Arthritis
Arthritis: Overview of All Types - Clinical Deep Dive
1. Osteoarthritis (OA)
Definition & Epidemiology
Classification
| Type | Description |
|---|---|
| Primary (idiopathic) | Appears insidiously as an aging phenomenon; oligoarticular, affects weight-bearing joints |
| Hereditary | Collagen gene defects; inflammatory hand OA (Heberden/Bouchard nodes) runs in families |
| Secondary | Prior cartilage damage from trauma, obesity, hemochromatosis, RA, gout, CPPD, neuropathy, acromegaly |
Pathogenesis
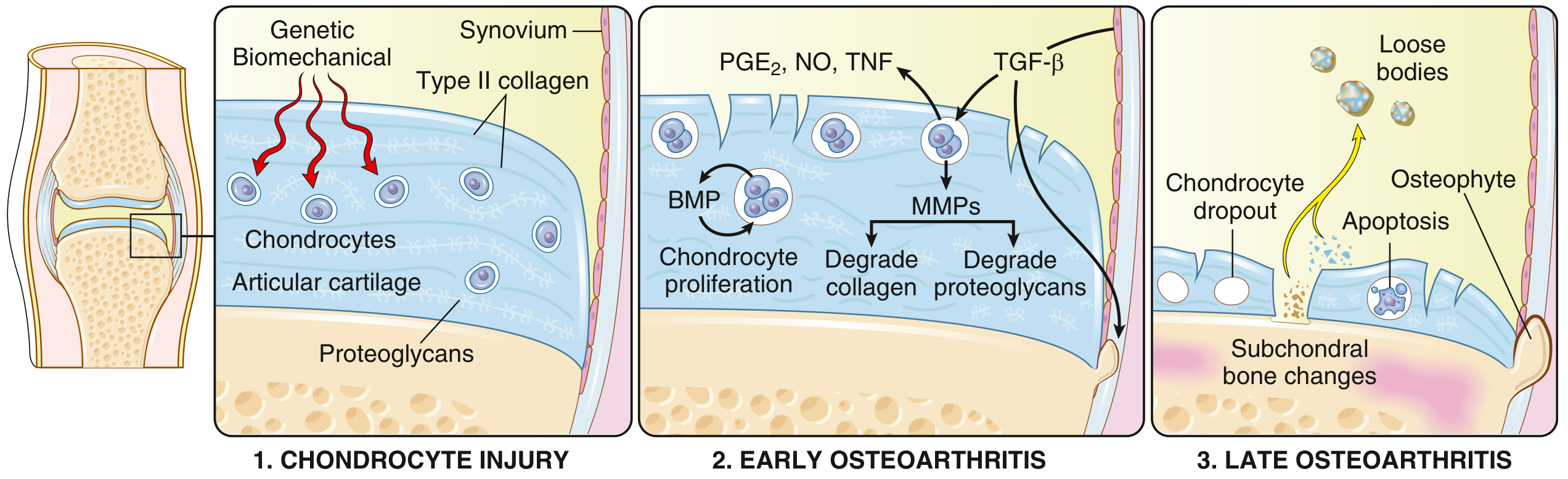
- Chondrocyte injury - Genetic/biomechanical insults damage Type II collagen and proteoglycans
- Early OA - Chondrocytes proliferate and release BMP (repair attempt), but MMPs degrade collagen and proteoglycans; PGE2, NO, TNF drive further damage; degradation exceeds repair
- Late OA - Chondrocyte dropout, apoptosis, subchondral bone changes, osteophyte formation, loose bodies
Clinical Features
- Insidious onset of joint pain, worse with activity, relieved by rest
- Morning stiffness < 30 minutes (vs. > 1 hour in RA)
- Bony enlargement (osteophytes): Heberden nodes (DIP), Bouchard nodes (PIP) in hands
- Crepitus on joint movement
- No systemic features - OA is purely articular
- Most OA is asymptomatic - an incidental radiographic finding
Joints Affected
Investigations
- X-ray: joint space narrowing, osteophytes, subchondral sclerosis, subchondral cysts
- No serologic markers (RF and ANA negative)
- Synovial fluid: non-inflammatory (WBC < 2000/mm³)
Treatment
- Non-pharmacologic: Weight loss (reduces load on joints), low-impact exercise, physiotherapy, assistive devices
- Pharmacologic: NSAIDs are the first-line pharmacologic choice; topical NSAIDs for knee/hand OA; acetaminophen for mild pain; intra-articular corticosteroids for flares
- Surgical: Joint replacement for severe, refractory disease
2. Rheumatoid Arthritis (RA)
Definition & Epidemiology
Pathogenesis
- Genetic: Strong HLA-DR association (HLA-DRB1 "shared epitope"); higher concordance in monozygotic twins
- Trigger: Unknown inciting event (possibly infectious) activates synovial lining cells and subsynovial vessels → pannus formation (aggressive proliferative synovium)
- Immune cascade: Leukocyte invasion, protease and cytokine release (TNF-α, IL-1, IL-6 are key)
- Autoantibodies: Rheumatoid factor (RF) targets IgG Fc; anti-citrullinated peptide antibodies (ACPA/anti-CCP) are more specific and appear years before clinical disease
- Pannus invades and destroys cartilage and bone → ankylosis in late disease
Clinical Features
- Symmetric synovitis of small joints of hands and feet - hallmark
- Morning stiffness > 1 hour
- Constitutional symptoms: fatigue, fever, weight loss
- Progression: Wrists → MCPs → PIPs → knees → ankles → larger joints (spares DIP joints, distinguishing it from OA and psoriatic arthritis)
- Extra-articular manifestations:
- Rheumatoid nodules (subcutaneous, over pressure points)
- Pulmonary: interstitial lung disease, pleural effusion
- Cardiac: pericarditis, accelerated atherosclerosis
- Ocular: scleritis, sicca syndrome
- Vasculitis, neuropathy
- Cervical spine: atlantoaxial subluxation (C1-C2 instability - risk of cord compression)
ACR 1987 Diagnostic Criteria (≥4 of 7, present ≥6 weeks)
- Morning stiffness ≥ 1 hour
- Arthritis of ≥ 3 joint areas
- Arthritis of hand joints (wrists, MCPs, PIPs)
- Symmetric arthritis
- Rheumatoid nodules
- Serum RF positive
- Radiographic erosions/periarticular osteopenia on hand/wrist X-ray
Investigations
- RF: Positive in ~80% of RA; not specific (also positive in SLE, Sjogren's, infection)
- Anti-CCP (ACPA): More specific (~95%), present years before symptoms
- Elevated ESR and CRP
- Synovial fluid: inflammatory (WBC > 2000, often > 50,000/mm³)
- X-ray: periarticular osteopenia → marginal erosions → joint space narrowing
Treatment
- NSAIDs/Corticosteroids: For symptom control and bridging only
- DMARDs (Disease-Modifying Anti-Rheumatic Drugs) - start early:
- Methotrexate - first-line DMARD; most widely used
- Hydroxychloroquine, Sulfasalazine, Leflunomide
- Biologic DMARDs for inadequate DMARD response:
- Anti-TNF agents: etanercept, adalimumab, infliximab
- IL-6 inhibitors: tocilizumab
- B-cell depletion: rituximab
- T-cell co-stimulation blockade: abatacept
- JAK inhibitors (tsDMARDs): tofacitinib, baricitinib
OA vs. RA Comparison
| Feature | Osteoarthritis | Rheumatoid Arthritis |
|---|---|---|
| Primary mechanism | Mechanical injury | Autoimmunity |
| Inflammation | Secondary | Primary |
| Joints | Weight-bearing, DIP | Small joints of hands (MCP, PIP), symmetric |
| Morning stiffness | < 30 min | > 1 hour |
| Pathology | Cartilage degeneration, osteophytes | Pannus, erosions, ankylosis |
| Serology | Negative | RF, anti-CCP positive |
| Systemic involvement | No | Yes (lungs, heart, eyes, etc.) |
3. Gout (Gouty Arthritis)
Definition & Epidemiology
Pathophysiology
- 90% of cases: reduced renal excretion of uric acid
- 10% of cases: overproduction (inborn errors, high purine diet, increased cell turnover)
- Secondary hyperuricemia: diuretics (especially thiazides), low-dose aspirin, cyclosporine, renal failure, myeloproliferative disorders
- MSU crystals trigger intense neutrophil-mediated inflammation
Clinical Stages
- Asymptomatic hyperuricemia - elevated uric acid; no symptoms; takes ~20 years before first attack
- Acute gouty arthritis - sudden onset severe monoarticular pain (often nocturnal); first MTP joint (podagra) in 50% of first attacks, eventually in 75-90% of patients; heels, ankles, knees also affected; self-limited in days to weeks
- Intercritical gout - symptom-free intervals between attacks
- Chronic tophaceous gout - persistent hyperuricemia → tophi (urate deposits in soft tissue, cartilage, ear pinnae), chronic arthritis, joint damage, renal involvement (urate nephropathy, uric acid stones)
Diagnosis
- Definitive: Needle-shaped, negatively birefringent urate crystals on polarized light microscopy of synovial fluid
- Presumptive: clinical features + hyperuricemia + rapid response to NSAIDs/colchicine
- Serum uric acid: usually > 8 mg/dL
- Note: in women and elderly, gout can be polyarticular and mimic RA (tophi mistaken for rheumatoid nodules)
Treatment
| Phase | Treatment |
|---|---|
| Acute attack | NSAIDs (indomethacin), colchicine, corticosteroids |
| Urate-lowering therapy (ULT) | Allopurinol (xanthine oxidase inhibitor) - first line; febuxostat; probenecid (uricosuric) |
| Prophylaxis during ULT initiation | Low-dose colchicine or NSAID for 3-6 months (prevents mobilization flares) |
4. Spondyloarthritis (SpA)
Definition
- Ankylosing Spondylitis (AS) - axial predominant
- Psoriatic Arthritis (PsA)
- Reactive Arthritis (formerly Reiter's syndrome)
- Enteropathic Arthritis (associated with IBD: Crohn's, UC)
Key Features Shared Across SpA
- HLA-B27 association: ~90% of ankylosing spondylitis patients are HLA-B27 positive
- Sacroiliitis and axial involvement
- Enthesitis: inflammation at tendon/ligament insertions (hallmark of SpA - distinguishes from RA)
- Asymmetric oligoarthritis of large joints
- Dactylitis ("sausage digit")
- RF negative (seronegative)
- Eye involvement: uveitis (anterior)
Classification (ASAS)
- Axial SpA (axSpA): back-dominated; subdivided into radiographic (= ankylosing spondylitis, with sacroiliac joint changes on X-ray) and non-radiographic
- Peripheral SpA: peripheral joint-dominated
Ankylosing Spondylitis (AS)
- Chronic inflammatory disease of the spine and sacroiliac joints
- Young men (< 40 years); insidious onset of inflammatory back pain (worse at rest/morning, improved with exercise - opposite of mechanical back pain)
- Eventual fusion of vertebrae ("bamboo spine") on X-ray
- Extra-articular: anterior uveitis, aortitis, apical pulmonary fibrosis, cauda equina syndrome
- Treatment: NSAIDs first-line; physiotherapy; anti-TNF biologics for refractory disease
5. Psoriatic Arthritis (PsA)
- Affects 5-7% of psoriasis patients (up to 40% of hospitalized patients with extensive psoriasis)
- RF usually negative
- Psoriatic skin lesions precede arthritis in 70% of cases; follow in 15%
- Five clinical patterns: oligoarticular asymmetric (most common), symmetric polyarticular (resembles RA), DIP-predominant, axial/spondylitic, arthritis mutilans (most destructive)
- DIP joint involvement and enthesitis distinguish it from RA
- Arthritis mutilans: osteolysis of phalanges/metacarpals → "telescoping fingers"
- X-ray: marginal erosions at DIP/PIP with new bone formation (periostitis) - "pencil-in-cup" deformity
- Treatment: NSAIDs → DMARDs (methotrexate, sulfasalazine) → anti-TNF biologics for axial/refractory disease
6. Reactive Arthritis
- Sterile inflammatory arthritis triggered by a distant infection (usually urogenital - Chlamydia - or enteric - Salmonella, Shigella, Yersinia, Campylobacter)
- Classic triad (Reiter's): arthritis + urethritis + conjunctivitis ("can't see, can't pee, can't climb a tree")
- Asymmetric oligoarthritis of lower limbs; enthesitis; dactylitis; oral ulcers; keratoderma blennorrhagica
- HLA-B27 positive in ~75%
- Usually self-limited (3-12 months); treat with NSAIDs; antibiotics for active infection; DMARDs for chronic cases
7. Septic (Infectious) Arthritis
Definition
Epidemiology & Risk
- Incidence: 2-10/100,000 in native joints; rises to 30-70/100,000 in RA patients
- Risk factors: pre-existing joint disease (OA, RA, gout), IV drug use, immunosuppression, corticosteroids, prosthetic joints
- Most commonly monoarticular: knee (50%), hip (25%), shoulder (15%) in adults
Clinical Features
- Acute onset severe monoarticular pain, warmth, swelling, erythema
- Fever in > 80% of children; only ~40% of adults
- Restricted range of motion (most sensitive sign)
- Position of comfort: slight flexion
Diagnosis
- Joint aspiration is mandatory - synovial fluid: turbid, WBC > 50,000/mm³ (often > 100,000), predominantly neutrophils; Gram stain and culture
- Blood cultures (often positive in hematogenous septic arthritis)
- X-ray: initially normal; MRI for early osteomyelitis or hip involvement
Treatment
- IV antibiotics targeting likely organisms; empirical anti-staphylococcal coverage (vancomycin for MRSA risk)
- Surgical drainage/arthroscopic washout - often required; hip septic arthritis always requires surgical drainage (cannot adequately drain by aspiration alone)
- Duration: typically 2-4 weeks IV → oral antibiotics
Quick Diagnostic Summary Table
| Type | Age/Sex | Joints | Key Lab/Imaging | Hallmark |
|---|---|---|---|---|
| OA | Elderly, F>M after 55 | Knees, hips, DIP | X-ray: osteophytes, JSN | No systemic features; Heberden/Bouchard nodes |
| RA | 20-50, F>>M | MCP, PIP, wrist (symmetric) | RF+, Anti-CCP+, erosions | Symmetric synovitis, > 1 hr morning stiffness |
| Gout | Men 40-60, postmeno F | 1st MTP, ankles, knees | -ve birefringent crystals, ↑uric acid | Podagra; acute severe monoarthritis |
| AS | Young men < 40 | Sacroiliac, spine | HLA-B27+, bamboo spine | Inflammatory back pain, improved with exercise |
| PsA | Any, psoriasis history | DIP, large joints, spine | HLA+ (multiple), pencil-in-cup | Enthesitis, DIP involvement, nail changes |
| Reactive | Young adults | Lower limb, asymmetric | HLA-B27+, preceding infection | Post-infectious; classic triad |
| Septic | Any (peak children/elderly) | Knee > Hip > Shoulder | WBC > 50,000 in joint fluid, +ve culture | Orthopedic emergency; fever + acute monoarthritis |
All ?
Mmm fine do you anle to make pdfs
1 & 2
ls /home/daytona/workspace/ 2>/dev/null && echo "OK"
mkdir -p /home/daytona/workspace/arthritis-pdf && python3 -c "from reportlab.lib…
~/arthritis-pdf/generate_arthritis_pdf.py
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.units import cm
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, PageBreak, KeepTogether
)
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY
from reportlab.platypus import ListFlowable, ListItem
OUTPUT = "/home/daytona/workspace/arthritis-pdf/Arthritis_Clinical_Overview.pdf"
# ── Colour palette ──────────────────────────────────────────────────────────
DARK_BLUE = colors.HexColor("#1A3A5C")
MED_BLUE = colors.HexColor("#2E6DA4")
LIGHT_BLUE = colors.HexColor("#D6E8F7")
ACCENT = colors.HexColor("#E84040")
GOLD = colors.HexColor("#F5A623")
LIGHT_GREY = colors.HexColor("#F2F4F7")
MID_GREY = colors.HexColor("#B0BEC5")
WHITE = colors.white
BLACK = colors.black
# ── Styles ───────────────────────────────────────────────────────────────────
base = getSampleStyleSheet()
def S(name, parent="Normal", **kw):
return ParagraphStyle(name, parent=base[parent], **kw)
styles = {
"cover_title": S("cover_title", "Title",
fontSize=34, textColor=WHITE, leading=42, alignment=TA_CENTER, spaceAfter=6),
"cover_sub": S("cover_sub", "Normal",
fontSize=14, textColor=colors.HexColor("#AED6F1"), alignment=TA_CENTER, spaceAfter=4),
"cover_note": S("cover_note", "Normal",
fontSize=10, textColor=colors.HexColor("#AED6F1"), alignment=TA_CENTER),
"h1": S("h1", "Heading1",
fontSize=18, textColor=WHITE, leading=24, spaceBefore=0, spaceAfter=0,
leftIndent=0),
"h2": S("h2", "Heading2",
fontSize=13, textColor=DARK_BLUE, leading=18, spaceBefore=10, spaceAfter=4,
borderPad=4),
"h3": S("h3", "Heading3",
fontSize=11, textColor=MED_BLUE, leading=15, spaceBefore=6, spaceAfter=3),
"body": S("body", "Normal",
fontSize=9.5, leading=14, spaceAfter=4, alignment=TA_JUSTIFY),
"bullet": S("bullet", "Normal",
fontSize=9.5, leading=13, leftIndent=14, spaceAfter=2),
"table_hdr": S("table_hdr", "Normal",
fontSize=9, textColor=WHITE, leading=12, alignment=TA_CENTER),
"table_cell": S("table_cell", "Normal",
fontSize=8.5, leading=12, alignment=TA_LEFT),
"table_cell_c": S("table_cell_c", "Normal",
fontSize=8.5, leading=12, alignment=TA_CENTER),
"caption": S("caption", "Normal",
fontSize=8, textColor=MID_GREY, alignment=TA_CENTER, spaceAfter=6),
"key_point": S("key_point", "Normal",
fontSize=9, leading=13, textColor=DARK_BLUE,
leftIndent=10, rightIndent=10, spaceAfter=3),
"footer": S("footer", "Normal",
fontSize=7.5, textColor=MID_GREY, alignment=TA_CENTER),
}
PAGE_W, PAGE_H = A4
MARGIN = 2.0 * cm
# ── Helper builders ──────────────────────────────────────────────────────────
def section_header(title, subtitle=""):
"""Coloured banner for a major section."""
data = [[Paragraph(f"<b>{title}</b>", styles["h1"])]]
t = Table(data, colWidths=[PAGE_W - 2*MARGIN])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), DARK_BLUE),
("ROUNDEDCORNERS", [6,6,6,6]),
("TOPPADDING", (0,0), (-1,-1), 10),
("BOTTOMPADDING", (0,0), (-1,-1), 10),
("LEFTPADDING", (0,0), (-1,-1), 14),
]))
elems = [t]
if subtitle:
elems.append(Paragraph(subtitle, styles["body"]))
elems.append(Spacer(1, 6))
return elems
def h2(text):
return [Paragraph(text, styles["h2"]), HRFlowable(width="100%", thickness=1,
color=MED_BLUE, spaceAfter=4)]
def h3(text):
return [Paragraph(text, styles["h3"])]
def body(text):
return [Paragraph(text, styles["body"])]
def bullets(items):
return [Paragraph(f"• {i}", styles["bullet"]) for i in items]
def spacer(h=6):
return [Spacer(1, h)]
def key_box(items, title="Key Points"):
content = [Paragraph(f"<b>{title}</b>", styles["key_point"])]
for i in items:
content.append(Paragraph(f"◆ {i}", styles["key_point"]))
t = Table([[content]], colWidths=[PAGE_W - 2*MARGIN])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), LIGHT_BLUE),
("ROUNDEDCORNERS", [6,6,6,6]),
("TOPPADDING", (0,0), (-1,-1), 8),
("BOTTOMPADDING", (0,0), (-1,-1), 8),
("LEFTPADDING", (0,0), (-1,-1), 10),
("RIGHTPADDING", (0,0), (-1,-1), 10),
("BOX", (0,0), (-1,-1), 1, MED_BLUE),
]))
return [t, Spacer(1, 6)]
def make_table(headers, rows, col_widths=None):
avail = PAGE_W - 2*MARGIN
if col_widths is None:
col_widths = [avail / len(headers)] * len(headers)
hdr_row = [Paragraph(f"<b>{h}</b>", styles["table_hdr"]) for h in headers]
data = [hdr_row]
for row in rows:
data.append([Paragraph(str(c), styles["table_cell"]) for c in row])
t = Table(data, colWidths=col_widths, repeatRows=1)
style = TableStyle([
("BACKGROUND", (0,0), (-1,0), DARK_BLUE),
("ROWBACKGROUNDS",(0,1), (-1,-1), [WHITE, LIGHT_GREY]),
("GRID", (0,0), (-1,-1), 0.4, MID_GREY),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 6),
("RIGHTPADDING", (0,0), (-1,-1), 6),
("VALIGN", (0,0), (-1,-1), "TOP"),
])
t.setStyle(style)
return [t, Spacer(1, 8)]
# ── Page callbacks ────────────────────────────────────────────────────────────
def on_page(canvas, doc):
canvas.saveState()
# Top blue bar
canvas.setFillColor(DARK_BLUE)
canvas.rect(0, PAGE_H - 0.7*cm, PAGE_W, 0.7*cm, fill=1, stroke=0)
canvas.setFillColor(WHITE)
canvas.setFont("Helvetica", 7)
canvas.drawCentredString(PAGE_W/2, PAGE_H - 0.5*cm, "ARTHRITIS — Clinical Overview")
# Bottom bar
canvas.setFillColor(LIGHT_GREY)
canvas.rect(0, 0, PAGE_W, 1.0*cm, fill=1, stroke=0)
canvas.setFillColor(MID_GREY)
canvas.setFont("Helvetica", 7)
canvas.drawString(MARGIN, 0.35*cm, "Sources: Robbins & Kumar Basic Pathology | Textbook of Family Medicine 9e | Goldman-Cecil Medicine | Rosen's Emergency Medicine | Firestein & Kelley's Rheumatology")
canvas.drawRightString(PAGE_W - MARGIN, 0.35*cm, f"Page {doc.page}")
canvas.restoreState()
def cover_page():
from reportlab.platypus import Frame, BaseDocTemplate
# We'll fake a cover with a coloured table
elems = []
# Blue banner fill
cover_data = [[
Paragraph("<b>ARTHRITIS</b>", styles["cover_title"]),
]]
ct = Table(cover_data, colWidths=[PAGE_W - 2*MARGIN])
ct.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), DARK_BLUE),
("TOPPADDING", (0,0), (-1,-1), 40),
("BOTTOMPADDING", (0,0), (-1,-1), 10),
("LEFTPADDING", (0,0), (-1,-1), 20),
("RIGHTPADDING", (0,0), (-1,-1), 20),
("ROUNDEDCORNERS",[8,8,8,8]),
]))
elems.append(ct)
sub_data = [[Paragraph("Clinical Deep-Dive: All Types, Pathology, Diagnosis & Treatment", styles["cover_sub"])]]
st = Table(sub_data, colWidths=[PAGE_W - 2*MARGIN])
st.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), MED_BLUE),
("TOPPADDING", (0,0), (-1,-1), 12),
("BOTTOMPADDING", (0,0), (-1,-1), 12),
("ROUNDEDCORNERS",[0,0,8,8]),
]))
elems.append(st)
elems.append(Spacer(1, 16))
# Type overview boxes
types = [
("1", "Osteoarthritis", "Degenerative", GOLD),
("2", "Rheumatoid Arthritis", "Autoimmune", ACCENT),
("3", "Gout", "Crystal", colors.HexColor("#27AE60")),
("4", "Spondyloarthritis", "Seronegative", MED_BLUE),
("5", "Psoriatic Arthritis", "Seronegative SpA", colors.HexColor("#8E44AD")),
("6", "Reactive Arthritis", "Post-infectious", colors.HexColor("#E67E22")),
("7", "Septic Arthritis", "Infectious/Emergency", ACCENT),
]
box_rows = []
for num, name, tag, col in types:
box_rows.append([
Paragraph(f"<b>{num}</b>", ParagraphStyle("n", fontSize=18, textColor=WHITE, alignment=TA_CENTER)),
Paragraph(f"<b>{name}</b><br/><font size=8 color='#FFFFFF'>{tag}</font>",
ParagraphStyle("t", fontSize=11, textColor=WHITE, leading=15)),
])
for i, (num, name, tag, col) in enumerate(types):
row_data = [[
Paragraph(f"<b>{i+1}</b>", ParagraphStyle("nn", fontSize=16, textColor=WHITE, alignment=TA_CENTER)),
Paragraph(f"<b>{name}</b><br/><font size=8>{tag}</font>",
ParagraphStyle("tt", fontSize=11, textColor=WHITE, leading=15)),
]]
rt = Table(row_data, colWidths=[1.2*cm, PAGE_W - 2*MARGIN - 1.2*cm - 0.2*cm])
rt.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), col),
("TOPPADDING", (0,0), (-1,-1), 8),
("BOTTOMPADDING", (0,0), (-1,-1), 8),
("LEFTPADDING", (0,0), (-1,-1), 10),
("ROUNDEDCORNERS",[6,6,6,6]),
]))
elems.append(rt)
elems.append(Spacer(1, 5))
elems.append(Spacer(1, 20))
note_data = [[Paragraph(
"Sources: Robbins & Kumar Basic Pathology • Textbook of Family Medicine 9e • Goldman-Cecil Medicine • Rosen's Emergency Medicine • Firestein & Kelley's Textbook of Rheumatology",
styles["caption"])]]
nt = Table(note_data, colWidths=[PAGE_W - 2*MARGIN])
nt.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), LIGHT_GREY),
("TOPPADDING", (0,0), (-1,-1), 8),
("BOTTOMPADDING", (0,0), (-1,-1), 8),
("BOX", (0,0), (-1,-1), 0.5, MID_GREY),
]))
elems.append(nt)
elems.append(PageBreak())
return elems
# ── Content ───────────────────────────────────────────────────────────────────
def build_content():
E = []
# ── COVER ─────────────────────────────────────────────────────────────────
E += cover_page()
# ── 1. OSTEOARTHRITIS ─────────────────────────────────────────────────────
E += section_header("1. Osteoarthritis (OA)", "Degenerative Joint Disease — Most Common Arthritis")
E += key_box([
"Most common form of arthritis; affects ~20% of U.S. population.",
"Primarily degenerative — cartilage breakdown with secondary inflammation.",
"Prevalence rises exponentially after age 50; ~40% of people >70 are affected.",
"NSAIDs (not COX-2 inhibitors alone) are first-line pharmacologic treatment.",
])
E += h2("Epidemiology & Classification")
E += body("OA occurs about equally in men and women ages 45–55, but is more common in women after 55. "
"It is found radiographically in almost all 75-year-olds, most of whom are asymptomatic.")
E += make_table(
["Type", "Description", "Examples"],
[
["Primary (Idiopathic)", "Insidious onset; aging phenomenon; oligoarticular", "Knee, hip, lumbar spine OA in the elderly"],
["Hereditary", "Collagen gene defects; inflammatory hand OA runs in families", "Heberden nodes, Bouchard nodes in women"],
["Secondary", "Prior cartilage damage from identifiable cause", "Post-trauma, obesity, hemochromatosis, RA, gout, CPPD, acromegaly, neuropathy"],
],
col_widths=[3.5*cm, 7*cm, 6.5*cm]
)
E += h2("Pathogenesis")
E += body("OA stems from <b>biomechanical stress</b> on articular cartilage, with genetic factors (GDF5, RUNX2, SMAD3 loci) amplifying risk. "
"The process evolves in three stages:")
E += bullets([
"<b>Stage 1 – Chondrocyte Injury:</b> Genetic/biomechanical insults damage Type II collagen and proteoglycans in articular cartilage.",
"<b>Stage 2 – Early OA:</b> Chondrocytes proliferate and release BMP (repair attempt). MMPs degrade collagen and proteoglycans; PGE₂, NO, TNF drive further damage — degradation exceeds repair.",
"<b>Stage 3 – Late OA:</b> Chondrocyte dropout and apoptosis, subchondral bone sclerosis and cysts, osteophyte formation, loose bodies in joint space.",
])
E += h2("Clinical Features")
E += make_table(
["Feature", "Details"],
[
["Onset", "Insidious; pain worsens with activity, relieved by rest"],
["Morning stiffness", "< 30 minutes (key distinction from RA)"],
["Joint involvement", "Weight-bearing: knees, hips, lumbar/cervical spine, 1st MTP, DIP/PIP of hands"],
["Heberden nodes", "Bony enlargement at DIP joints (osteophytes)"],
["Bouchard nodes", "Bony enlargement at PIP joints"],
["Crepitus", "Grating sensation on joint movement"],
["Systemic features", "ABSENT — OA is purely articular"],
["Radiographic findings", "Joint space narrowing, osteophytes, subchondral sclerosis, subchondral cysts"],
],
col_widths=[5*cm, 12*cm]
)
E += h2("Investigations")
E += bullets([
"X-ray: joint space narrowing, osteophytes, subchondral sclerosis/cysts — most important investigation",
"Serology: RF and ANA negative; no specific OA biomarker",
"Synovial fluid: non-inflammatory (WBC < 2,000/mm³); no crystals",
"MRI: best for early cartilage damage (not routine in most cases)",
])
E += h2("Treatment")
E += make_table(
["Category", "Intervention"],
[
["Non-pharmacologic", "Weight loss (reduces joint load), low-impact exercise (swimming, cycling), physiotherapy, quadriceps strengthening, assistive devices (cane, braces)"],
["Pharmacologic — 1st line", "NSAIDs (oral or topical for knee/hand); acetaminophen for mild pain"],
["Pharmacologic — adjuncts", "Intra-articular corticosteroids (short-term flare relief); intra-articular hyaluronic acid (controversial)"],
["Surgical", "Joint replacement (arthroplasty) for severe, refractory disease unresponsive to conservative measures"],
],
col_widths=[4.5*cm, 12.5*cm]
)
E += spacer(8)
# ── 2. RHEUMATOID ARTHRITIS ───────────────────────────────────────────────
E += section_header("2. Rheumatoid Arthritis (RA)", "Chronic Systemic Autoimmune Inflammatory Disease")
E += key_box([
"Affects 1–2% of adults; female predominance 3:1; peak incidence ages 20–50.",
"Symmetric synovitis with morning stiffness >1 hour is the hallmark.",
">70% of polyarticular RF-positive RA patients develop joint erosions within 2 years without treatment.",
"Start DMARDs early — before irreversible joint destruction occurs.",
])
E += h2("Pathogenesis")
E += bullets([
"<b>Genetic:</b> HLA-DRB1 'shared epitope' is the strongest genetic risk factor; higher concordance in monozygotic twins.",
"<b>Trigger:</b> Unknown inciting event (possibly infectious or environmental) in a genetically susceptible host.",
"<b>Pannus formation:</b> Synovial lining cells and subsynovial vessels proliferate → aggressive pannus invades cartilage and bone.",
"<b>Immune cascade:</b> T-cell and B-cell activation; key cytokines TNF-α, IL-1, IL-6 drive inflammation and erosion.",
"<b>Autoantibodies:</b> Rheumatoid factor (RF) targets IgG Fc; Anti-CCP (ACPA) — more specific, detectable years before symptoms.",
])
E += h2("Clinical Features")
E += make_table(
["System", "Manifestations"],
[
["Articular (early)", "Symmetric synovitis of MCPs, PIPs, wrists; spares DIP joints"],
["Articular (late)", "Ulnar deviation, swan-neck/boutonnière deformities, Z-thumb; joint ankylosis"],
["Constitutional", "Fatigue, fever, weight loss, malaise (often precede joint symptoms)"],
["Rheumatoid nodules", "Subcutaneous; over pressure points (olecranon, fingers); indicate seropositive disease"],
["Pulmonary", "Interstitial lung disease, pleural effusion, pulmonary nodules, Caplan syndrome"],
["Cardiac", "Pericarditis, accelerated atherosclerosis (major cause of mortality), valvular disease"],
["Ocular", "Scleritis, episcleritis, sicca syndrome (secondary Sjögren's)"],
["Neurologic", "Atlantoaxial subluxation (C1–C2 instability → spinal cord compression risk), peripheral neuropathy"],
["Haematologic", "Anaemia of chronic disease, Felty syndrome (RA + splenomegaly + neutropenia)"],
],
col_widths=[4.5*cm, 12.5*cm]
)
E += h2("ACR 1987 Diagnostic Criteria (≥4 of 7, symptoms ≥6 weeks)")
E += make_table(
["#", "Criterion", "Definition"],
[
["1", "Morning stiffness", "In and around joints; ≥1 hour before maximal improvement"],
["2", "Arthritis of ≥3 joint areas", "Soft-tissue swelling or fluid in ≥3 joints"],
["3", "Arthritis of hand joints", "Wrists, MCPs, or PIPs involved"],
["4", "Symmetric arthritis", "Simultaneous bilateral involvement"],
["5", "Rheumatoid nodules", "Subcutaneous nodules over bony prominences"],
["6", "Serum RF positive", "Positive by any method in <5% of normal controls"],
["7", "Radiographic changes", "Erosions or periarticular osteopenia on hand/wrist X-ray"],
],
col_widths=[0.8*cm, 5*cm, 11.2*cm]
)
E += h2("Investigations")
E += bullets([
"RF: positive in ~80% of RA; not specific (also positive in SLE, Sjögren's, infections, elderly)",
"Anti-CCP (ACPA): ~95% specific for RA; detectable years before clinical disease",
"Elevated ESR and CRP — reflect inflammatory activity",
"FBC: normocytic anaemia, thrombocytosis in active disease",
"Synovial fluid: inflammatory (WBC >2,000/mm³, often >50,000); no crystals",
"X-ray hands/feet: periarticular osteopenia → marginal erosions → joint space narrowing",
"MRI/Ultrasound: detect early synovitis and erosions before X-ray changes",
])
E += h2("Treatment — Treat-to-Target Strategy")
E += make_table(
["Category", "Agents", "Notes"],
[
["Symptomatic", "NSAIDs, corticosteroids (oral/intra-articular)", "Bridging only; not disease-modifying"],
["Conventional DMARDs (csDMARDs)", "Methotrexate (1st-line), hydroxychloroquine, sulfasalazine, leflunomide", "MTX is anchor drug; combinations used (triple therapy)"],
["Biologic DMARDs — anti-TNF", "Etanercept, adalimumab, infliximab, certolizumab, golimumab", "For inadequate response to csDMARDs"],
["Biologic DMARDs — other", "Tocilizumab (IL-6 inhibitor), rituximab (B-cell), abatacept (T-cell co-stim)", "Alternative biologics depending on profile"],
["Targeted synthetic DMARDs", "Tofacitinib, baricitinib, upadacitinib (JAK inhibitors)", "Oral; used when biologics fail or not tolerated"],
],
col_widths=[3.5*cm, 6*cm, 7.5*cm]
)
E.append(PageBreak())
# ── 3. GOUT ──────────────────────────────────────────────────────────────
E += section_header("3. Gout (Crystal Arthropathy)", "Monosodium Urate Crystal Deposition Disease")
E += key_box([
"Primarily affects men 40–60 years and postmenopausal women.",
"Hyperuricemia (usually >8 mg/dL) is the underlying abnormality — but asymptomatic hyperuricemia is not a disease.",
"Definitive diagnosis: needle-shaped, negatively birefringent crystals on polarized light microscopy.",
"First MTP joint (podagra) involved in 50% of initial attacks; eventually in 75–90% of patients.",
])
E += h2("Pathophysiology")
E += make_table(
["Mechanism", "Details"],
[
["Reduced excretion (90%)", "Renal underexcretion of urate; genetic predisposition + thiazides, low-dose aspirin, cyclosporine, renal failure"],
["Overproduction (10%)", "Inborn errors (HGPRT deficiency — Lesch-Nyhan), high purine diet, myeloproliferative disorders, tumour lysis"],
["Crystal deposition", "MSU crystals form in cooler peripheral joints → phagocytosed by neutrophils → IL-1β release → acute intense inflammation"],
["Tophi", "Chronic urate deposits in soft tissue, cartilage, bone, ear pinnae; indicate years of uncontrolled hyperuricemia"],
],
col_widths=[4.5*cm, 12.5*cm]
)
E += h2("Clinical Stages")
E += make_table(
["Stage", "Features"],
[
["Asymptomatic hyperuricemia", "Elevated uric acid; no symptoms; typically takes ~20 years before first attack"],
["Acute gouty arthritis", "Sudden severe monoarticular pain (often nocturnal); exquisite tenderness; swelling, warmth, erythema; self-limited in days–weeks"],
["Intercritical gout", "Symptom-free intervals; attacks become more frequent and prolonged over time"],
["Chronic tophaceous gout", "Persistent hyperuricemia → tophi; chronic destructive arthritis; renal complications (urate nephropathy, uric acid stones)"],
],
col_widths=[5*cm, 12*cm]
)
E += h2("Diagnosis")
E += bullets([
"<b>Definitive:</b> Needle-shaped, negatively birefringent monosodium urate crystals on polarized light microscopy of synovial fluid or tophi material",
"<b>Presumptive:</b> Clinical features + hyperuricemia + rapid response to colchicine/NSAIDs",
"Serum uric acid: usually >8 mg/dL (note: may be normal during acute attack)",
"Joint aspiration: cloudy fluid, high WBC (polymorphonuclear predominance)",
"X-ray (late disease): punched-out erosions with overhanging edges ('rat bite' erosions), tophi calcifications",
"Note: In women and elderly, gout may be <b>polyarticular</b> and mimic RA; tophi may be mistaken for rheumatoid nodules",
])
E += h2("Treatment")
E += make_table(
["Phase", "Treatment", "Notes"],
[
["Acute attack", "NSAIDs (indomethacin, naproxen), colchicine, corticosteroids (oral/IA)", "Start within 24 hours of attack onset for best effect"],
["Urate-lowering therapy (ULT)", "Allopurinol (xanthine oxidase inhibitor) — 1st line; Febuxostat; Probenecid (uricosuric)", "Target serum uric acid <6 mg/dL (<5 mg/dL in tophaceous gout)"],
["Prophylaxis during ULT initiation", "Low-dose colchicine or NSAID for 3–6 months", "Prevents mobilization flares as urate depots dissolve"],
["Dietary/lifestyle", "Reduce red meat, seafood, fructose-sweetened beverages, alcohol (especially beer); increase hydration", "Address secondary causes: review diuretics, aspirin"],
],
col_widths=[4*cm, 6.5*cm, 6.5*cm]
)
E += spacer(8)
# ── 4. SPONDYLOARTHRITIS ─────────────────────────────────────────────────
E += section_header("4. Spondyloarthritis (SpA)", "HLA-B27 Associated Seronegative Arthritides")
E += key_box([
"Group of related syndromes: ankylosing spondylitis, psoriatic arthritis, reactive arthritis, enteropathic arthritis.",
"HLA-B27 positive in ~90% of ankylosing spondylitis patients.",
"RF negative (seronegative); enthesitis is the pathologic hallmark.",
"Classified as axial SpA (spine/sacroiliac predominant) or peripheral SpA.",
])
E += h2("Common Features Across All SpA Subtypes")
E += make_table(
["Feature", "Description"],
[
["Enthesitis", "Inflammation at tendon/ligament insertions (e.g., Achilles, plantar fascia, iliac crest) — HALLMARK of SpA"],
["Sacroiliitis", "Inflammation of sacroiliac joints; key diagnostic feature on imaging"],
["Asymmetric oligoarthritis", "Typically lower limb large joints (knee, ankle, hip)"],
["Dactylitis", "'Sausage digit' — diffuse swelling of an entire finger/toe; very specific for SpA"],
["Anterior uveitis", "Most common extra-articular feature across SpA subtypes"],
["HLA-B27", "Present in ~90% AS, ~75% reactive arthritis, ~50% psoriatic arthritis with axial disease"],
["RF negative", "Key feature distinguishing SpA from RA"],
],
col_widths=[4*cm, 13*cm]
)
E += h2("Ankylosing Spondylitis (AS)")
E += bullets([
"Chronic inflammatory disease of spine and sacroiliac joints; predominantly young men <40 years",
"<b>Inflammatory back pain:</b> insidious onset, worse at night and in the morning, <b>improved with exercise</b> (opposite of mechanical back pain), relieved poorly by rest",
"Schober test: measures lumbar flexion limitation",
"X-ray: sacroiliitis → 'bamboo spine' (syndesmophytes, spinal fusion) in late disease",
"MRI: detects active sacroiliitis before X-ray changes (bone marrow oedema)",
"Extra-articular: anterior uveitis, aortitis, aortic regurgitation, apical pulmonary fibrosis, cauda equina syndrome",
"<b>Treatment:</b> NSAIDs (first-line) + physiotherapy (mandatory); anti-TNF biologics (adalimumab, etanercept) for refractory disease; IL-17 inhibitors (secukinumab, ixekizumab)",
])
E += spacer(8)
# ── 5. PSORIATIC ARTHRITIS ────────────────────────────────────────────────
E += section_header("5. Psoriatic Arthritis (PsA)", "Seronegative SpA Associated with Psoriasis")
E += key_box([
"Affects 5–7% of psoriasis patients (up to 40% of hospitalised patients with extensive psoriasis).",
"Psoriatic skin lesions precede arthritis in 70% of cases; family history is important when skin lesions absent.",
"DIP joint involvement and enthesitis distinguish PsA from RA.",
"RF usually negative.",
])
E += h2("Clinical Patterns (5 Types)")
E += make_table(
["Pattern", "Features", "Frequency"],
[
["Oligoarticular asymmetric", "Asymmetric involvement of <5 joints; large joints; most common presentation", "~70% (classic)"],
["Symmetric polyarticular", "Resembles RA; multiple small joints; but DIP involved, RF negative", "~15%"],
["DIP-predominant", "Mainly DIP joints; associated with nail disease (pitting, onycholysis)", "~5%"],
["Spondylitic/axial", "Sacroiliitis ± spondylitis; may be asymptomatic radiographically", "~5%"],
["Arthritis mutilans", "Most destructive; osteolysis of phalanges/metacarpals → 'telescoping fingers' (opera glass hand)", "~5%"],
],
col_widths=[4*cm, 9*cm, 4*cm]
)
E += h2("Diagnosis & Treatment")
E += bullets([
"X-ray: marginal erosions at DIP/PIP with periostitis (new bone formation); 'pencil-in-cup' deformity in arthritis mutilans",
"CASPAR criteria used for diagnosis (psoriasis + arthritis + RF negative + imaging findings)",
"<b>Treatment:</b> NSAIDs (1st line) → DMARDs (methotrexate, sulfasalazine) → anti-TNF biologics for axial/refractory disease",
"IL-17 inhibitors (secukinumab) and IL-12/23 inhibitors (ustekinumab) also approved",
"Avoid corticosteroid injections through psoriatic skin (colonised with Staph/Strep)",
])
E += spacer(8)
# ── 6. REACTIVE ARTHRITIS ─────────────────────────────────────────────────
E += section_header("6. Reactive Arthritis", "Post-infectious Sterile Arthritis (formerly Reiter's Syndrome)")
E += key_box([
"Sterile inflammatory arthritis triggered by a distant infection — usually urogenital or enteric.",
"Classic triad: arthritis + urethritis + conjunctivitis ('can't see, can't pee, can't climb a tree').",
"HLA-B27 positive in ~75%; strongly associated.",
"Usually self-limited (3–12 months).",
])
E += h2("Triggering Organisms")
E += make_table(
["Route", "Organisms"],
[
["Urogenital (STI)", "Chlamydia trachomatis (most common in developed countries)"],
["Enteric (food/waterborne)", "Salmonella, Shigella, Yersinia, Campylobacter, Clostridioides difficile"],
],
col_widths=[4*cm, 13*cm]
)
E += h2("Clinical Features & Treatment")
E += bullets([
"Asymmetric oligoarthritis of lower limbs (knees, ankles, feet) 1–4 weeks after infection",
"Enthesitis (Achilles, plantar fascia), dactylitis",
"Mucocutaneous: oral ulcers (painless), keratoderma blennorrhagica (psoriasiform skin lesions on palms/soles), circinate balanitis",
"Ocular: conjunctivitis (mild, bilateral) or anterior uveitis",
"<b>Treatment:</b> NSAIDs for arthritis; antibiotics for active infection (Chlamydia: doxycycline/azithromycin); DMARDs (sulfasalazine, methotrexate) for chronic/recurrent disease",
])
E += spacer(8)
# ── 7. SEPTIC ARTHRITIS ───────────────────────────────────────────────────
E += section_header("7. Septic (Infectious) Arthritis", "Orthopedic Emergency — Prompt Diagnosis Required")
E += key_box([
"Orthopedic emergency: loss of joint function in 25–50% of patients even with prompt treatment.",
"Most common organism: Staphylococcus aureus (all ages).",
"Incidence: 2–10/100,000 in native joints; jumps to 30–70/100,000 in RA patients.",
"Joint aspiration is mandatory for diagnosis — do not delay pending imaging.",
])
E += h2("Pathways & Organisms")
E += make_table(
["Mechanism", "Details"],
[
["Hematogenous (most common)", "Bacteraemia seeds synovial membrane; explains why septic arthritis may coexist with osteomyelitis"],
["Direct inoculation", "Trauma, joint aspiration, or injection"],
["Contiguous spread", "Adjacent osteomyelitis, soft tissue infection"],
],
col_widths=[4.5*cm, 12.5*cm]
)
E += make_table(
["Population", "Common Organisms"],
[
["All adults", "S. aureus (most common), Streptococcus spp."],
["Sexually active young adults", "Neisseria gonorrhoeae (most common cause of septic arthritis in <40 y adults)"],
["IV drug users, immunocompromised", "S. aureus (including MRSA), Gram-negative bacilli (Pseudomonas)"],
["Neonates/infants", "S. aureus, Group B Streptococcus, Gram-negative rods"],
["Prosthetic joint (early <3 months)", "S. aureus, coagulase-negative staph, Gram-negatives"],
],
col_widths=[5*cm, 12*cm]
)
E += h2("Clinical Features")
E += bullets([
"Acute onset severe monoarticular pain; exacerbated by any range of motion",
"Cardinal signs: swelling, erythema, warmth; joint held in position of slight flexion (greatest comfort)",
"Fever >80% of children; only ~40% of adults (especially immunosuppressed/steroid users may have minimal fever)",
"Adults: knee (50%), hip (25%), shoulder (15%)",
"Gonococcal septic arthritis: may present with migratory polyarthralgia → monoarthritis + skin vesiculopustular lesions + tenosynovitis",
])
E += h2("Diagnosis")
E += make_table(
["Investigation", "Expected Findings"],
[
["Joint aspiration (mandatory)", "Turbid fluid; WBC >50,000/mm³ (often >100,000), >90% neutrophils; Gram stain and culture"],
["Blood cultures", "Often positive in hematogenous septic arthritis (draw before antibiotics)"],
["Serum WBC, CRP, ESR", "Elevated but non-specific"],
["X-ray", "Initially normal; useful to exclude fracture; late: joint space loss, osteomyelitis"],
["MRI", "Best for hip septic arthritis; detects osteomyelitis, soft tissue extension"],
["Ultrasound", "Detects joint effusion; guides aspiration (especially hip)"],
],
col_widths=[4.5*cm, 12.5*cm]
)
E += h2("Treatment")
E += bullets([
"<b>IV antibiotics empirically:</b> anti-staphylococcal (flucloxacillin or vancomycin for MRSA risk); adjust to culture/sensitivity",
"<b>Duration:</b> typically 2–4 weeks IV → oral switch; total 4–6 weeks for S. aureus",
"<b>Surgical drainage:</b> hip joint always requires surgical drainage (arthroscopy or open); knee can often be managed with repeated aspiration",
"Gonococcal arthritis: IV ceftriaxone → oral switch; excellent prognosis",
"Physiotherapy: early passive range of motion once infection controlled to prevent ankylosis",
])
E.append(PageBreak())
# ── COMPARISON TABLES ─────────────────────────────────────────────────────
E += section_header("Summary & Comparison Tables", "Quick Reference for Diagnosis and Differentiation")
E += spacer(6)
E += h2("Table 1: Diagnostic Comparison — All 7 Types")
E += make_table(
["Type", "Age/Sex", "Joints Affected", "Key Lab/Imaging", "Hallmark Feature"],
[
["Osteoarthritis", "Elderly; F>M after 55", "Knees, hips, lumbar spine, DIP/PIP", "X-ray: osteophytes, JSN; Serology negative", "No systemic features; Heberden/Bouchard nodes; morning stiffness <30 min"],
["Rheumatoid Arthritis", "20–50 y; F>>M (3:1)", "MCP, PIP, wrists (symmetric); spares DIP", "RF+, Anti-CCP+, ↑ESR/CRP; X-ray erosions", "Symmetric synovitis; morning stiffness >1 hr; systemic features; extra-articular manifestations"],
["Gout", "Men 40–60; postmeno women", "1st MTP (podagra), ankles, knees", "↑Uric acid; −ve birefringent crystals in fluid", "Acute severe monoarthritis; nocturnal onset; podagra; tophi"],
["Ankylosing Spondylitis", "Young men <40", "Sacroiliac joints, spine", "HLA-B27+; MRI sacroiliitis; bamboo spine on X-ray", "Inflammatory back pain improved with exercise; enthesitis; iritis"],
["Psoriatic Arthritis", "Any; psoriasis history", "DIP joints, large joints, axial; asymmetric", "HLA+(multiple); pencil-in-cup deformity; RF neg", "Nail changes (pitting, onycholysis); DIP involvement; enthesitis; dactylitis"],
["Reactive Arthritis", "Young adults post-infection", "Lower limb large joints; asymmetric", "HLA-B27+; cultures of infection trigger", "Post-infectious; classic triad (urethritis, conjunctivitis, arthritis)"],
["Septic Arthritis", "Any (children, elderly, immunocomp)", "Knee > Hip > Shoulder; monoarticular", "Joint fluid WBC >50,000; Gram stain/culture +ve", "Orthopedic emergency; fever; acute severe monoarthritis"],
],
col_widths=[3*cm, 3*cm, 4*cm, 4*cm, 4.5*cm]
)
E += h2("Table 2: OA vs. RA — Head-to-Head Comparison")
E += make_table(
["Feature", "Osteoarthritis", "Rheumatoid Arthritis"],
[
["Primary mechanism", "Mechanical injury to articular cartilage", "Autoimmunity (T-cell and antibody-mediated)"],
["Role of inflammation", "Secondary; exacerbates cartilage damage", "Primary — drives all joint destruction"],
["Joints involved", "Weight-bearing: knees, hips; DIP joints", "Small joints: MCPs, PIPs, wrists (symmetric); spares DIP"],
["Morning stiffness", "<30 minutes", ">1 hour"],
["Systemic involvement", "No", "Yes: lungs, heart, eyes, cervical spine, blood"],
["Serology", "RF, ANA negative", "RF+ in 80%; Anti-CCP+ in ~70% (95% specific)"],
["Pathology", "Cartilage degeneration, osteophytes, subchondral cysts", "Pannus formation, marginal erosions, ankylosis"],
["Synovial fluid", "Non-inflammatory (<2,000 WBC/mm³)", "Inflammatory (>2,000–50,000+ WBC/mm³)"],
["Treatment", "NSAIDs, physiotherapy, joint replacement", "DMARDs (MTX), biologics (anti-TNF, IL-6i, JAKi)"],
],
col_widths=[4.5*cm, 6*cm, 6*cm]
)
E += h2("Table 3: Synovial Fluid Analysis in Arthritis")
E += make_table(
["Category", "WBC/mm³", "Appearance", "Conditions"],
[
["Normal", "<200", "Clear, viscous", "Normal joint"],
["Non-inflammatory", "200–2,000", "Clear/yellow, viscous", "OA, trauma, early SLE"],
["Inflammatory", "2,000–50,000", "Turbid, yellow, low viscosity", "RA, gout, pseudogout, SpA, reactive arthritis"],
["Septic (presumed)", ">50,000 (often >100,000)", "Turbid/purulent, very low viscosity", "Bacterial septic arthritis"],
["Haemorrhagic", "Variable (RBCs)", "Red/bloody", "Trauma, haemophilia, pigmented villonodular synovitis"],
],
col_widths=[3.5*cm, 3.5*cm, 5*cm, 5.5*cm]
)
E += h2("Table 4: Crystal Arthropathies Comparison")
E += make_table(
["Feature", "Gout (MSU)", "Pseudogout (CPPD)"],
[
["Crystal type", "Monosodium urate (MSU)", "Calcium pyrophosphate dihydrate (CPPD)"],
["Birefringence", "Negatively birefringent; needle-shaped", "Weakly positively birefringent; rhomboid-shaped"],
["Common joints", "1st MTP (podagra), ankles, knees", "Knees (most common), wrists, hips"],
["Age/sex", "Middle-aged men; postmeno women", "Elderly; equal sex distribution"],
["X-ray", "Punched-out erosions; tophi calcifications", "Chondrocalcinosis (calcification in cartilage)"],
["Underlying causes", "Hyperuricemia; thiazides, renal failure", "Hyperparathyroidism, haemochromatosis, hypomagnesaemia"],
["Acute treatment", "NSAIDs, colchicine, corticosteroids", "NSAIDs, colchicine, corticosteroids"],
["Long-term treatment", "Allopurinol/febuxostat (urate-lowering)", "No specific crystal-reducing therapy available"],
],
col_widths=[4*cm, 6*cm, 7*cm]
)
E += h2("Table 5: Key Drug Summary in Arthritis Management")
E += make_table(
["Drug/Class", "Mechanism", "Used In", "Key Side Effects"],
[
["NSAIDs", "COX-1/2 inhibition → ↓prostaglandins", "OA, RA, Gout (acute), SpA, PsA, Reactive arthritis", "GI ulcers, renal impairment, CV risk, fluid retention"],
["Colchicine", "Inhibits microtubule polymerisation → ↓neutrophil chemotaxis", "Gout (acute + prophylaxis), CPPD, pericarditis", "GI: diarrhoea, nausea; myopathy (high dose); drug interactions (CYP3A4)"],
["Allopurinol", "Xanthine oxidase inhibitor → ↓uric acid synthesis", "Gout prevention (ULT)", "Rash (SJS in HLA-B*58:01 carriers), hypersensitivity syndrome"],
["Methotrexate", "Folic acid antagonist → anti-inflammatory via adenosine pathway", "RA (1st-line DMARD), PsA, other inflammatory arthritis", "Hepatotoxicity, myelosuppression, mucositis, pneumonitis; folate supplementation required"],
["Anti-TNF biologics", "Block TNF-α (key pro-inflammatory cytokine)", "RA, AS, PsA, IBD-related arthritis", "Infection risk (TB reactivation — screen with IGRA before use), injection site reactions"],
["IL-6 inhibitors (tocilizumab)", "Block IL-6 receptor", "RA (especially with systemic features)", "Infection, dyslipidaemia, liver enzyme elevation; may mask fever"],
["JAK inhibitors (tofacitinib)", "Inhibit JAK1/3 → ↓cytokine signalling", "RA, PsA, AS", "Infection, VTE risk, CV events; avoid in high CV risk patients"],
["Corticosteroids", "Broad anti-inflammatory via glucocorticoid receptor", "Bridging in RA, acute gout, septic arthritis (adjunct in some cases)", "Osteoporosis, hyperglycaemia, adrenal suppression, Cushing's features with prolonged use"],
],
col_widths=[3.5*cm, 4*cm, 4*cm, 5.5*cm]
)
E += spacer(8)
# Sources
sources = [
"Robbins & Kumar Basic Pathology, p. 790 — OA pathogenesis and OA vs RA comparison",
"Textbook of Family Medicine 9e, pp. 873–893 — OA, RA, Gout, PsA, Reactive Arthritis",
"Goldman-Cecil Medicine (International Edition) — Spondyloarthritis (Chapter 244)",
"Rosen's Emergency Medicine — Septic Arthritis (p. 2730)",
"Firestein & Kelley's Textbook of Rheumatology (2-Volume Set) — OA genetics, SpA",
]
E += h2("Sources")
E += bullets(sources)
return E
# ── Build PDF ─────────────────────────────────────────────────────────────────
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
leftMargin=MARGIN,
rightMargin=MARGIN,
topMargin=MARGIN + 0.7*cm,
bottomMargin=MARGIN + 1.0*cm,
title="Arthritis — Clinical Overview",
author="Orris Medical AI",
subject="All types of arthritis: pathology, diagnosis, treatment",
)
story = build_content()
doc.build(story, onFirstPage=on_page, onLaterPages=on_page)
print(f"PDF created: {OUTPUT}")
cd /home/daytona/workspace/arthritis-pdf && python3 generate_arthritis_pdf.py 2>…
ls -lh /home/daytona/workspace/arthritis-pdf/Arthritis_Clinical_Overview.pdf
Arthritis Clinical Overview
PDF Document · PDF
- Cover page with colour-coded index of all 7 types
- 7 clinical sections - OA, RA, Gout, Spondyloarthritis, Psoriatic Arthritis, Reactive Arthritis, Septic Arthritis - each with key points box, pathogenesis, clinical features, investigations, and treatment tables
- 5 summary/comparison tables:
- Diagnostic comparison across all 7 types
- OA vs. RA head-to-head
- Synovial fluid analysis guide
- Gout vs. Pseudogout (crystal arthropathies)
- Key drug summary (NSAIDs, colchicine, allopurinol, MTX, biologics, JAK inhibitors, steroids)
- Sourced from Robbins Pathology, Goldman-Cecil Medicine, Rosen's Emergency Medicine, and Firestein & Kelley's Rheumatology
Unable to download it
ls -lh /home/daytona/workspace/arthritis-pdf/ && echo "---" && python3 -c " with…
python3 -c " import base64 with open('/home/daytona/workspace/arthritis-pdf/Arth…
Arthritis Clinical Overview
PDF Document · PDF
download
HTML File · HTML
- Email it to you - if your platform supports that
- Recreate as a web-viewable format - I can produce the full content as a clean HTML page you can print-to-PDF from your own browser (File → Print → Save as PDF)
- Upload to a file host - if the sandbox has internet outbound access
Thank you I downloaded it
I'm a final year medical student (Sri Lanka- preparing for final exam), I'll give you my references, whenever I ask can you give answers, explanations or notes including important exam aspects, by get adhere to those references and please make sure not make any mistakes. References: Medicine :Kumar and clerk 11th edition Oxford handbook for Medicine Harrison principles of medicine Pead : Illustrated pediatrics Concise peadiatrics(Sri lankan book) Oxford hand book for peadiatrics Surgery : Bailey and love Oxford handbook Gyn & Obs : Oxford hand book for gyn and obs Ten teachers eranthi Madam's book(gyn and obs) --( in Sri Lanka) dutta's textbook of gynecology Psychiatry : Oxford hand book Hanwela sir's book (sri lankan book) Mim's Microbiology Robin's pathology Bennerd and brown's pharmacology And accepted national and other standards updated guidelines for all of them
| Subject | References |
|---|---|
| Medicine | Kumar & Clark 11th ed, Oxford Handbook of Medicine, Harrison's Principles |
| Paediatrics | Illustrated Paediatrics, Concise Paediatrics (SL), Oxford Handbook of Paediatrics |
| Surgery | Bailey & Love, Oxford Handbook of Surgery |
| Gyn & Obs | Oxford Handbook G&O, Ten Teachers, Eranthi Madam's book (SL), Dutta's Gynaecology |
| Psychiatry | Oxford Handbook of Psychiatry, Hanwela Sir's book (SL) |
| Cross-cutting | Mims' Microbiology, Robbins' Pathology, Brenner & Rector's Pharmacology, Current national/international guidelines |
- Content aligned to those references as the primary authority
- Sri Lankan context respected (local guidelines, SL-specific books prioritised where relevant)
- Exam-focused: I'll flag high-yield points, common exam traps, and structured answer formats (SAQ/MCQ style where helpful)
- No guessing - if something is uncertain or outside your references, I'll say so clearly
- PDFs available on request for any topic
Epilepsy
EPILEPSY
Final Year MBBS - Exam Notes | Kumar & Clark | Harrison's | Oxford Handbook of Medicine
DEFINITION
⚠️ Exam Trap: A single seizure is NOT epilepsy. A provoked seizure (e.g., from hypoglycaemia, fever, drugs) is NOT epilepsy.
EPIDEMIOLOGY
- Prevalence: ~1% of the population
- Most common serious neurological disorder
- Bimodal age distribution: peak in childhood and >60 years
- ~30% of patients remain refractory to medical treatment
AETIOLOGY (ILAE Classification)
| Category | Examples |
|---|---|
| Structural | Hippocampal sclerosis (mesial TLE), cortical dysplasia, post-stroke, tumour, trauma, post-encephalitis |
| Genetic | Ion channel mutations (SCN1A in Dravet, KCNQ2); chromosomal (Angelman, Down syndrome) |
| Infectious | Neurocysticercosis (most common cause worldwide), TB, cerebral malaria, HIV encephalopathy |
| Metabolic | Hypoglycaemia, hyponatraemia, hypocalcaemia, uraemia, pyridoxine deficiency |
| Immune | Autoimmune encephalitis (anti-NMDAR, anti-LGI1) |
| Unknown | Majority (~50% of cases) |
⚠️ Exam High-Yield: In Sri Lanka/South Asia - neurocysticercosis and CNS TB are important infective causes. Always ask about travel, diet (pork), and TB contacts.
SEIZURE CLASSIFICATION (ILAE 2017)
A. By Onset Type
SEIZURES
/ \
FOCAL GENERALISED UNKNOWN ONSET
(partial)
/ \
Aware Impaired → Can evolve to bilateral tonic-clonic
(Simple) Awareness ("focal to bilateral tonic-clonic")
(Complex)
1. Focal Onset Seizures
| Old Term | New ILAE 2017 Term |
|---|---|
| Simple partial | Focal aware seizure |
| Complex partial | Focal impaired awareness seizure |
| Secondary generalised | Focal to bilateral tonic-clonic |
- Motor features: clonic jerking, tonic posturing, automatisms (lip smacking, fumbling)
- Non-motor features: aura (epigastric rising, déjà vu, smell - temporal lobe), sensory, autonomic, emotional
- Todd's paresis: post-ictal focal weakness lasting minutes to hours after focal seizure - IMPORTANT for exams
2. Generalised Onset Seizures
| Type | Features |
|---|---|
| Tonic-clonic (grand mal) | Tonic phase (stiffening) → clonic phase (jerking); post-ictal confusion; tongue biting; urinary incontinence |
| Absence (petit mal) | Brief 5-20 sec staring; no post-ictal phase; 3 Hz spike-wave on EEG; childhood onset |
| Myoclonic | Brief muscle jerks; usually morning; juvenile myoclonic epilepsy (JME) |
| Atonic (drop attacks) | Sudden loss of muscle tone; falls; seen in Lennox-Gastaut syndrome |
| Tonic | Sustained muscle contraction; falls |
| Clonic | Rhythmic jerking without prior tonic phase |
⚠️ Exam High-Yield: Absence vs. focal impaired awareness - Absence: no aura, no post-ictal phase, very brief (<30 sec), 3 Hz spike-wave. Complex partial: may have aura, post-ictal confusion, longer, temporal EEG focus.
IMPORTANT EPILEPSY SYNDROMES
| Syndrome | Age | Features | EEG | Drug of Choice |
|---|---|---|---|---|
| West Syndrome (Infantile spasms) | 3-12 months | Salaam attacks; developmental regression | Hypsarrhythmia | ACTH / Vigabatrin |
| Lennox-Gastaut Syndrome | 1-7 years | Multiple seizure types (tonic, atonic, absence); intellectual disability | Slow spike-wave (<2.5 Hz) | Valproate, Clobazam; Rufinamide |
| Childhood Absence Epilepsy (CAE) | 4-10 years | Multiple daily absences; normal development | 3 Hz spike-wave | Ethosuximide / Valproate |
| Juvenile Myoclonic Epilepsy (JME) | 12-18 years | Morning myoclonic jerks + GTCS; precipitated by sleep deprivation | Polyspike-wave 4-6 Hz | Valproate (lifelong often needed) |
| Temporal Lobe Epilepsy (TLE) | Any | Focal impaired awareness + automatisms; aura common | Temporal spike-wave | Carbamazepine / Lamotrigine |
| Dravet Syndrome | <1 year | Febrile seizures → refractory epilepsy; SCN1A mutation | Varies | Valproate + Clobazam; avoid Na+ channel blockers |
| Benign Rolandic Epilepsy | 5-12 years | Nocturnal GTCS + facial twitching; self-limited | Centrotemporal spikes | Often no treatment needed |
DIAGNOSIS
History (Most Important)
- From witness (patient unaware during seizure): detailed account of ictal behaviour
- Onset: focal or generalised? Aura?
- Duration, frequency, precipitants (sleep deprivation, alcohol, flickering lights, fever, menstruation - catamenial epilepsy)
- Post-ictal phase: confusion, Todd's paresis, headache
- Birth history, developmental history, family history
- Drug/alcohol history
Investigations
- Most important investigation for epilepsy
- Epileptiform activity (spikes/sharp waves) in ~90% of epileptics depending on recording circumstances
- Only ~2% of non-epileptics show epileptiform activity
- Interictal EEG is usual (not during seizure)
- Normal EEG does NOT exclude epilepsy
- Ictal EEG (video-EEG monitoring) = gold standard
- Sleep-deprived EEG, hyperventilation, photic stimulation increase yield
- Photosensitive epilepsy: photoparoxysmal response on photic stimulation
⚠️ Exam Trap: "The EEG is always abnormal in epilepsy" - FALSE. A substantial number of epileptics have consistently normal interictal EEGs.
- MRI brain - preferred; detects structural causes (hippocampal sclerosis, tumours, cortical dysplasia, vascular malformations)
- CT brain - for acute settings (haemorrhage, calcification e.g. neurocysticercosis)
- Hippocampal sclerosis (mesial temporal sclerosis): most common structural cause of TLE; MRI shows hippocampal atrophy and T2 hyperintensity
- FBC, electrolytes (Na, Ca, Mg, glucose), renal/liver function
- AED levels (if on treatment)
- Prolactin: rises after tonic-clonic seizures (within 20 min) - helps differentiate from pseudoseizures (non-epileptic attack disorder / NEAD)
- If meningitis/encephalitis suspected
- Not routine
DIFFERENTIAL DIAGNOSIS
⚠️ Very commonly tested - Differentiating seizure from syncope/pseudoseizure
| Feature | Epileptic Seizure | Syncope | Non-Epileptic Attack (NEAD/Pseudoseizure) |
|---|---|---|---|
| Prodrome | Aura (specific) | Pre-syncope: dizziness, dimming vision | Variable, emotional trigger often |
| Position | Any | Upright | Any |
| Colour | Cyanosis (GTCS) | Pallor | Normal or flushing |
| Duration | Usually <3 min | Seconds | Often prolonged (>2 min), waxing-waning |
| Jerking | Synchronous, rhythmic | Brief myoclonic (if prolonged) | Asynchronous, thrashing, pelvic thrusting |
| Tongue bite | Side of tongue | Tip of tongue (rare) | Rare |
| Incontinence | Common (GTCS) | Uncommon | Uncommon |
| Post-ictal confusion | Yes (mins-hours) | Rapid recovery | Variable, often prolonged |
| Prolactin | Elevated (20 min post-GTCS) | Normal | Normal |
| EEG during attack | Abnormal | Normal | Normal |
MANAGEMENT OF EPILEPSY
When to Start AEDs?
- After 2 or more unprovoked seizures
- After 1 seizure if: known structural lesion, abnormal EEG, abnormal neurology, strong family history, or high personal risk (e.g., driver)
General Principles
- Monotherapy first - start low, go slow; 70% controlled with first AED
- If first drug fails at adequate dose → try second monotherapy
- Combination only after 2 monotherapies fail
- Drug-refractory epilepsy = failure of 2 appropriate AEDs at adequate doses
AED Selection by Seizure Type
| Seizure/Syndrome | First-line | Second-line/Alternatives |
|---|---|---|
| Focal seizures | Carbamazepine, Lamotrigine, Oxcarbazepine | Levetiracetam, Sodium valproate, Gabapentin |
| Generalised tonic-clonic | Sodium valproate, Lamotrigine | Levetiracetam, Carbamazepine (with caution) |
| Absence | Ethosuximide, Sodium valproate | Lamotrigine |
| Myoclonic | Sodium valproate | Levetiracetam, Clonazepam |
| JME | Sodium valproate | Levetiracetam, Lamotrigine |
| TLE (focal) | Carbamazepine | Lamotrigine, Levetiracetam |
⚠️ Critical Exam Point: Carbamazepine WORSENS absence, myoclonic and atonic seizures - NEVER use in generalised epilepsy syndromes with these types.
⚠️ Valproate in women of childbearing age: HIGH teratogenicity risk (neural tube defects, cognitive effects in child) - AVOID if possible; requires Pregnancy Prevention Programme in UK (relevant for Harrison's/Kumar & Clark).
Key AED Side Effects (High Yield)
| Drug | Important Side Effects |
|---|---|
| Carbamazepine | Diplopia, ataxia, hyponatraemia (SIADH), rash (Stevens-Johnson in HLA-B*1502 - Asian patients), aplastic anaemia, enzyme inducer |
| Phenytoin | Nystagmus, ataxia, gingival hyperplasia, hirsutism, coarse facies, folate deficiency, peripheral neuropathy, zero-order kinetics (small dose change = large level change) |
| Sodium Valproate | Tremor, weight gain, hair loss (reversible), teratogenicity (neural tube defects), hepatotoxicity (especially in children <2 y), thrombocytopenia, pancreatitis |
| Lamotrigine | Rash (SJS if titrated too fast), insomnia, diplopia; must titrate SLOWLY especially with valproate |
| Levetiracetam | Behavioural problems, irritability, depression; otherwise well tolerated |
| Ethosuximide | GI upset, headache; only for absence seizures |
| Phenobarbitone | Sedation, tolerance, hyperactivity in children, enzyme inducer, dependence |
| Carbamazepine/Phenytoin/Phenobarb | Enzyme inducers - affect OCP, warfarin, other drugs |
⚠️ HLA-B*1502 (common in Sri Lankan/South Asian populations) - associated with carbamazepine-induced Stevens-Johnson Syndrome. Consider testing before starting carbamazepine.
Stopping AEDs
- Consider after 2 years seizure-free
- Must discuss driving licence implications
- Gradual taper over months (never abrupt - risk of withdrawal seizures)
- Higher risk of recurrence: structural cause, abnormal EEG, focal epilepsy
Drug-Refractory Epilepsy (20%)
- Surgery: anterior temporal lobectomy - 80-90% seizure freedom in mesial TLE with hippocampal sclerosis
- Vagus Nerve Stimulation (VNS): ~50% get ≥50% seizure reduction
- Deep Brain Stimulation (DBS): anterior nucleus of thalamus
- Responsive Neurostimulation (RNS): closed-loop device
- Ketogenic diet: especially in children; high fat, low carbohydrate
STATUS EPILEPTICUS (SE)
Definition
- Convulsive SE: seizure lasting >5 minutes (operational - time to treat; older definition was 30 min)
- Traditional definition: >30 minutes of continuous seizure OR ≥2 seizures without full recovery between them
- A medical emergency - mortality 10-20%
Causes (VITAMINS mnemonic)
Most common cause in a known epileptic = AED non-compliance
Management - Time-Based Protocol
| Time | Action |
|---|---|
| 0-5 min | ABC, O₂, position (left lateral), IV access, blood glucose (BM), bloods (FBC, U&E, Ca, Mg, glucose, LFT, AED levels, ABG), ECG, monitor |
| 5-10 min (1st line) | Lorazepam IV 0.1 mg/kg (4 mg in adult) - drug of choice; or Diazepam IV 0.15-0.25 mg/kg; Midazolam buccal/IM if no IV access |
| If seizure continues 5 min after 1st benzodiazepine | Repeat benzodiazepine (second dose) |
| 10-30 min (2nd line) | Levetiracetam IV (preferred now) OR Fosphenytoin IV OR Sodium valproate IV; start while giving 2nd benzo |
| 30-60 min (Refractory SE) | Anaesthetic agents: Propofol OR Thiopental OR Midazolam infusion; intubation; ICU; continuous EEG monitoring |
| >60 min (Super-refractory SE) | Ketamine, hypothermia, ketogenic diet, immunotherapy (if autoimmune encephalitis), surgery |
⚠️ Exam Point: Lorazepam (not diazepam) is drug of choice for IV SE because it has longer CNS duration of action. Diazepam preferred if IV access unavailable (rectal). Midazolam IM/buccal for pre-hospital.
⚠️ Fosphenytoin preferred over phenytoin IV (less cardiotoxic, can give faster, no propylene glycol).
⚠️ If glucose low or alcoholic → give thiamine BEFORE dextrose (prevents Wernicke's).
EPILEPSY IN SPECIAL SITUATIONS
Epilepsy & Driving
- Must be seizure-free for 1 year before driving a private car (UK/most countries; Sri Lanka guidelines similar)
- Heavy goods/bus: seizure-free for 10 years off medication
- Must notify the licensing authority
Epilepsy & Pregnancy
- Uncontrolled seizures are MORE dangerous to foetus than most AEDs
- Valproate: highest teratogenic risk - avoid (neural tube defects, spina bifida, developmental delay)
- Carbamazepine: lowest teratogenic risk among older AEDs; still causes neural tube defects
- Lamotrigine/Levetiracetam: preferred in pregnancy
- Give folic acid 5 mg/day pre-conception and throughout pregnancy
- Vitamin K to neonate at birth (enzyme-inducing AEDs reduce clotting factor synthesis)
Febrile Convulsions (relevant to Paeds rotation)
- Age 6 months - 6 years; fever >38°C
- Simple: <15 min, generalised, single episode in 24h, complete recovery
- Complex: >15 min OR focal OR >1 episode in 24h → investigate further
- NOT the same as epilepsy; only 2-3% develop epilepsy later
- Treatment: diazepam rectal/buccal midazolam for seizure; antipyretics; NOT regular AEDs for simple febrile convulsions
EXAM SUMMARY - HIGH-YIELD POINTS
| # | Key Point |
|---|---|
| 1 | Epilepsy = ≥2 unprovoked seizures; a provoked seizure is NOT epilepsy |
| 2 | ILAE 2017: focal aware / focal impaired awareness / focal to bilateral tonic-clonic |
| 3 | EEG: ~90% show epileptiform activity; normal EEG does NOT exclude epilepsy |
| 4 | Absence: 3 Hz spike-wave; no post-ictal phase; ethosuximide or valproate |
| 5 | Carbamazepine worsens absence/myoclonic/atonic seizures - never use |
| 6 | Valproate: most teratogenic - avoid in women of childbearing age |
| 7 | HLA-B*1502 (Asian): carbamazepine → Stevens-Johnson Syndrome |
| 8 | Phenytoin: zero-order kinetics, gingival hyperplasia, hirsutism, nystagmus |
| 9 | SE first-line = IV Lorazepam; second-line = Levetiracetam/Fosphenytoin/Valproate IV |
| 10 | Status epilepticus operational definition = >5 min (treat now, don't wait for 30 min) |
| 11 | Todd's paresis = post-ictal focal weakness; distinguishes focal from generalised |
| 12 | Prolactin elevated after GTCS (within 20 min); normal in pseudoseizures |
| 13 | Febrile convulsions: do NOT give regular AEDs for simple febrile convulsions |
| 14 | Drug-refractory TLE → temporal lobectomy; 80-90% seizure freedom |
| 15 | Drive only after 1 year seizure-free (private car) |