56 yrs old patient could not able to lie in supine position that position triggers his vertigo
Reading File
Finding Sources
Finding Sources
Searching PubMed
benign paroxysmal positional vertigo diagnosis treatment
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a complete clinical analysis of this patient:
56-Year-Old with Supine-Triggered Vertigo
Most Likely Diagnosis: BPPV - Horizontal (Lateral) Canal Variant
The classic story here is Benign Paroxysmal Positional Vertigo (BPPV). Specifically, a patient who cannot lie supine because that position triggers vertigo points most strongly to the horizontal (lateral) canal variant of BPPV (HC-BPPV), since turning the head in the supine position is the signature trigger for this variant.
Pathophysiology
BPPV results from otoconal debris (calcium carbonate crystals/otoliths) that detach from the otoconal layer and migrate into the semicircular canals:
- Posterior canal BPPV (most common, ~80-90%): Triggered by the Dix-Hallpike maneuver - lying back with head turned to one side. Episodes are brief (<30 seconds) and fatigable.
- Horizontal canal BPPV (~10-15%): Triggered by turning the head side-to-side in the supine position. This is the pattern this patient is describing - even the act of lying flat becomes intolerable.
- Most cases result from cupulolithiasis (debris fixed on the cupula, making it gravity-sensitive) rather than canalithiasis.
- The nystagmus is pure horizontal, has short latency, is not fatigable, and often changes direction with head turns to either side (but this reflects positional change, not a central cause).
As noted in Localization in Clinical Neurology, 8e:
"Vertigo may be induced by turning the head to either side in the supine position and is always more prominent on the pathologic side. The horizontal variant of BPPV resolves faster than the posterior variant."
Why the Patient Avoids Supine
In HC-BPPV, the mere act of lying flat and then turning the head - even slightly during sleep - displaces the cupula-loaded horizontal canal and generates strong vertiginous episodes. Patients learn to sleep semi-reclined or on one specific side to avoid triggering it. - Adams and Victor's Principles of Neurology, 12th Ed.
Diagnostic Approach
Step 1: Dix-Hallpike Test (DHT)
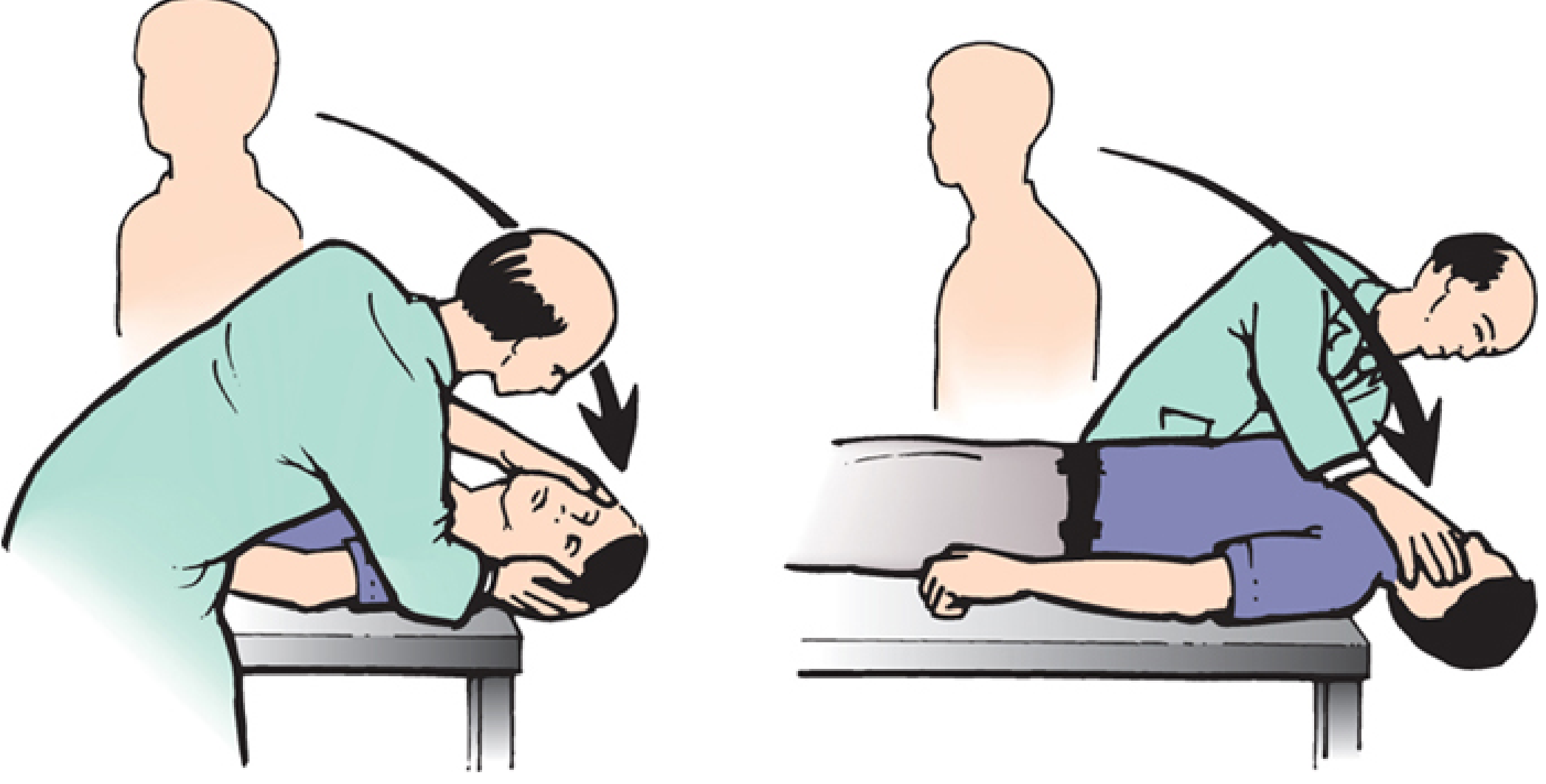
The Dix-Hallpike (Nylén-Bárány) maneuver - patient is moved from sitting to supine with head turned 30-45° to each side.
- Positive in posterior canal BPPV: upbeat-torsional nystagmus after 2-15 sec latency, lasting <30 sec, fatigable
- If negative or shows purely horizontal nystagmus on both sides → proceed to the Supine Roll Test
Step 2: Supine Roll Test (for HC-BPPV)
Procedure:
- Lay the patient flat in the supine position (head does not need to overhang)
- Turn the head 90 degrees to the right, observe for nystagmus and vertigo
- Return to midline, then turn 90 degrees to the left
Positive result: Pure horizontal nystagmus triggered when turning to either side. The affected side is identified by the more intense symptoms and more dramatic nystagmus. - Rosen's Emergency Medicine
Key distinction from central disease: The direction of nystagmus changes with head position (geotropic or apogeotropic), but this is expected in HC-BPPV and is NOT due to gaze direction change - it does not imply a central lesion.
Peripheral vs Central Features - Red Flags to Exclude
| Feature | Peripheral (BPPV) | Central (Worrying) |
|---|---|---|
| Onset | After brief latency (1-15 s) | Immediate |
| Duration | <1 minute | Persistent |
| Fatigability | Present | Absent |
| Nystagmus | Torsional or horizontal | Purely vertical (downbeat), multidirectional |
| Other neuro symptoms | Absent | Diplopia, dysphagia, ataxia, headache |
| Hearing loss | Absent | Variable |
Red flags requiring urgent imaging (MRI brain/posterior fossa):
- Downbeat nystagmus on DHT
- No latency period before nystagmus
- Non-fatigable nystagmus
- Associated neurological symptoms (diplopia, ataxia, dysphagia, headache)
- Chiari malformation features, cerebellar signs
- History of head trauma, or suspicion of posterior fossa tumor
Also consider: vertebrobasilar insufficiency in a 56-year-old - compression of the vertebral artery with head rotation can cause vertigo (look for vascular risk factors). - Bradley and Daroff's Neurology in Clinical Practice
Treatment
For Posterior Canal BPPV (if Dix-Hallpike positive):
Epley Canalith Repositioning Maneuver - first-line treatment.
- 4-5 sequential head rotations, each held 30+ seconds
- The affected ear is the one that is downward when vertigo is elicited on DHT
- Success rate ~80-90% in a single session
- Do NOT prescribe vestibular suppressants for episodes lasting <2 minutes
For Horizontal Canal BPPV (if Supine Roll Test positive):
Gufoni Maneuver - the particle repositioning maneuver for HC-BPPV. A 2024 systematic review (PMID: 38705895) confirms its effectiveness.
Barbecue Roll (360° roll maneuver) - patient rolls from supine toward the unaffected side, 90° at a time, pausing at each position. This is used for the geotropic variant of HC-BPPV.
From Tintinalli's Emergency Medicine:
"Horizontal canal BPPV is rarer, resolves spontaneously more quickly, and is more difficult to assess and treat than posterior canal BPPV. Thus, it is reasonable to refer the patient with suspected horizontal canal BPPV to a clinician familiar with the diagnosis for further management."
Brandt-Daroff exercises can be added as adjunct home therapy (PMID: 38341824 - 2024 systematic review supports their use).
Summary
| Question | Answer |
|---|---|
| Most likely diagnosis | BPPV - horizontal canal variant |
| Pathomechanism | Cupulolithiasis of horizontal semicircular canal |
| Diagnostic test | Supine Roll Test (positive bilaterally, more intense on affected side) |
| First-line treatment | Gufoni maneuver (or Barbecue roll) |
| If Dix-Hallpike positive instead | Epley maneuver |
| When to image | Red flags present (downbeat nystagmus, neuro deficits, non-fatigable) |
Note on age: At 56 years, also consider Ménière disease (if episodes last 20 min to several hours and are accompanied by tinnitus/hearing loss), vestibular migraine, or, less commonly, a vascular cause. BPPV is most prevalent in patients over 50 and is often idiopathic; it has been associated with osteoporosis and prior head trauma. - Adams and Victor's Principles of Neurology, 12th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.