ECG change with their image and treatment
Reading File
Finding Sources
Finding Sources
Searching Images
ECG changes ST elevation MI STEMI
Reading File
Finding Sources
Searching Images
ECG atrial fibrillation LBBB heart block Wolff-Parkinson-White
Finding Sources
Searching Images
ECG ventricular tachycardia ventricular fibrillation heart block complete
Searching Images
ECG hyperkalemia hypokalemia QT prolongation electrolyte changes
Searching Images
normal sinus rhythm ECG P wave QRS T wave labeled diagram
Searching Images
ECG pericarditis saddle shaped ST elevation diffuse PR depression
I now have rich image data and clinical content. Let me compile the comprehensive ECG guide.
ECG Changes: Patterns, Images & Treatment
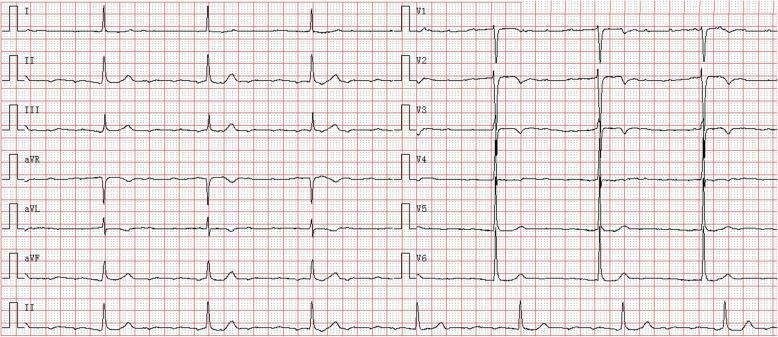
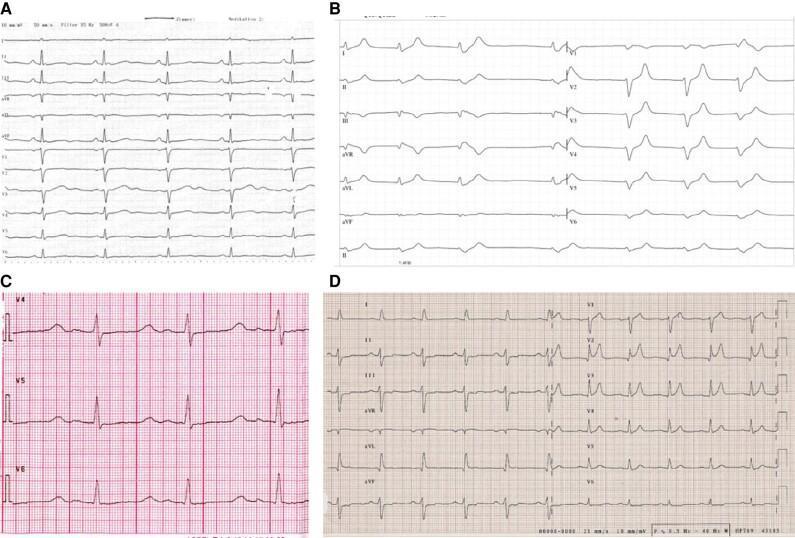
🫀 Normal Sinus Rhythm (Reference)
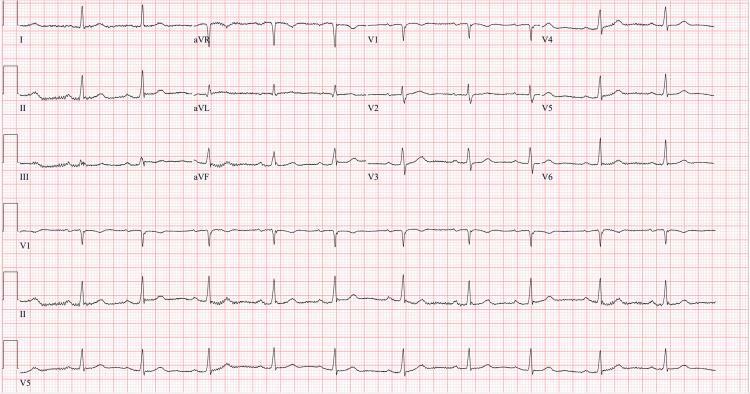
ECG features: Regular P before every QRS, PR interval 120–200 ms, QRS < 120 ms, isoelectric ST segments, upright T waves in I, II, V4–V6.
1. STEMI — Inferior Wall (RCA territory)
ECG features:
- ST elevation ≥1 mm in leads II, III, aVF
- Reciprocal ST depression in I and aVL
- May show early hyperacute T waves
Treatment:
- Primary PCI within 90 minutes of first medical contact (door-to-balloon < 90 min)
- Antiplatelet: Aspirin 325 mg loading + P2Y12 inhibitor (ticagrelor or prasugrel preferred over clopidogrel)
- Anticoagulation: UFH, bivalirudin, or enoxaparin
- If PCI unavailable within 120 min: fibrinolysis (tenecteplase/alteplase)
- Beta-blocker (within 24 h if hemodynamically stable), ACE inhibitor, high-intensity statin
- Monitor for RV infarction (right-sided leads; avoid nitrates if RV involvement)
2. STEMI — Anterior Wall (LAD territory)
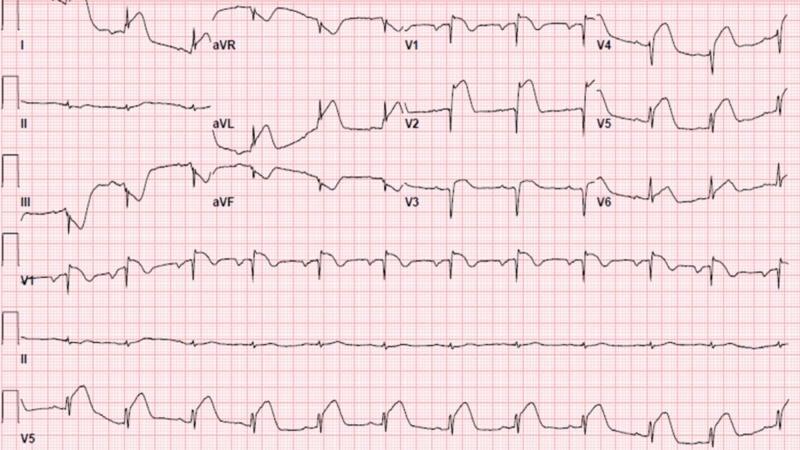
ECG features:
- ST elevation in V1–V4 (convex/"tombstone" morphology)
- Hyperacute T waves in V2–V4
- Reciprocal ST depression in II, III, aVF
- Loss of R-wave progression → pathological Q waves (later)
Treatment: Same STEMI protocol as above. Proximal LAD occlusion carries highest mortality risk; early PCI is critical. ACE inhibitor mandatory for anterior MI + reduced EF.
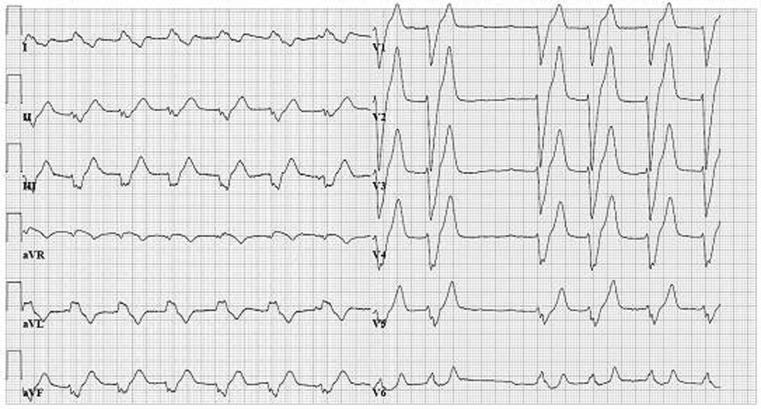
3. Anterolateral STEMI

ECG features:
- ST elevation across V1–V6, I, and aVL
- Hyperacute peaked T waves V2–V4
- Reciprocal depression in II, III, aVF
- Often proximal LAD occlusion
Treatment: Urgent PCI; consider intra-aortic balloon pump or mechanical support if cardiogenic shock develops.
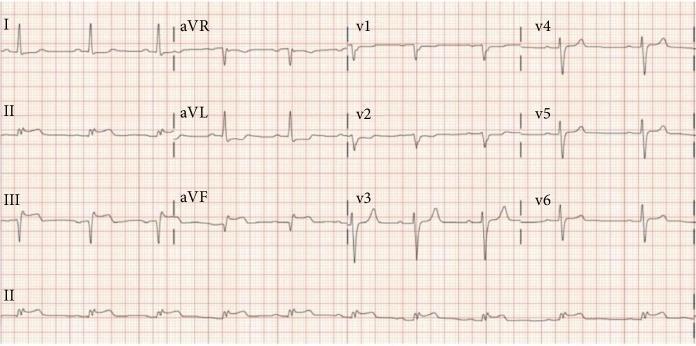
4. NSTEMI / UA (Non-ST Elevation ACS)
ECG features:
- ST depression (horizontal or downsloping) ± T-wave inversion
- No ST elevation, no new LBBB
- Symmetric deep T inversions in V1–V4 = Wellens' pattern (critical LAD stenosis)
Treatment:
- Risk stratify with GRACE/TIMI score
- Dual antiplatelet + anticoagulation
- Early invasive strategy (angiography < 24–72 h) for high-risk features
- Troponin-positive → treat as NSTEMI; admit, IV heparin, beta-blocker, statin
5. Atrial Fibrillation (AF)
ECG features:
- Irregularly irregular RR intervals
- No discernible P waves — replaced by fibrillatory (f) waves
- Narrow QRS unless aberrant conduction or accessory pathway
Treatment:
- Rate control: beta-blockers (metoprolol), non-DHP CCBs (diltiazem, verapamil), digoxin in HFrEF
- Rhythm control: electrical cardioversion (if < 48 h onset or anticoagulated ≥ 3 weeks), flecainide/propafenone (no structural disease), amiodarone (structural disease), ablation
- Anticoagulation: CHA₂DS₂-VASc ≥ 2 (men) or ≥ 3 (women) → DOAC (apixaban, rivaroxaban, dabigatran preferred over warfarin)
- Treat precipitating causes (thyrotoxicosis, infection, alcohol)
6. Wolff-Parkinson-White (WPW) Syndrome
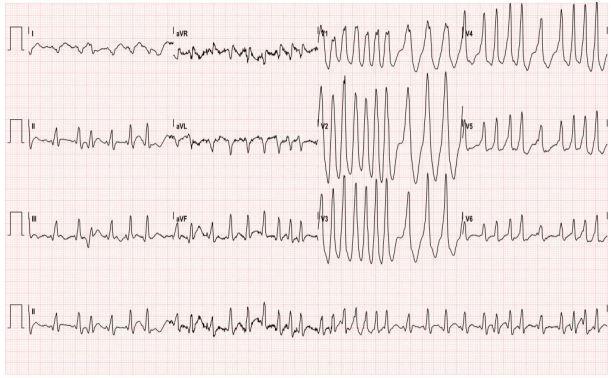
ECG features (sinus rhythm):
- Short PR < 120 ms
- Delta wave (slurred QRS upstroke)
- Widened QRS
Pre-excited AF (shown above): Very rapid (>200 bpm), irregularly irregular, wide bizarre QRS — life-threatening emergency.
Treatment:
- Pre-excited AF (WPW + AF): AVOID AV-nodal blockers (adenosine, digoxin, verapamil, diltiazem — may accelerate conduction → VF)
- Drug of choice: Procainamide IV or electrical cardioversion
- Definitive: Radiofrequency catheter ablation of accessory pathway (curative)
7. Complete (3rd-Degree) AV Block
ECG features:
- Complete AV dissociation — P waves and QRS complexes march through independently
- Slow escape rhythm (ventricular: 20–40 bpm; junctional: 40–60 bpm)
- Wide QRS if ventricular escape; narrow if junctional (Hisian)
Treatment:
- Atropine 0.5–1 mg IV (temporary, mainly for junctional escape)
- Transcutaneous pacing (emergency bridge)
- Transvenous temporary pacing → definitive permanent pacemaker implantation
- If caused by inferior MI (usually RCA): may be transient; monitor; pace if symptomatic
8. Ventricular Tachycardia (VT) vs. Normal Sinus Rhythm

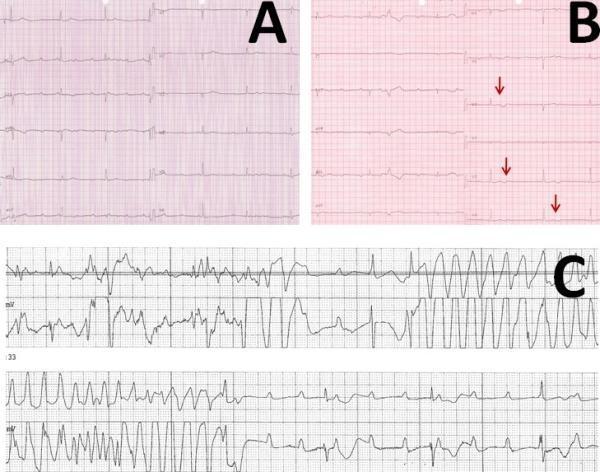
ECG features of VT:
- Wide QRS (> 120 ms), rate 100–250 bpm, regular
- AV dissociation, fusion beats, capture beats
- Monomorphic = uniform QRS; Polymorphic = varying QRS (including Torsades de Pointes)
Treatment:
- Stable VT: Amiodarone 150 mg IV bolus; lidocaine as alternative
- Unstable VT / pulseless VT: Immediate unsynchronized DC shock (200 J biphasic)
- Torsades de Pointes: IV Magnesium sulfate 2 g bolus; correct hypokalemia; stop QT-prolonging drugs; temporary overdrive pacing
- Underlying cause: treat ischemia, electrolytes, drug toxicity
- Long-term: ICD if structural heart disease + EF < 35%
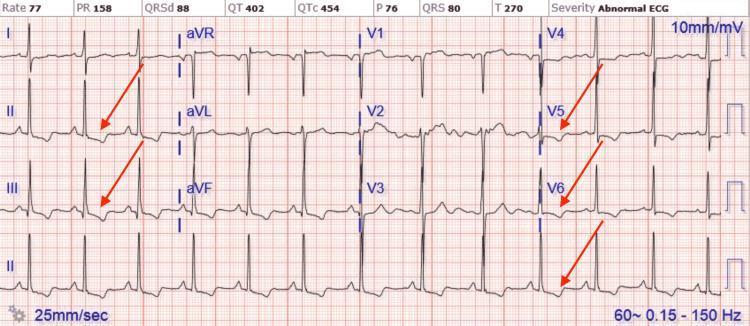
9. Acute Pericarditis

ECG features:
- Diffuse concave ("saddle-shaped") ST elevation in multiple leads (I, II, aVF, V2–V6)
- PR-segment depression (most visible in lead II) — pathognomonic
- Reciprocal ST depression and PR elevation in aVR
- Spodick's sign: downsloping TP segment
- No reciprocal changes matching a single coronary territory (distinguishes from STEMI)
Treatment:
- First-line: NSAIDs (ibuprofen 600 mg TID or aspirin 750–1000 mg TID) + Colchicine 0.5 mg BD × 3 months (reduces recurrence by ~50%)
- Restrict physical activity until symptom-free + CRP normalized
- Avoid glucocorticoids (first-line) — increase recurrence
- Steroids reserved for: autoimmune pericarditis, contraindication to NSAIDs, refractory cases
10. Electrolyte Disturbances
Hyperkalemia & Hypokalemia — All Stages
| Electrolyte | ECG Change | Treatment |
|---|---|---|
| Hyperkalemia | Peaked ("tented") T waves → wide QRS → sine wave → VF | Calcium gluconate (membrane stabilize), insulin + dextrose, salbutamol, kayexalate, dialysis |
| Hypokalemia | Flat/inverted T waves, U waves, prolonged QU, ST depression | Oral/IV potassium replacement; correct hypomagnesemia |
| Hypocalcemia | Prolonged ST segment → long QT | IV calcium gluconate; correct vitamin D deficiency |
| Hypercalcemia | Shortened QT interval, short ST segment | IV saline hydration, furosemide, bisphosphonates, treat underlying cause |
Quick Reference Summary
| ECG Pattern | Key Finding | Urgent Action |
|---|---|---|
| Inferior STEMI | STE II, III, aVF | Primary PCI < 90 min |
| Anterior STEMI | STE V1–V4 | Primary PCI < 90 min |
| NSTEMI/UA | ST depression, T inversion | Risk stratify; early angiography |
| AF | Irregularly irregular, no P waves | Rate/rhythm control; anticoagulate |
| WPW pre-excited AF | Very rapid irregular wide QRS | Procainamide; NO AV nodal blockers |
| Complete AV block | AV dissociation, escape rhythm | Pacemaker |
| VT | Wide regular tachycardia | Amiodarone or DC shock |
| Torsades de Pointes | Twisting polymorphic VT | Mg²⁺ sulfate IV |
| Pericarditis | Diffuse saddle ST, PR depression | NSAIDs + colchicine |
| Hyperkalemia | Peaked T → sine wave | CaCl₂ + insulin/dextrose |
| Hypokalemia | U waves, flat T | KCl replacement |
This is a shared conversation. Sign in to Orris to start your own chat.