PMID 38965515] highlighted the association between solid malignancies and nephrotic syndrome, reinforcing the need for malignancy screening in adult-onset nephrotic syndrome, particularly membranous nephropathy.
Sources: Harrison's Principles of Internal Medicine 22E (2025), Robbins Pathologic Basis of Disease, Brenner and Rector's The Kidney, Comprehensive Clinical Nephrology 7th Ed., Frameworks for Internal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.