Route and spread of maxillary carcinoma 10 marks answer for ms ent exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a thorough 10-mark MS ENT exam answer. Here it is:
Route and Spread of Maxillary Carcinoma
Introduction
Carcinoma of the maxillary sinus (antrum) is the most common sinonasal malignancy, accounting for approximately 55% of all sinonasal tumours. Squamous cell carcinoma is the predominant histological type. A defining feature of this tumour is late presentation - only 25% of maxillary sinus carcinomas are confined within the antrum at the time of diagnosis, making understanding of spread patterns clinically essential.
Ohngren's Line - Prognostic Division of Spread
Described in 1933, Ohngren's line runs from the medial canthus of the eye to the angle of the mandible. It divides the maxillary sinus into:
- Suprastructure (above the line): Tumours here spread towards the orbit, skull base, pterygoid plates and infratemporal fossa - worse prognosis, less resectable
- Infrastructure (below the line): Tumours spread towards the oral cavity, alveolus and palate - better prognosis, more amenable to surgery
1. Local / Direct Spread
Sinonasal carcinomas first fill the antrum before eroding bony walls. Periosteum and dura act as temporary barriers, but thin bone (anterior maxilla, orbital floor) is readily destroyed.
| Direction | Structures Involved | Clinical Features |
|---|---|---|
| Medially | Lateral nasal wall, nasal cavity | Nasal obstruction, epistaxis, unilateral discharge |
| Laterally | Cheek, buccal sulcus | Cheek swelling, skin ulceration (see image below) |
| Superiorly | Orbital floor, inferior orbital fissure, orbit | Proptosis, diplopia, epiphora, infraorbital paraesthesia |
| Inferiorly | Hard palate, alveolus | Loose teeth, palatal swelling, oro-antral fistula |
| Posteriorly | Infratemporal fossa, pterygopalatine fossa, pterygoid plates | Trismus (key sign), referred otalgia |
| Posterosuperiorly | Skull base, cavernous sinus, middle cranial fossa | Cranial nerve palsies, intracranial extension |

Advanced carcinoma of the maxillary antrum. The tumour has breached the lateral wall and presents as a swelling in the cheek. (Scott-Brown's Otorhinolaryngology)
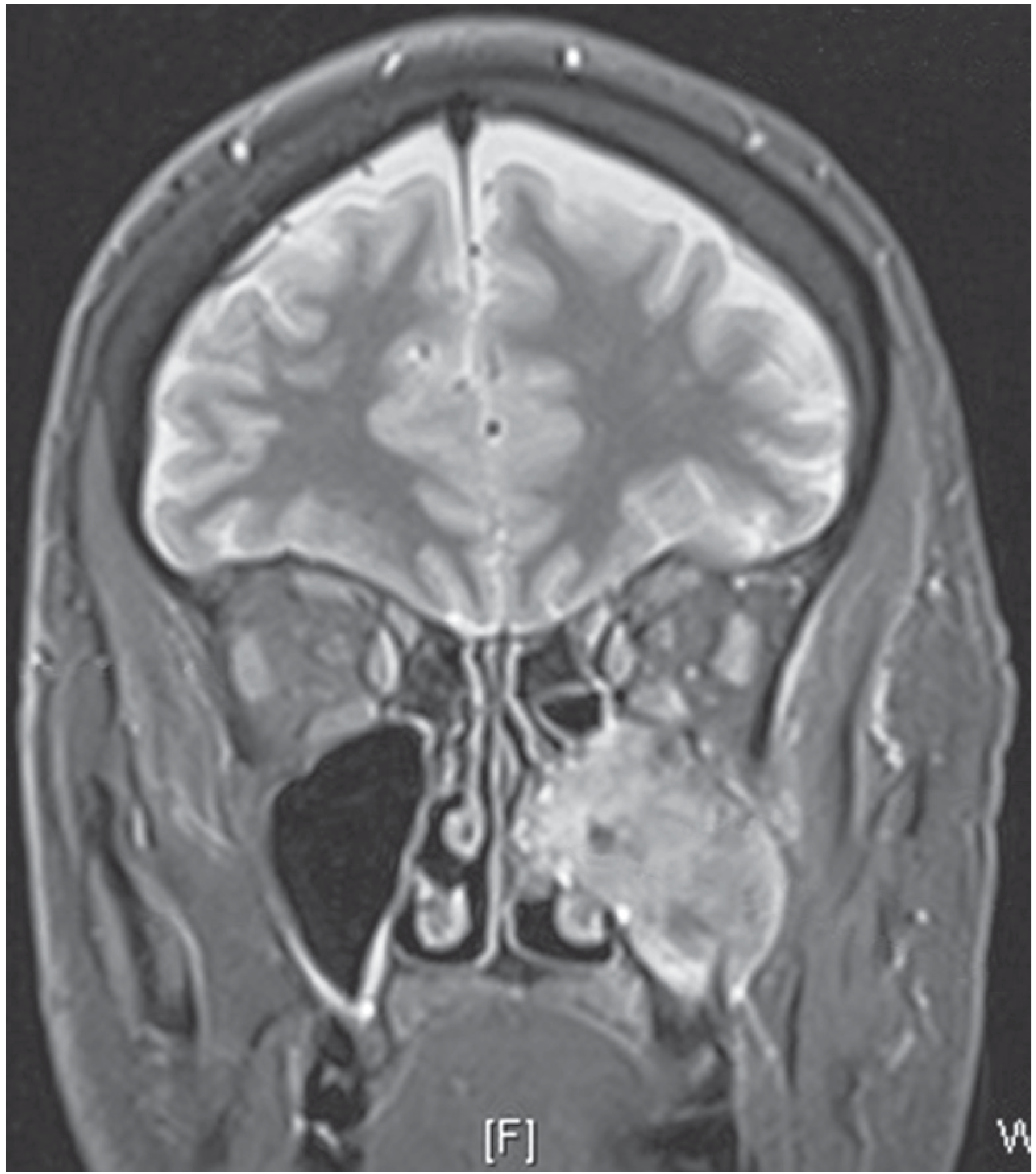
Coronal MRI: Extensive left maxillary antral carcinoma invading adjacent structures including the orbit. (Bailey & Love's)
2. Perineural Spread
This is a clinically important route, particularly in adenoid cystic carcinoma but also in SCC:
- Greater palatine nerve - from palatal tumours, spread travels superiorly through the greater palatine foramen into the pterygopalatine fossa
- Infraorbital nerve (V2 branch of trigeminal) - infraorbital paraesthesia / numbness of the cheek is an early warning sign of nerve involvement
- Maxillary division of trigeminal (V2) - can carry tumour intracranially through the foramen rotundum to the Meckel's cave and cavernous sinus
3. Regional Lymphatic Spread
The lymphatic drainage of the maxillary sinus is relatively sparse. Two pathways exist:
Anterior pathway: Anteroinferior nasal cavity and nasal vestibule drain to facial, parotid, and submandibular nodes, then to the upper deep cervical chain.
Posterior pathway: The remainder of the nose and paranasal sinuses drain anteriorly to the Eustachian tube to retropharyngeal nodes (first echelon), then to the upper deep cervical chain.
Key points for the exam:
- Lymph node spread occurs in 25-35% of patients at some point during disease
- Only ~10% present with nodal disease at diagnosis (marker of locally advanced disease)
- Submandibular and jugulodigastric nodes are most commonly involved
- Bilateral nodal involvement can occur with midline-extending tumours
- The relatively scant lymphatic supply explains why nodal disease is a late feature
4. Distant (Haematogenous) Spread
Distant metastases are uncommon at presentation. They occur in:
- ~20% of adenocarcinomas
- ~10% of squamous cell carcinomas
- Usually associated with local recurrence
- Common sites: lungs, liver, bone
Clinical Correlations - Signs Indicating Route of Spread
| Sign / Symptom | Route / Structure Involved |
|---|---|
| Cheek swelling | Lateral wall erosion |
| Nasal obstruction / epistaxis | Medial spread into nasal cavity |
| Epiphora, proptosis, diplopia | Superior spread into orbit |
| Infraorbital anaesthesia / paraesthesia | Infraorbital nerve (V2) involvement |
| Trismus | Posterior spread to pterygoid muscles / infratemporal fossa |
| Loose upper teeth / oro-antral fistula | Inferior spread to alveolus/palate |
| Cervical lymphadenopathy | Regional lymphatic spread (late sign) |
| Headache / CN palsies | Skull base / cavernous sinus extension |
Summary Points for 10-mark Answer
- Maxillary carcinoma spreads in six directions - medial, lateral, superior, inferior, posterior, and posterosuperior
- Ohngren's line separates suprastructure (worse prognosis) from infrastructure tumours
- Only 25% are confined to the antrum at presentation - late presentation is characteristic
- Perineural spread (especially along V2 and greater palatine nerve) is a route to skull base
- Lymph node metastasis is relatively late (10% at presentation); submandibular and jugulodigastric nodes are first involved; retropharyngeal nodes drain the posterior pathway
- Trismus = posterior spread (pterygoids); infraorbital paraesthesia = nerve involvement; proptosis = orbital invasion
- Distant metastases are uncommon and more frequent in adenocarcinoma than SCC
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery; Bailey and Love's Short Practice of Surgery, 28th ed.; Cummings Otolaryngology Head and Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.