Insulin analogues ( medicine)
Reading File
Finding Sources
Finding Sources
Searching PubMed
"insulin analogues"[MeSH Terms] AND diabetes
Finding Sources
Searching PubMed
insulin analogues diabetes glycemic control
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive data from Harrison's (2025), Katzung's Pharmacology (16th ed.), and Lippincott's Pharmacology. I have enough to write a thorough, well-organized answer. Let me compose it now.
Insulin Analogues
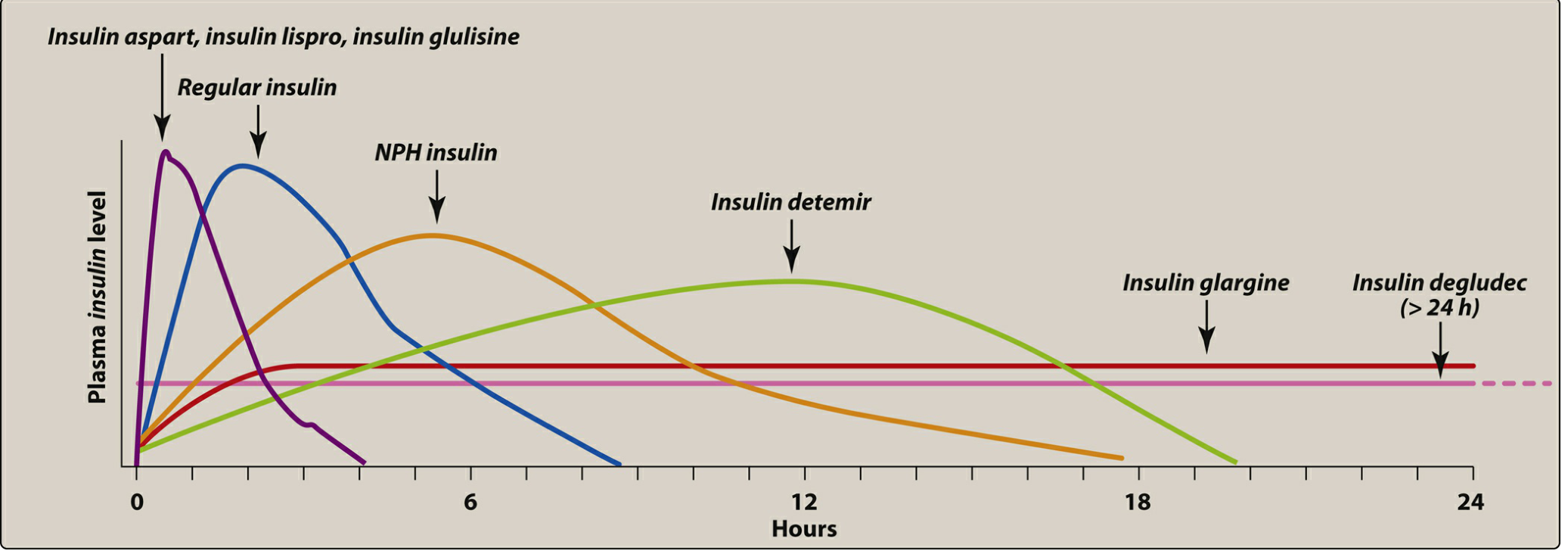
Insulin analogues are genetically engineered modifications of the human insulin molecule. By altering specific amino acids in the A or B chain, manufacturers change the physicochemical properties - and therefore the pharmacokinetics - of the resulting insulin. The goal is to more closely mimic physiologic insulin secretion: a steady low-level "basal" secretion and sharp postprandial "bolus" spikes.
1. Background: Why Analogues Were Developed
Human regular insulin forms hexamers in subcutaneous tissue, which must first dissociate into monomers before absorption - creating a delay of 30-60 minutes before onset and a prolonged tail of action lasting 6-8 hours. This profile does not match the sharp postprandial insulin surge or the flat basal requirement. NPH insulin, while more prolonged, still has an inconvenient peak at 6-7 hours and variable absorption (~25% variability). Analogues were designed to fix both of these shortcomings.
2. Classification and Pharmacokinetics
A. Rapid-Acting Analogues (Prandial)
These are used for mealtime (prandial) coverage - injected 0-15 minutes before or just after starting a meal.
| Agent | Brand Name(s) | Onset | Peak | Duration | Structural Change |
|---|---|---|---|---|---|
| Insulin lispro | Humalog, Admelog, Lyumjev | 5-15 min | 30-90 min | 3-4 h | B-chain: positions 28 (Pro) and 29 (Lys) are reversed |
| Insulin aspart | Novolog, Fiasp | 5-15 min | 30-90 min | 3-4 h | B28 proline replaced by aspartic acid |
| Insulin glulisine | Apidra | 5-15 min | 30-90 min | 3-4 h | B3 Asn → Lys; B29 Lys → Glu |
Key advantage: These modifications reduce self-aggregation, so the analogue exists primarily as monomers/dimers in solution and absorbs rapidly. Absorption variability drops from ~25% (regular) to ~5% (analogues). Duration is consistently ~4 hours regardless of dose - a major advantage over regular insulin.
Fiasp (fast-acting insulin aspart) contains added niacinamide, giving it an even faster onset and offset than standard aspart.
B. Short-Acting (Human Regular Insulin - for comparison)
- Regular insulin (Humulin R, Novolin R): Onset 30-60 min, peak 2-3 h, duration 6-8 h
- Must be injected 30-45 minutes before meals
- Still used IV in DKA management and in insulin pumps when analogues are not available
- U-500 (500 units/mL) formulation used in severe insulin resistance
C. Intermediate-Acting
- NPH insulin (Humulin N, Novolin N): Protamine + zinc are added to regular insulin, forming a suspension that delays absorption. Onset 2-4 h, peak 6-10 h, duration 10-16 h.
- Used as a less expensive basal insulin. Now largely replaced by long-acting analogues in most clinical settings.
- Never administer IV (unlike regular insulin).
D. Long-Acting Analogues (Basal)
These provide a flat, peakless profile that mimics background insulin secretion throughout the day.
| Agent | Brand Name(s) | Onset | Peak | Duration | Structural Change |
|---|---|---|---|---|---|
| Insulin glargine | Lantus, Basaglar, Semglee, Toujeo | 0.5-1 h | Flat (peakless) | ~24 h | A21: Asn → Gly; B-chain C-terminus: +2 Arg residues |
| Insulin detemir | Levemir | 0.5-1 h | Flat | ~17 h | B30 Thr removed; C14 fatty acid chain added (albumin binding) |
| Insulin degludec | Tresiba | 0.5-1.5 h | Flat | >42 h | B30 Thr removed; B-chain C-terminus extended with hexadecanedioyl fatty diacid via linker |
Glargine mechanism: At the acidic pH of the vial (pH 4.0), glargine is soluble. After injection into subcutaneous tissue (physiologic pH ~7.4), it forms microprecipitates from which insulin molecules slowly dissolve. This creates a steady, peakless 24-hour profile. Important: Never mix glargine with other insulins - the acidic pH will alter other formulations.
Detemir mechanism: The fatty acid side chain binds reversibly to albumin in subcutaneous tissue and plasma, creating a depot that slowly releases insulin. Duration is ~17 hours. Note: detemir is now being phased out of the US market.
Degludec mechanism: Forms soluble multihexamers after subcutaneous injection. These slowly dissociate, giving an ultra-long action of >42 hours. This allows once-weekly dosing regimens to be investigated. Compared to glargine, degludec provides similar HbA1c reduction but with less nocturnal and severe hypoglycemia. A newer agent, insulin icodec (once-weekly subcutaneous analogue), is in clinical trials and has shown efficacy comparable to daily glargine - representing the next frontier in basal insulin therapy. [PMID: 38224978]
E. Inhaled Insulin
- Technosphere insulin (Afrezza): Dry powder inhaled via a small device; peak levels in 12-15 min, duration ~3 hours - faster than any injectable rapid-acting analogue.
- Formulations: 4, 8, or 12 unit single-use color-coded cartridges.
- Contraindicated in smokers, asthma, and COPD.
- Requires pre-treatment spirometry.
- Most common side effect: cough (27% of patients), with a small persistent decline in FEV1.
3. Mechanism of Action (All Insulins)
All insulins - both human and analogue - act via the same receptor and pathway:
- Bind the insulin receptor tyrosine kinase on target cells (liver, muscle, adipose)
- Receptor autophosphorylation activates insulin receptor substrate (IRS) proteins
- Downstream signaling via PI3K → Akt promotes:
- Glucose uptake: GLUT4 translocation to cell surface in muscle and fat
- Glycogen synthesis: Activation of glycogen synthase in liver and muscle
- Lipogenesis: Inhibition of lipolysis in adipose
- Protein synthesis: Anti-catabolic effect
- Suppression of hepatic glucose output (gluconeogenesis and glycogenolysis)
4. Clinical Use: Basal-Bolus Strategy
The gold standard of insulin replacement mimics the pancreatic pattern:
- Basal insulin (glargine or degludec once daily, or NPH twice daily) controls fasting glucose and suppresses hepatic glucose output overnight and between meals.
- Prandial (bolus) insulin (lispro, aspart, or glulisine) given with each meal controls postprandial glucose spikes.
This "basal-bolus" regimen is standard of care for Type 1 DM and for insulin-requiring Type 2 DM.
Basal insulin therapy alone (typically glargine or degludec) is often the initial insulin added for Type 2 DM when oral agents are insufficient.
Premixed insulins (e.g., 70/30 NPH/regular, 75/25 protamine-lispro/lispro, 70/30 protamine-aspart/aspart) offer convenience at the cost of flexibility.
Insulin pumps (CSII): Use rapid-acting analogues exclusively, delivering continuous basal rates plus meal boluses. Now combined with continuous glucose monitors (CGM) as automated insulin delivery (AID/"closed-loop" or "artificial pancreas") systems.
5. Concentration Formulations
| Concentration | Agent | Use |
|---|---|---|
| U-100 (100 units/mL) | Standard for most insulins | Routine use |
| U-200 (200 units/mL) | Lispro (Humalog), Degludec | High-dose patients (reduce injection volume) |
| U-300 (300 units/mL) | Glargine (Toujeo) | High-dose patients; slightly longer duration |
| U-500 (500 units/mL) | Regular (Humulin R) | Severe insulin resistance |
6. Adverse Effects
| Effect | Details |
|---|---|
| Hypoglycemia | Most common and serious. Less frequent with analogues vs. human insulin, especially nocturnal hypoglycemia with glargine/degludec vs. NPH |
| Weight gain | Anabolic effect of insulin; common with all formulations |
| Lipodystrophy | Local lipoatrophy or lipohypertrophy at injection sites; rotation prevents this |
| Injection site reactions | Redness, swelling, itching; more common with older animal insulins |
| Insulin allergy | Rare; mediated by anti-insulin IgE; may cause local urticaria or (rarely) anaphylaxis |
| Immune resistance | Anti-insulin IgG antibodies can reduce efficacy (rare with modern analogues) |
| Cough / FEV1 decline | Specific to inhaled insulin (Afrezza) |
7. Special Populations
- Pregnancy: Lispro and aspart are considered safe (Category B evidence). Glargine and degludec are less studied; NPH is traditional first choice for basal coverage in pregnancy. Detemir has the most pregnancy safety data among long-acting analogues.
- Renal impairment: Insulin clearance is reduced; dose reduction required. Degludec's ultra-long action warrants extra caution.
- Pediatrics: Lispro, aspart, and glargine are approved for use in children.
8. Emerging Agents
- Insulin icodec: Once-weekly subcutaneous basal analogue; forms a long-acting depot in the subcutaneous space. Phase 3 trials show non-inferiority to once-daily glargine with similar or fewer hypoglycemic events. [PMID: 38224978]
- Glucose-responsive ("smart") insulins: Under development - these activate only when glucose is elevated, theoretically eliminating hypoglycemia risk. [PMID: 38857114]
- Weekly insulin efsitora alfa: Another once-weekly basal analogue in trials.
Summary Table
| Class | Example | Onset | Peak | Duration | Primary Use |
|---|---|---|---|---|---|
| Rapid-acting analogue | Lispro, Aspart, Glulisine | 5-15 min | 30-90 min | 3-4 h | Prandial (mealtime) |
| Short-acting (human) | Regular | 30-60 min | 2-3 h | 6-8 h | Prandial; IV drips; DKA |
| Inhaled analogue | Afrezza | ~15 min | 1 h | ~3 h | Prandial (inhalation) |
| Intermediate-acting | NPH | 2-4 h | 6-10 h | 10-16 h | Basal (less commonly used now) |
| Long-acting analogue | Glargine | 0.5-1 h | Flat | ~24 h | Basal (once daily) |
| Ultra-long-acting analogue | Degludec | 0.5-1.5 h | Flat | >42 h | Basal (once daily; flexible dosing) |
| Once-weekly (emerging) | Icodec | - | Flat | ~7 days | Basal (weekly) |
Sources:
- Harrison's Principles of Internal Medicine, 22nd Edition (2025), Ch. 416
- Katzung's Basic and Clinical Pharmacology, 16th Edition, Ch. 41
- Lippincott Illustrated Reviews: Pharmacology, Ch. 24
This is a shared conversation. Sign in to Orris to start your own chat.