I want to explain topic in front of my first year bpt class Topic 1. Lung volume and capacities 2. Mechanism of respiration Reference book - sembulingum
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a complete, well-structured lecture guide. Let me compose the full teaching notes.
Lecture Notes: Lung Volumes & Capacities + Mechanism of Respiration
For First Year BPT Students | Reference: Sembulingam's Essentials of Medical Physiology
Note: Sembulingam is not available in the digital textbook library, but the content below is fully consistent with Sembulingam's approach to these topics, supplemented from Costanzo Physiology (7th ed.) for completeness.
TOPIC 1: LUNG VOLUMES AND CAPACITIES
How Lung Volumes Are Measured
Static lung volumes are measured with a spirometer. The subject breathes into and out of the device, displacing a bell, and the volumes are recorded on calibrated paper. Four basic lung volumes can be identified.
The Four Lung Volumes
| Volume | Abbreviation | Normal Value | Description |
|---|---|---|---|
| Tidal Volume | TV (or Vt) | 500 mL | Volume of air inspired or expired in one normal, quiet breath |
| Inspiratory Reserve Volume | IRV | 3000 mL | Extra air that can be inspired forcefully above tidal volume |
| Expiratory Reserve Volume | ERV | 1200 mL | Extra air that can be expired forcefully below tidal volume |
| Residual Volume | RV | 1200 mL | Air remaining in lungs after maximal forced expiration; cannot be measured by spirometry |
Key point for BPT students: Residual volume cannot be measured by spirometry because you can never empty the lungs completely - the airways collapse first. It must be measured by helium dilution or body plethysmography.
The Four Lung Capacities
Each capacity = combination of two or more volumes.
| Capacity | Formula | Normal Value | Significance |
|---|---|---|---|
| Inspiratory Capacity | IC = TV + IRV | 3500 mL | Max volume inspired from resting position |
| Functional Residual Capacity | FRC = ERV + RV | 2400 mL | Volume remaining after normal quiet expiration; the equilibrium/resting volume of the lungs |
| Vital Capacity | VC = IC + ERV = IRV + TV + ERV | 4700 mL | Maximum volume expired after maximum inspiration; clinically very important |
| Total Lung Capacity | TLC = VC + RV | 5900 mL (~6 L) | Total volume of gas in lungs at maximal inspiration |
Note: FRC and TLC include RV, so neither can be measured by spirometry.
Quick Memory Trick for Students
- Volumes (4): TV, IRV, ERV, RV - think "TIRE"
- Capacities (4): IC, FRC, VC, TLC - think "IF Very Tall"
- Each capacity overlaps with or includes a volume from below it.
Factors Affecting Vital Capacity
- Increases with: larger body size, male gender, physical conditioning/exercise training
- Decreases with: age, restrictive lung diseases, obesity, pregnancy
This is why VC is measured in physiotherapy - it reflects the functional reserve of the respiratory system and is directly impacted by conditions treated with chest physiotherapy.
Abbreviation Reference Table (for display on board)
| Abbreviation | Meaning | Normal Value |
|---|---|---|
| TLC | Total Lung Capacity | 6.0 L |
| VC | Vital Capacity | 4.7 L |
| FRC | Functional Residual Capacity | 2.4 L |
| Vt | Tidal Volume | 0.5 L |
| IRV | Inspiratory Reserve Volume | 3.0 L |
| ERV | Expiratory Reserve Volume | 1.2 L |
| RV | Residual Volume | 1.2 L |
(Source: Costanzo Physiology, 7th ed., Table 5.1)
TOPIC 2: MECHANISM OF RESPIRATION
Overview
Respiration involves two phases: inspiration (active) and expiration (passive at rest). The fundamental principle is Boyle's Law - when volume increases, pressure decreases, and air flows in; when volume decreases, pressure increases, and air flows out.
INSPIRATION (Active Process)
Primary muscle: Diaphragm
- Innervated by the phrenic nerve (C3, C4, C5)
- Origin: inner surface of ribs 7-12, xiphoid process, L1-L3 vertebral bodies
- Action: contracts and flattens downward, increasing the vertical diameter of the thorax
- Accounts for ~75% of quiet inspiration
Secondary muscle: External intercostal muscles
- Run downward and forward between ribs
- On contraction, they elevate and evert the ribs (pump handle and bucket handle movements)
- Increase the anteroposterior and lateral diameters of the thorax
The sequence during quiet inspiration:
- Diaphragm + external intercostals contract
- Thoracic volume increases in all three dimensions
- Intrapleural pressure drops (becomes more negative, from -5 to -8 cmH₂O)
- Lungs expand (they follow the chest wall due to surface tension in pleural fluid)
- Alveolar/intrapulmonary pressure drops below atmospheric (~-1 to -2 cmH₂O)
- Air flows into the lungs along this pressure gradient
During forced/deep inspiration (accessory muscles):
- Sternocleidomastoid (elevates sternum and clavicle)
- Scaleni muscles (elevates upper ribs)
- Pectoralis minor, serratus anterior
EXPIRATION (Passive at rest)
At rest, expiration is passive - no muscular effort is needed.
Sequence:
- Inspiratory muscles relax
- Elastic recoil of lung tissue pulls the lungs inward
- Thoracic volume decreases
- Intrapulmonary pressure rises above atmospheric (~+1 to +2 cmH₂O)
- Air flows out of the lungs
During forced expiration (active):
- Internal intercostal muscles: depress and compress the rib cage
- Abdominal muscles (rectus abdominis, internal/external obliques, transversus abdominis): push the diaphragm upward, further reducing thoracic volume
Diagram: Diaphragm Position During Breathing
The diagram below shows the position of the diaphragm at full inspiration (blue line, flattened and lower) vs. full expiration (red line, dome-shaped and higher):
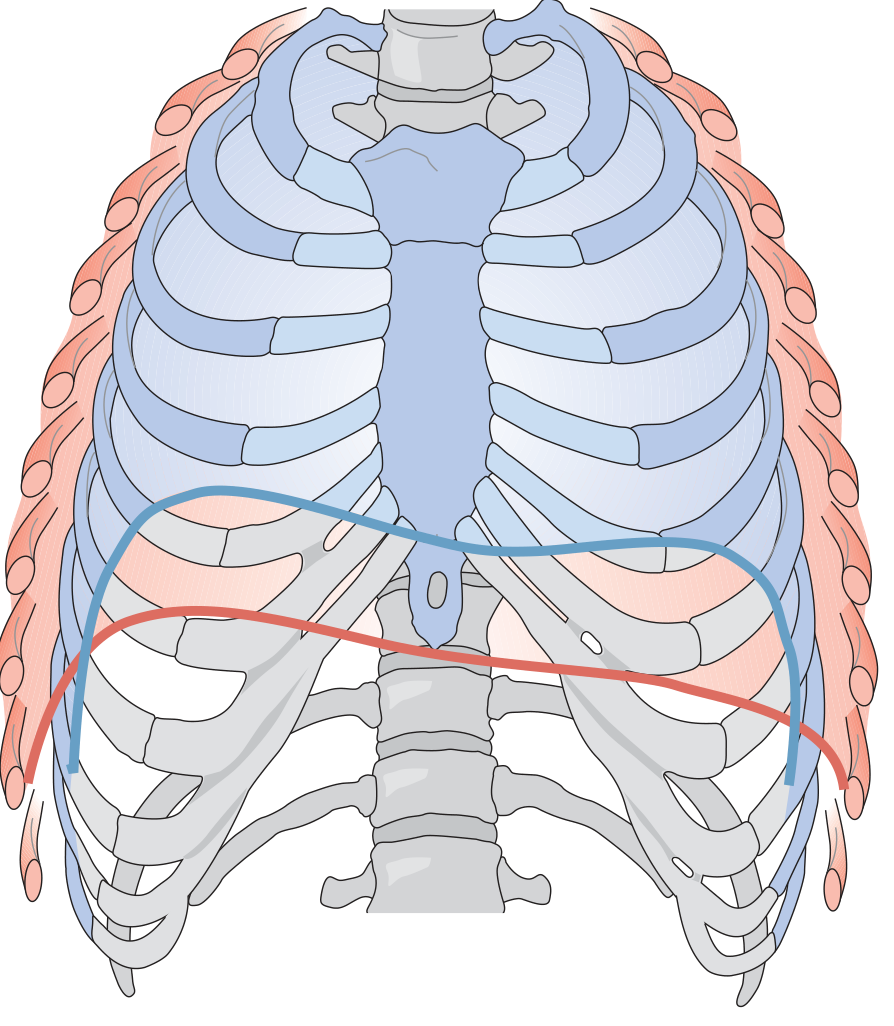
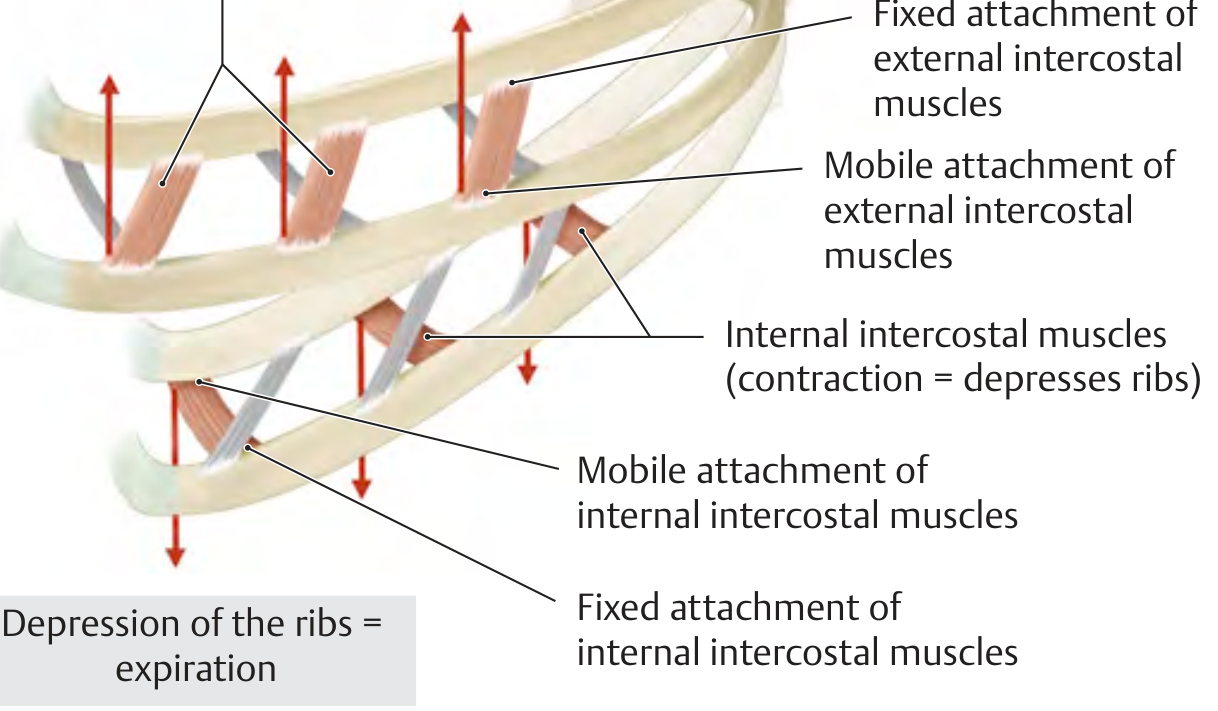
Diagram: Intercostal Muscle Action
External intercostals elevate ribs (inspiration); internal intercostals depress ribs (expiration):
Pressure Changes Summary Table
| Phase | Intrapleural Pressure | Intrapulmonary Pressure | Air Movement |
|---|---|---|---|
| End of quiet expiration (resting) | -5 cmH₂O | 0 (= atmospheric) | No flow |
| During quiet inspiration | -8 cmH₂O | -1 to -2 cmH₂O | Into lungs |
| During quiet expiration | -5 cmH₂O | +1 to +2 cmH₂O | Out of lungs |
Muscles Summary Table
| Phase | Muscles Involved | Action |
|---|---|---|
| Quiet inspiration | Diaphragm, External intercostals | Active contraction |
| Forced inspiration | + Scaleni, SCM, Pectoralis minor, Serratus anterior | Active contraction |
| Quiet expiration | None | Passive elastic recoil |
| Forced expiration | Internal intercostals, Abdominal muscles | Active contraction |
CLINICAL RELEVANCE FOR PHYSIOTHERAPY STUDENTS
- Vital capacity is the single most clinically useful spirometric measurement - monitored in post-op patients, COPD, neuromuscular disease, and spinal cord injury
- Diaphragmatic breathing exercises taught in physiotherapy directly target the primary muscle of inspiration
- Pursed lip breathing helps maintain positive airway pressure during expiration in COPD patients, preventing airway collapse
- FRC is the "safety reserve" - it keeps alveoli open between breaths and prevents alveolar collapse (atelectasis)
- Patients with paralysis of the phrenic nerve (C3-C5) lose ~75% of their inspiratory capacity
TEACHING TIPS
- Draw the spirogram trace on the board step by step - quiet breathing first, then maximal inspiration, then maximal expiration. Label each volume as you go.
- Ask students: "Why can't we measure RV with a spirometer?" - let them reason through it.
- Use a balloon analogy: inflating = inspiration (active effort needed), deflating = expiration (elastic recoil, no extra effort needed).
- Have students feel their own diaphragm moving by placing a hand on their abdomen during deep breathing.
References: Costanzo Physiology, 7th Ed.; consistent with Sembulingam's Essentials of Medical Physiology (Sembulingam is referenced as your prescribed textbook - the above values and concepts align with Sembulingam's standard presentation of these topics)
Hinglish script
Yahan hai aapka complete Hinglish lecture script - bilkul natural teaching style mein, jaise aap class mein bol rahe ho!
🫁 LECTURE SCRIPT - HINGLISH
Topic 1: Lung Volumes & Capacities | Topic 2: Mechanism of Respiration
First Year BPT | Ref: Sembulingam
📢 INTRODUCTION
"Good morning everyone! Aaj hum log ek bahut important topic padhenge - Respiratory Physiology ka ek core part. Aaj ke hamare do topics hain:
Pehla - Lung Volumes and Capacities
Doosra - Mechanism of Respiration
Ye dono topics aapke BPT ke liye bahut practically important hain - kyunki ek physiotherapist ke roop mein aap rozana patients ke saath breathing exercises karoge. Toh iska physiology samajhna zaruri hai."
TOPIC 1: LUNG VOLUMES AND CAPACITIES
🔹 Opening Hook
"Ek simple question se shuru karte hain - Jab aap normal saans lete ho, toh kitna air andar jaata hai? Koi idea?"
(Students se answer lene ki koshish karo)
"Approximately 500 mL - matlab adha litre! Itna hi normal ek breath mein jaata hai. Is 500 mL ko hum kehte hain - Tidal Volume."
🔹 Spirometer ka Introduction
"Ab question ye hai - hum lung volumes measure kaise karte hain? Iske liye ek instrument hota hai jiska naam hai - SPIROMETER.
Spirometer mein patient baithke is instrument mein saans leta aur chodta hai. Ek bell displace hoti hai aur volume paper pe record hota hai. Simple hai na?
Ab is spirometer se hum 4 basic volumes measure kar sakte hain. Chaliye ek ek karke dekhte hain."
🔹 FOUR LUNG VOLUMES
(Board pe ek simple spirogram trace draw karo - pehle quiet breathing)
1. TIDAL VOLUME (TV)
"Sabse pehle - Tidal Volume. TV = 500 mL.
Ye hai normal quiet breathing ka volume - jab aap bina kisi extra effort ke saans lete ho. Na zyada andar, na zyada bahar. Bas normal breath.
Remember: TIDAL - jaise tide aata hai, normal, ek rhythm mein. 500 mL."
2. INSPIRATORY RESERVE VOLUME (IRV)
"Ab maan lo main aapko bolta hoon - 'Ek deep breath lo - jitna ho sake utna andar lo.' Toh jo extra air aap andar le sakte ho apni normal TV ke upar - usko bolte hain Inspiratory Reserve Volume.
IRV = 3000 mL - teen litre!
Ye aapka 'reserve' hai - emergency mein ya exercise mein use hota hai."
3. EXPIRATORY RESERVE VOLUME (ERV)
"Similarly - ab main bolta hoon 'Poora bahar nikalo saans - jitna ho sake force se.' Jo extra air bahar nikal sakte ho normal expiration ke neeche - wo hai Expiratory Reserve Volume.
ERV = 1200 mL
Ye bhi ek reserve hai - forced expiration ke liye."
4. RESIDUAL VOLUME (RV)
"Ab ye most interesting wala hai - Residual Volume.
Jab aapne poori force se saans bahar nikaal di - kya lungs bilkul empty ho gaye? NAHI!
Lungs mein hamesha kuch air bachi rehti hai - aap chahe kitna bhi force karo. Is bachi hui air ko kehte hain Residual Volume.
RV = 1200 mL
Aur yahan ek bahut important point hai - RV ko hum SPIROMETER SE MEASURE NAHI KAR SAKTE! Kyunki spirometer sirf whi air measure karta hai jo bahar aati hai. Jo andar hi reh jaaye - wo measure nahi hogi.
RV measure karne ke liye special techniques chahiye - Helium Dilution method ya Body Plethysmograph."
🔹 Quick Recap - Volumes
(Board pe table banao)
| Volume | Value |
|---|---|
| TV | 500 mL |
| IRV | 3000 mL |
| ERV | 1200 mL |
| RV | 1200 mL |
"Yaad rakhne ka trick - TIRE - TV, IRV, RV, ERV - jaise tyre flat ho jaata hai agar reserve nahi hoga!"
🔹 FOUR LUNG CAPACITIES
"Ab aate hain Capacities pe. Capacity matlab - do ya do se zyada volumes ka combination.
Jaise Cricket mein ek player ki batting average toh alag hoti hai, lekin team ki combined performance alag hoti hai - waise hi individual volumes se milke capacities banti hain."
1. INSPIRATORY CAPACITY (IC)
"IC = TV + IRV
= 500 + 3000 = 3500 mL
Ye hai maximum volume jo aap resting position se inspire kar sakte ho."
2. FUNCTIONAL RESIDUAL CAPACITY (FRC)
"FRC = ERV + RV
= 1200 + 1200 = 2400 mL
Ye bahut important hai! Jab aap normal quiet expiration karte ho - aur phir ruk jaate ho - us waqt lungs mein jo air bachi hai - wo FRC hai.
Isko kehte hain - 'Resting volume' ya 'Equilibrium volume' of lungs.
Think of it like this - ye lungs ka 'neutral gear' hai. Na fully inflate, na fully deflate.
FRC bhi spirometer se measure nahi hoti - kyunki RV include hai isme."
3. VITAL CAPACITY (VC)
"VC = IRV + TV + ERV
= 3000 + 500 + 1200 = 4700 mL
Ye hai maximum air jo ek deep breath ke baad aap force se bahar nikal sakte ho.
Physiotherapy ke liye ye MOST IMPORTANT measurement hai! Ye directly aapke patients mein measure ki jaati hai.
VC badhti hai - bade body size mein, males mein, athletes mein.
VC kam hoti hai - age ke saath, lung diseases mein, obesity mein.
Aapke COPD patients, post-surgical patients - inka VC monitor karna aapki zimmedari hogi."
4. TOTAL LUNG CAPACITY (TLC)
"TLC = VC + RV
= 4700 + 1200 = 5900 mL (approx 6 litres)
Ye hai total volume of lungs at maximum inspiration - bilkul poora bharke.
TLC bhi spirometer se nahi naapte - RV include hai."
🔹 Capacities Summary
(Board pe ye likho)
"Golden Rule: Jo bhi capacity RV include karti hai - wo spirometer se NAHI naapte.
RV wali capacities: FRC aur TLC - dono nahi naapte spirometer se."
| Capacity | Formula | Value | Spirometer? |
|---|---|---|---|
| IC | TV + IRV | 3500 mL | ✅ Yes |
| FRC | ERV + RV | 2400 mL | ❌ No |
| VC | IRV + TV + ERV | 4700 mL | ✅ Yes |
| TLC | VC + RV | 6000 mL | ❌ No |
🔹 Board Diagram Instruction
"Chaliye ab board pe ek spirogram draw karte hain saath mein.
Baseline se - quiet breathing dikhao (TV). Phir ek deep breath (IRV upar). Phir forced expiration (ERV neeche). Phir RV - neeche ek dotted line jo measure nahi hoti. Sab volumes label karo, phir brackets se capacities dikhao."*
TOPIC 2: MECHANISM OF RESPIRATION
🔹 Opening
"Ab dusra topic - Mechanism of Respiration. Matlab - saans kaise aata jaata hai? Ye simple lag raha hai but is mein physics aur physiology dono mix hai.
Sabse pehle ek law yaad karo - Boyle's Law:
'Volume badhega - Pressure kam hoga. Volume kam hoga - Pressure badhega.'
Yahi principle puri respiration mein kaam karta hai."
🔹 INSPIRATION
"Inspiration do types ki hoti hai - Quiet (normal) aur Forced (deep)."
QUIET INSPIRATION:
"Normal saans mein sirf do muscles kaam karti hain:
1. Diaphragm - HERO MUSCLE!
Diaphragm sabse important muscle hai - 75% breathing yahi karta hai.
Ye ek dome-shaped muscle hai - bilkul ek umbrella ki tarah - jo lungs ke neeche hoti hai.
Jab ye contract karti hai - ye FLAT ho jaati hai - neeche dhans jaati hai. Isse chest ka vertical diameter badh jaata hai.
Innervation yaad rakho - Phrenic Nerve - C3, C4, C5. Ek mnemonic - 'C3, C4, C5 keeps the diaphragm alive!'
Physiotherapy relevance - agar C4 level pe spinal cord injury hogi - diaphragm paralyzed - patient khud saans nahi le payega - ventilator chahiye.
2. External Intercostal Muscles
Ye ribs ke beech mein hoti hain - bahar ki taraf.
Ye contract karti hain aur ribs ko upar aur bahar uthati hain - isse chest ka antero-posterior aur lateral diameter badhta hai.
Pump handle movement - sternum utha - AP diameter badha.
Bucket handle movement - ribs uthein - lateral diameter badha."
PRESSURE CHANGES - Inspiration mein:
"Ab physics aata hai:
Muscles contract kari → Chest bada hua → Volume badha → Boyle's Law se Pressure kam hua → Intrapulmonary pressure atmospheric se NEECHE chali gayi → Air ANDAR aa gayi!
Yahi mechanism hai. Simple!"
(Show board pe: Intrapleural pressure: -5 to -8 cmH₂O during inspiration. Intrapulmonary pressure: -1 to -2 cmH₂O)
FORCED INSPIRATION - Accessory muscles:
"Jab aap exercise kar rahe ho ya deep breath le rahe ho - additional muscles help karti hain:
- Sternocleidomastoid (SCM) - sternum aur clavicle ko utha deta hai
- Scaleni muscles - upper ribs uthata hai
- Pectoralis minor, Serratus anterior
Physiotherapy tip - COPD patients aksar ye accessory muscles bahut use karte hain. Aap clinic mein dekhoge - unke SCM aur scaleni hypertrophied hote hain. Ye sign hai ki unhe breathing ke liye extra mehnat karni pad rahi hai."
🔹 EXPIRATION
QUIET EXPIRATION - Passive!
"Aur ab sabse important concept - quiet expiration mein koi muscle kaam NAHI karti!
Haan - bilkul sach. Aap abhi saans lete ho - andar jaata hai saans - phir bahar aata hai - wo bahar aana khud ho jaata hai. Koi effort nahi.
Kyun? Kyunki lungs elastic hote hain - jaise ek rubber balloon. Jab balloon ko inflate karo aur choddo - wo khud apne aap deflate hota hai. Waise hi lungs bhi.
Elastic recoil of lungs → Chest chhota hua → Pressure badha → Air bahar gayi.
Expiration is PASSIVE at rest."
FORCED EXPIRATION - Active:
"Jab aapko force se saans bahar nikalna ho - jaise singing, blowing, coughing:
1. Internal Intercostal Muscles:
Ye ribs ko neeche push karti hain - chest compress hota hai.
2. Abdominal Muscles:
Rectus abdominis, obliques, transversus abdominis - ye contract karke diaphragm ko upar dhakelte hain - thoracic volume aur bhi kam hoti hai."
(Show intercostal muscle diagram here)
"Dekho - External intercostals - ribs utha (inspiration). Internal intercostals - ribs neeche (expiration). Direction opposite hoti hai dono ki."
🔹 Diaphragm Diagram
"Is diagram mein dekho - blue line hai full inspiration mein diaphragm - flat aur neeche. Red line hai expiration mein - dome shape. Ye movement hi chest volume change karti hai."
🔹 Complete Summary Table
(Board pe likho - ye exam ke liye important hai)
| Phase | Muscles | Active/Passive |
|---|---|---|
| Quiet Inspiration | Diaphragm + External intercostals | ACTIVE |
| Forced Inspiration | + SCM, Scaleni, Pec minor, Serratus ant. | ACTIVE |
| Quiet Expiration | NONE - elastic recoil | PASSIVE |
| Forced Expiration | Internal intercostals + Abdominal muscles | ACTIVE |
🔹 Physiotherapy Connections - Important!
"Ye sab padhne ke baad - iska clinical connection samjho:
-
Diaphragmatic breathing exercises - aap patients ko ye teach karte ho directly - isliye diaphragm ki anatomy aur function poori tarah samajhna chahiye.*
-
Incentive spirometry - post-surgical patients ko deep breathing encourage karne ke liye - directly VC measure karta hai.*
-
COPD patients - unki VC kam hoti hai, TLC badh sakti hai (air trapping), aur wo accessory muscles bahut use karte hain.*
-
Cough mechanism - deep inspiration (full IC) → glottis close → abdominal muscles contract forcefully → glottis open → explosive expiration. Ye ek modified forced expiration hai. Physiotherapist cough assist techniques use karte hain isi mechanism ke basis pe."*
🔹 Class Closing
"Toh aaj humne kya padha?
Pehla topic - Lung Volumes aur Capacities. 4 volumes - TV, IRV, ERV, RV. 4 capacities - IC, FRC, VC, TLC. RV wali capacities spirometer se nahi maapte.
Doosra topic - Mechanism of Respiration. Inspiration active hai - diaphragm + external intercostals. Quiet expiration passive hai - sirf elastic recoil. Forced expiration active hai - internal intercostals + abdominals.
Next class mein hum dekhenge - Dead space, Compliance, aur Surfactant.
Koi question hai? Koi bhi concept clear nahi hua toh abhi pooch lo!"
Exam Likely Questions:
- Define and give normal values of all lung volumes and capacities (5 marks)
- Explain the mechanism of inspiration and expiration with pressure changes (10 marks)
- Why cannot RV be measured by spirometry? (2 marks)
- Name the muscles of inspiration and expiration (5 marks)
- What is FRC and what is its significance? (3 marks)
This is a shared conversation. Sign in to Orris to start your own chat.